Page 1 of 30
PH10.{1-2,13} | PH10.{1-2,13} | Drug Information Appraisal and Promotional Literature Critique — SDL Guide — SDL Guide
Learning Objectives
- Compare and contrast primary, secondary, and tertiary sources of drug information with their respective strengths and limitations
- Perform a structured critical appraisal of a drug promotional brochure, package insert, or clinical trial report using bias and statistical literacy frameworks
- Demonstrate a professional approach to pharmaceutical representative interactions that maximises authentic information while resisting promotional bias
INSTRUCTIONS
Every day, prescribers are bombarded with drug information from sales representatives, journal advertisements, conference symposia, social-media posts, and online tools — not all of it accurate or complete. A prescriber who cannot critically appraise the source and quality of drug information is vulnerable to prescribing errors, cost escalation, and patient harm. This module equips you with a systematic framework for classifying and evaluating drug information sources and for conducting a structured appraisal of promotional literature — skills the WHO Guide to Good Prescribing identifies as foundational to rational pharmacotherapy.
References
- WHO Guide to Good Prescribing, WHO/DAP/94.11 (guideline)
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 1 (Drug information sources) (textbook)
- NMC Competency-Based Curriculum 2024 — PH10.1, PH10.2, PH10.13 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are a junior resident. A pharmaceutical representative visits your ward, presents a glossy brochure for a new antibiotic, and claims it has 'twice the cure rate' of existing options. The brochure cites one internal company study. Your consultant asks you to verify this claim before the drug is added to the ward protocol. Where do you start — and how do you decide if the claim is trustworthy?
WHY THIS MATTERS
The ability to critically appraise drug information is not an academic exercise — it directly protects patients. Pharmaceutical promotion is a $30-billion global industry, and studies consistently show that prescribers who rely on promotional sources without cross-referencing independent evidence prescribe more expensive, newer, and occasionally more hazardous drugs than those who primarily consult independent references. In India, the NMC Competency-Based Curriculum mandates that medical graduates demonstrate skill in evaluating promotional literature (PH10.2) and managing pharmaceutical representative interactions professionally (PH10.13) precisely because these skills determine the quality and rationality of real-world prescribing decisions throughout a doctor's career.
RECALL
You have previously encountered the concept of evidence hierarchy from community medicine — with systematic reviews and randomised controlled trials sitting above case reports and expert opinion. You also recall that a p-value below 0.05 is conventionally taken as statistically significant, though you may not yet have linked these concepts explicitly to drug information appraisal. In this module, we build on those foundations to apply evidence quality evaluation directly to the clinical decision of whether to trust and use a piece of drug information.
The Drug Information Landscape: Why Sources Matter
Every prescribing decision is an information decision. When you choose amoxicillin over azithromycin for community-acquired pneumonia in a young adult, you are implicitly weighing information from guidelines, textbooks, clinical experience, and perhaps recent trial reports. The quality and independence of these sources critically shapes whether that decision is rational and safe.
The contemporary drug information environment is characterised by information overload and deliberate promotional pressure. A 2013 survey in PLOS Medicine found that pharmaceutical company-funded studies were significantly more likely to report favourable outcomes than independently funded studies — a phenomenon called publication bias. Meanwhile, the sheer volume of medical literature makes it impossible to read everything: PubMed alone indexes more than a million new citations each year.
This creates a three-pronged challenge for the prescriber:
1. Source selection — which source is most appropriate for the specific clinical question (new drug mechanism? dosing in renal failure? drug interaction? cost comparison?)
2. Quality evaluation — is the information credible, independent, and methodologically sound?
3. Currency — is the information up-to-date, or has it been superseded by newer evidence?
Recognising these challenges is the first step in building the critical appraisal habit that separates a safe, rational prescriber from one who simply follows the loudest information channel.
