Page 20 of 30
PH10.{14-15,17} | PH10.{14-15,17} | Patient Communication, Adherence and Public Drug Education — SDL Guide — SDL Guide (Part 2)
Adherence: Determinants, Assessment, and Methods to Improve
Adherence (the preferred, non-paternalistic term replacing 'compliance') is defined by WHO as 'the extent to which a person's behaviour — taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.' The word 'agreed' is important: adherence is a collaborative, not a directive, concept.
Non-adherence is classified as:
- Intentional: the patient consciously decides not to take the medication — typically from side-effect concerns, cost, lack of perceived benefit, or distrust
- Unintentional: the patient wants to adhere but cannot — due to forgetting, misunderstanding instructions, regimen complexity, or cognitive impairment
The two types require different interventions: intentional non-adherence needs motivational work and shared decision-making; unintentional non-adherence needs simplification and reminder systems.
WHO multidimensional adherence model — five factor domains:
1. Socioeconomic factors: poverty, cost of medication, distance to pharmacy, illiteracy, unstable housing — directly constrain adherence regardless of patient motivation
2. Health system factors: quality of patient-prescriber relationship, continuity of care, waiting times, drug availability at the dispensing point
3. Condition-related factors: asymptomatic conditions (hypertension, hyperlipidaemia) have much lower adherence than symptomatic ones; depression and cognitive impairment reduce adherence
4. Therapy-related factors: number of drugs (polypharmacy), dosing complexity (frequency, timing requirements with food), side effects, formulation (liquid vs tablet vs injectable)
5. Patient-related factors: beliefs about medication ('natural' vs 'chemical'), health literacy, self-efficacy, social support
Assessment tools:
The Morisky Medication Adherence Scale (MMAS-8) is a validated 8-item self-report questionnaire assessing adherence behaviour over the past 2 weeks. A score of <6 indicates low adherence; 6–7 medium; 8 high. It is primarily a screening tool — elevated risk detected should lead to an adherence-focused consultation, not automatic dose escalation.
Simpler clinical approaches include: asking non-judgementally ('Many people find it difficult to take their tablets every day — how often do you take yours?'); pill counting at review; pharmacy refill records.
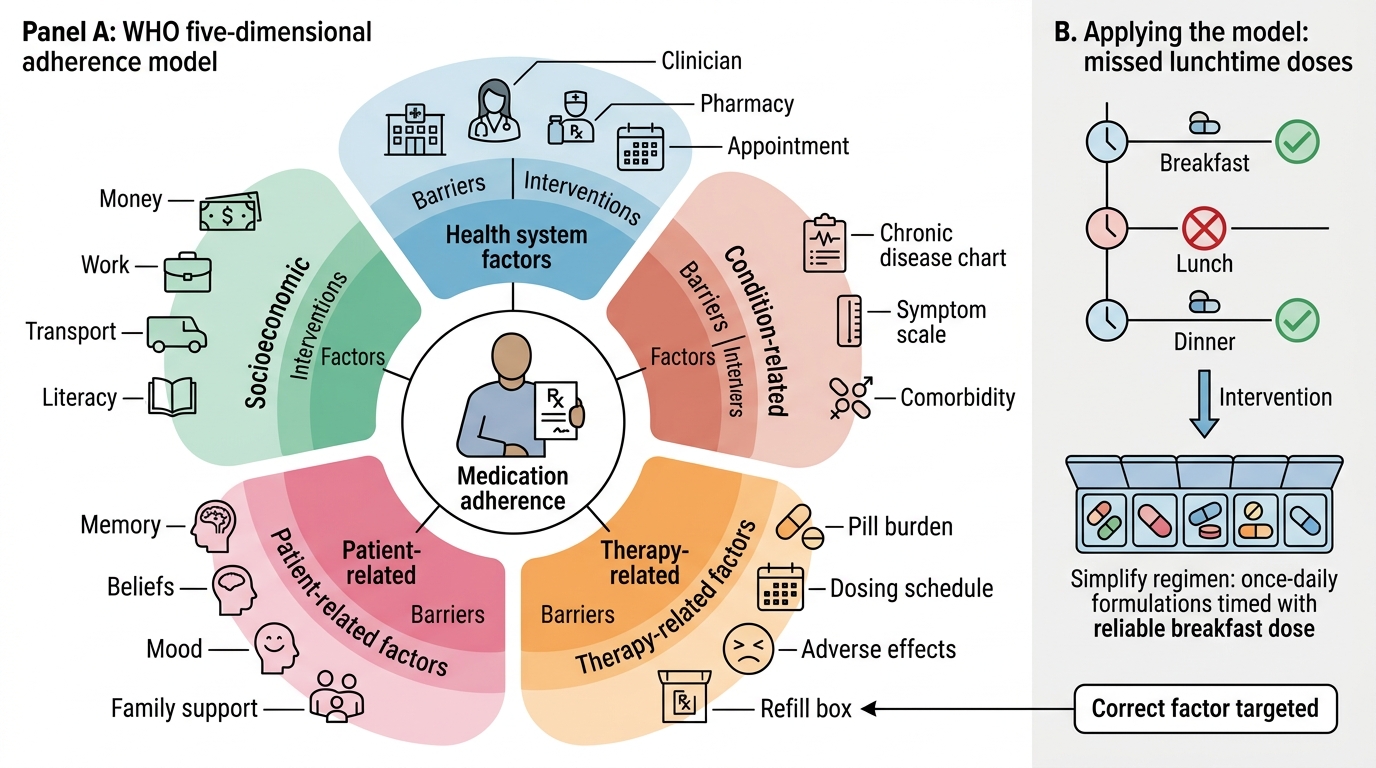
WHO Five-Dimension Model of Medication Adherence
SELF-CHECK
A 55-year-old man with hypertension and type 2 diabetes on four medications misses 40% of his doses. He says he 'forgets, especially at lunch.' He takes breakfast and dinner medications reliably. What is the MOST appropriate adherence-improvement strategy for this patient?