Taxonomy of Drug Information Sources: Primary, Secondary, Tertiary
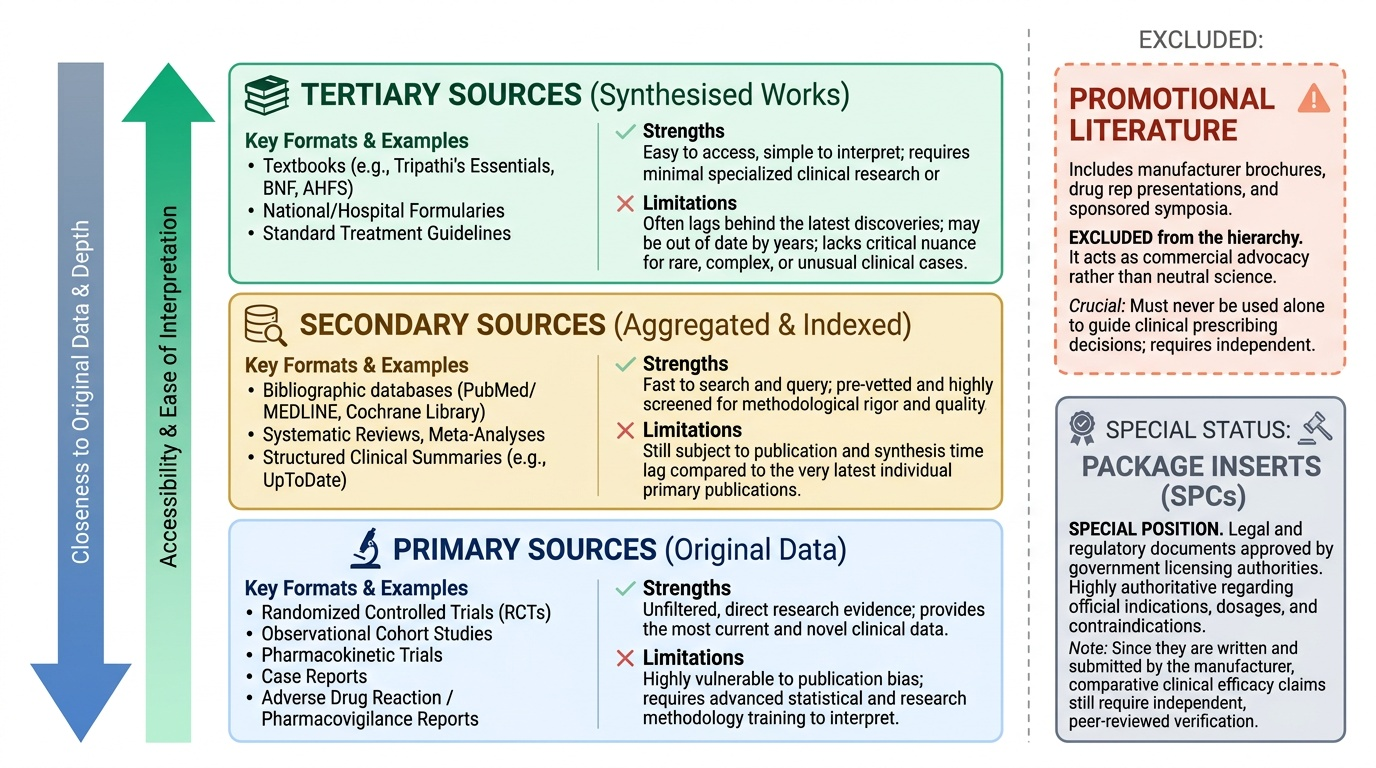
Drug information sources are conventionally classified into three tiers based on how close they are to the original data — a classification that predicts both their depth and their risk of distortion.
Primary sources are original research outputs: randomised controlled trials (RCTs), observational cohort studies, pharmacokinetic studies, case reports, and pharmacovigilance adverse drug reaction reports. They provide the most direct evidence but require the reader to have methodological literacy to evaluate them — and are vulnerable to publication bias (negative trials are less likely to be published).
Secondary sources aggregate and index primary literature. They include bibliographic databases (PubMed/MEDLINE, the Cochrane Library), systematic reviews, meta-analyses, and structured summaries (UpToDate, Clinical Evidence). They are faster to search and pre-screened for quality but may lag behind the most recent publications.
Tertiary sources are synthesised, processed works: standard pharmacology textbooks (Tripathi's Essentials of Medical Pharmacology, BNF, AHFS Drug Information), formularies (National Essential Medicines List, hospital formularies), and standard treatment guidelines. They are most accessible and require least methodological knowledge to use, but may be years out of date by publication and lack nuance for unusual cases.
IMPORTANT: Promotional literature (company brochures, drug representative detailing, conference symposia sponsored by manufacturers) is intentionally excluded from the three-tier classification. It is not a neutral information source — it is advocacy for a commercial product. This does not mean it cannot contain accurate information, but it must never be used as a primary source for prescribing decisions without independent cross-referencing.
IMPORTANT: Package inserts (prescribing information / Summary of Product Characteristics) occupy a special position: they are regulatory documents approved by the licensing authority and contain mandatory safety information, but they are written and submitted by the manufacturer. They are authoritative on licensing status and contraindications as approved, but their clinical comparison claims require verification against independent sources.
Provided image
SELF-CHECK
A colleague wants to quickly check the recommended dose of metformin for a patient with stage 3b CKD (eGFR 35 mL/min). Which source would give the MOST reliable, current, and accessible dosing guidance?
A. A) The drug company's promotional brochure for metformin
B. B) A systematic review on metformin from 2009
C. C) An up-to-date clinical reference such as BNF or UpToDate under 'metformin — renal impairment'
D. D) A pharmacology textbook chapter on biguanides
Reveal Answer
Answer: C. C) An up-to-date clinical reference such as BNF or UpToDate under 'metformin — renal impairment'
C is correct. For a specific clinical decision about dosing in renal impairment, a frequently-updated tertiary clinical reference (BNF, UpToDate) is most appropriate — it synthesises the latest data and regulatory guidance. A promotional brochure has commercial bias. A 2009 systematic review may be outdated given the revised SGLT2i and metformin renal guidance issued after 2015. A textbook chapter may not reflect the most recent prescribing information updates.
Critical Appraisal Framework for Drug Literature
Critical appraisal is the structured process of evaluating drug information for its validity, relevance, and clinical significance. It applies whether you are reading a primary RCT, a meta-analysis, or a promotional brochure — the questions differ in emphasis but share a common architecture. The WHO Guide to Good Prescribing and the AGREE framework both emphasise that the ability to appraise clinical literature is a core competency for every prescriber, not just researchers.
The critical appraisal process for drug information has four stages:
Stage 1 — PICO Framing. Before evaluating any source, clarify what you are asking: Patient/Population (who?), Intervention (which drug?), Comparator (vs what?), and Outcome (what matters — symptom relief? mortality? laboratory endpoint?). Many promotional claims fail at this stage because they compare a new drug against placebo rather than against the existing standard treatment.
Stage 2 — Study Design and Bias Assessment. The higher the study design on the evidence hierarchy, the lower the risk of systematic error. Key biases to identify:
- Selection bias: were the trial participants representative of your patients? (e.g. elderly patients, those with comorbidities, and women are frequently underrepresented in drug trials)
- Performance bias: were participants and assessors blinded to treatment allocation?
- Publication bias: is the literature you are reading a selection of all trials conducted — specifically, is it weighted toward positive results?
- Funding bias: industry-funded studies have a higher odds ratio for producing pro-industry results in meta-analyses
- Outcome reporting bias: were all pre-specified outcomes reported, or only those that were favourable?
Stage 3 — Statistical Literacy. Even a methodologically sound trial can be presented in a statistically misleading way:
- Relative risk reduction (RRR) always sounds large: a drug that reduces event rate from 4% to 2% has an RRR of 50%, but an absolute risk reduction (ARR) of only 2%
- Number needed to treat (NNT) = 1/ARR: in the above example, NNT = 50 — you must treat 50 patients to prevent one event
- Number needed to harm (NNH) applies the same calculation to adverse events — allows comparison of benefit-risk
- A statistically significant result (p<0.05) may lack clinical significance if the effect size is small
- Confidence intervals (CI): a wide CI spanning 1.0 for a risk ratio means the result is uncertain even if significant
Stage 4 — Conflict of Interest and Applicability. Identify who funded the study, whether there are author conflicts of interest, and whether the trial population and setting are applicable to your patients (Indian patients, resource-limited settings, differing baseline risk).