A. A) Switch all medications to once-daily formulations timed with a dose he reliably takes (e.g. breakfast)
B. B) Add a fifth medication to compensate for the missed doses
C. C) Discharge him from the clinic for non-compliance
D. D) Prescribe an electronic pill dispenser regardless of cost
Reveal Answer
Answer: A. A) Switch all medications to once-daily formulations timed with a dose he reliably takes (e.g. breakfast)
A is correct. The patient has unintentional non-adherence (forgets the lunchtime dose) and reliable adherence to breakfast and dinner medications. The evidence-based approach is simplification: switch to once-daily formulations (if clinically appropriate equivalents exist) and consolidate all doses to the breakfast time slot — reducing the regimen from three daily timings to one. This is therapy-related factor intervention. Option B escalates regimen complexity — the opposite of the required intervention. Option C abandons the patient. Option D (electronic dispensers) may help but cost and practicality are barriers; simplification is the first-line intervention.
Motivating Patients with Chronic Diseases: Applied Strategies
Motivating patients with chronic disease to maintain long-term adherence requires more than information delivery — it requires an understanding of what drives health behaviour change. The evidence base points to several effective strategies.
Motivational Interviewing (MI):
Motivational interviewing is a collaborative, person-centred communication style for strengthening a person's motivation for and commitment to change. It has RCT evidence for improving adherence in HIV, cardiovascular disease, and diabetes. The core principles are:
- Express empathy (understand and reflect the patient's perspective without judgment)
- Develop discrepancy (help the patient explore the gap between their current behaviour and their stated values/goals — 'You told me you want to see your grandchildren grow up. How does stopping your blood pressure tablet connect with that goal?')
- Roll with resistance (do not argue against resistance — explore it: 'Tell me more about what concerns you about taking this medication long-term')
- Support self-efficacy (reinforce the patient's belief that they can change — 'You successfully stopped smoking two years ago — that's exactly the kind of determination that helps manage diabetes')
Shared decision-making:
For patients with genuine reservations about a medication, shared decision-making — providing transparent information about options, expected benefits and harms, and eliciting the patient's values and preferences — produces better adherence than a directive approach. A patient who chooses a medication with full understanding is more likely to take it than one who is instructed to.
Practical strategies by barrier type:
| Barrier | Strategy | Example |
|---|---|---|
| Forgetfulness | Link to daily routine; pill box; phone alarm | 'Can you keep your tablet next to your toothbrush?' |
| Cost | Generic substitution; Jan Aushadhi; partial regimen | Calculate patient's drug spend; offer NLEM alternatives |
| Side effects | Anticipate and pre-empt; dose timing adjustment | 'Nausea from metformin usually improves — try taking it with the largest meal' |
| Lack of perceived benefit | Explain mechanism and long-term risk | 'Your BP feels normal because the tablet is working — stopping it would let the pressure rise again' |
| Complexity | Simplify regimen; once-daily formulations | 'Can we reduce to one morning pill by combining these?' |
| Negative beliefs | Explore and address specifically | 'What have you heard about these tablets affecting the kidneys?' |
Public Drug Education: Communicating Beyond the Clinic
The prescriber's communication responsibility extends beyond the individual patient encounter. As a trained healthcare professional, you have both the knowledge and the social authority to educate patients, families, and communities about drug-related public health issues. Three areas are particularly important for the Indian context.
Drug dependence education:
India faces a significant and growing burden of substance dependence — alcohol, opioids, benzodiazepines, cannabis, and prescription drug misuse are all prevalent. The prescriber's role includes:
- Routinely screening for substance misuse in relevant patient populations (CAGE questionnaire for alcohol; AUDIT; DAST for drugs)
- Counselling patients receiving potentially dependence-producing medications (opioids, benzodiazepines — see the Cautious Prescribing SDL for this cluster) about the risk of dependence and the planned duration of use
- Educating community members and family members about recognition of dependence and how to access treatment (de-addiction centres, community mental health teams)
Rational OTC use:
In India, the widespread availability of antibiotics, steroids, and NSAIDs without prescription — while technically in violation of Schedule H regulations — is a public health challenge. Patient education topics include:
- Antibiotics do not treat viral infections (common cold, most sore throats, viral diarrhoea) — taking them unnecessarily causes side effects and contributes to resistance
- Steroids (including topical corticosteroids) have significant side effects with prolonged unsupervised use; face creams containing steroids for 'fairness' are a documented harm in India
- Paracetamol: the safe OTC analgesic, but only at the correct dose (max 1g/dose, 4g/day in adults; lower in hepatic disease or heavy alcohol use); acetaminophen toxicity is the commonest cause of acute liver failure in some settings
Social media and drug misinformation:
The COVID-19 pandemic dramatically amplified the problem of drug misinformation — hydroxychloroquine, ivermectin, and other drugs were circulated as cures on social media without evidence. As a prescriber and public health communicator:
- Use accessible social media channels to share accurate information from WHO, NMC, and ICMR sources
- Gently counter misinformation encountered in patient consultations without shaming ('That was widely shared on WhatsApp — let me share what the current evidence actually shows')
- Support health literacy initiatives in your community — a well-informed patient population makes better OTC decisions
CLINICAL PEARL
The teach-back method saves prescribing effort downstream. At the end of every prescription counselling session, ask the patient to tell you in their own words: 'Just to make sure I explained everything clearly — how will you take this tablet?' This question takes 30 seconds and catches misunderstandings before they translate into non-adherence, treatment failure, and more appointments. Research shows teach-back reduces medication errors by 80% in post-discharge medication counselling. It is not a test of the patient's intelligence — it is a check on the prescriber's communication.
Self-Assessment: Patient Communication and Adherence
Apply your communication and adherence skills through these structured exercises before your next clinical session.
Exercise 1 — Drug counselling script:
Write a drug counselling script for a 45-year-old patient starting metformin 500 mg twice daily for newly diagnosed type 2 diabetes. Cover all five elements of the counselling framework.
Model script (abbreviated):
1. Why: 'Metformin lowers your blood sugar by reducing the amount of sugar your liver puts into the blood and by making your body more sensitive to insulin. This reduces your risk of the complications of diabetes — problems with your kidneys, eyes, nerves, and heart — over time.'
2. How: 'One tablet twice a day — take it with or just after your main meals. This reduces the chance of stomach upset. At the same time every day is best — you can set a phone reminder.'
3. Expected effects: 'Your blood sugar will start to improve within 1–2 weeks, but you may not feel any different day to day. The effect builds over months. Unlike some other diabetes tablets, metformin rarely causes low blood sugar (hypoglycaemia) by itself.'
4. Alerts: 'In the first few weeks, some people get nausea, diarrhoea, or a metallic taste — take it with food and start low if these are bothersome. These usually settle within 4 weeks. If you are ever having a procedure with contrast dye (X-ray dye), let the radiologist know you take metformin — they may ask you to hold it before and after the scan.'
5. Return: 'Return in 3 months for a blood sugar check and a kidney function test. See your doctor sooner if you develop symptoms I have not mentioned.'
Exercise 2 — Adherence consultation:
A 68-year-old woman has been on four antihypertensives for 3 years. Her BP at today's visit is 165/100 despite what appears to be an adequate regimen. On MMAS-8 screening she scores 4 (low adherence). She says 'I sometimes feel dizzy and I am not sure the tablets are helping.' Design an adherence-focused consultation plan.
Model plan: (1) Explore the dizziness — is it postural (drug effect) or a separate symptom? If postural hypotension, simplify the regimen or reduce dose of offending agent. (2) Address lack of perceived benefit: explain that hypertension is asymptomatic by design — the tablet is working if BP is lower; show her the measurement difference. (3) MMAS-8 follow-up: ask about the specific items she scored on — is it forgetting (unintentional) or choosing not to take (intentional)? (4) If forgetfulness: simplify to once-daily formulations; (5) If concerns about long-term use: explore and address the specific belief. (6) Schedule 4-week follow-up with BP measurement and MMAS-8 repeat to track improvement.