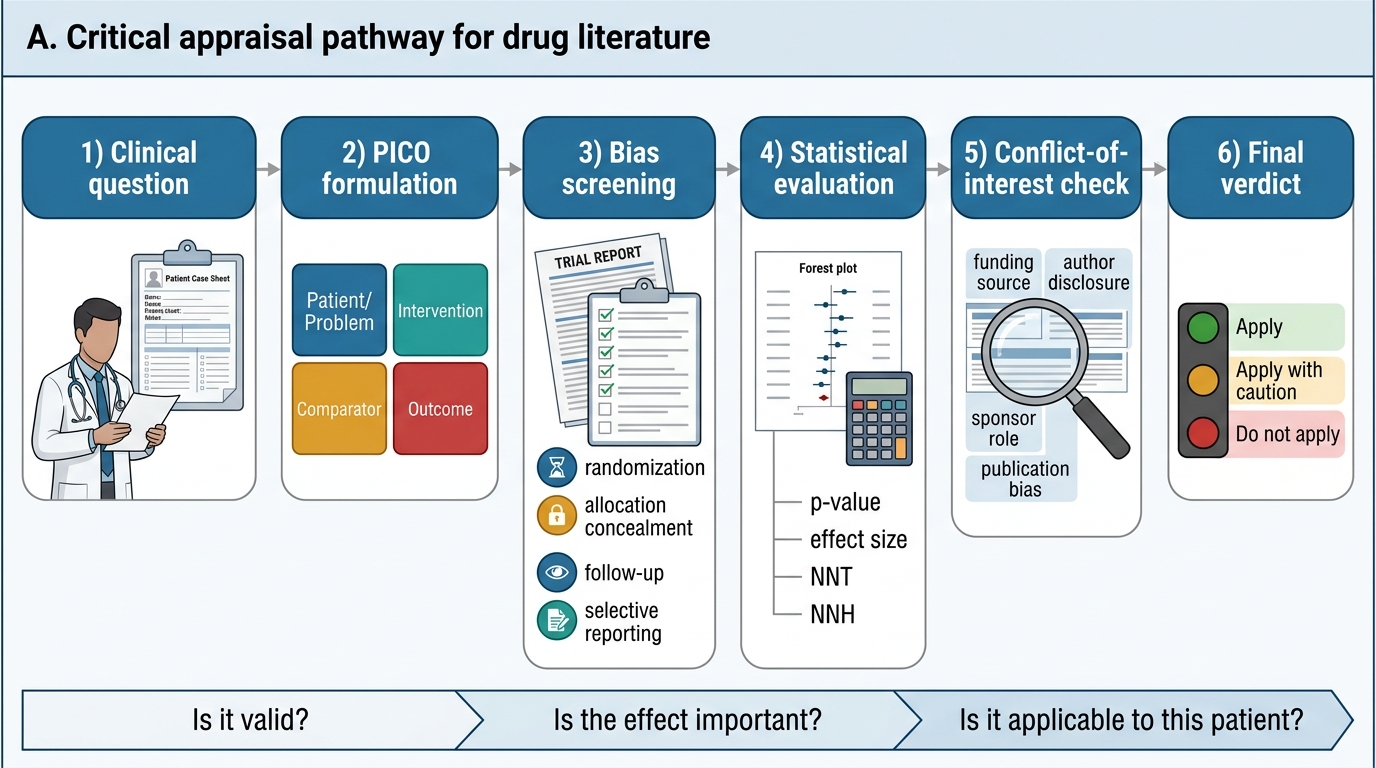
Critical Appraisal Pathway for Drug Literature