Page 22 of 30
PH10.16 | PH10.16 | Cautious Prescribing for Dependence-Producing Drugs — SDL Guide — SDL Guide
Learning Objectives
- Demonstrate an understanding of the pharmacology of dependence, including tolerance, physical dependence, and addiction for major drug classes (opioids and benzodiazepines)
- Apply a framework for cautious prescribing of dependence-producing drugs, including indication screening, dose minimisation, duration limitation, and monitoring
- Recommend an appropriate line of management for a patient presenting with features of opioid or benzodiazepine dependence
INSTRUCTIONS
The same drugs that relieve severe cancer pain, terminate seizures, and manage acute anxiety also have the potential to generate dependence when prescribed incautiously, for too long, or to patients without a genuine therapeutic indication. Prescription-drug misuse is a growing clinical problem in India — benzodiazepine dependence in middle-aged women, opioid diversion from palliative prescriptions, and tramadol misuse in young men are documented in Indian epidemiological literature. This module builds the framework for cautious prescribing that permits appropriate therapeutic use while protecting patients from iatrogenic harm.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 33 (Opioid analgesics), Ch 31 (Anxiolytics/hypnotics — dependence) (textbook)
- NDPS Act 1985 (Narcotic Drugs and Psychotropic Substances Act, India) (legislation)
- WHO Guidelines on the Pharmacological Treatment of Persisting Pain in Adults with Medical Illnesses, 2012 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old accountant presents for a prescription renewal of alprazolam 0.5 mg twice daily. He has been on this for 18 months, originally prescribed for 'work-related stress' by a colleague. He now says he cannot function without it and gets 'unbearable anxiety and shaking' if he misses a dose. He has already been to two other doctors who refused to renew, and he is asking you as 'the third option.' How do you manage this consultation — and at what point did the prescribing of a legitimate anxiolytic become iatrogenic dependence?
WHY THIS MATTERS
Opioid and benzodiazepine dependence in India is substantially iatrogenic — originating with legitimate medical prescriptions that were either continued too long, given to patients with risk factors for dependence, or not monitored adequately. A 2019 National Drug Dependence Treatment Centre (NDDTC) AIIMS survey found that sedative-hypnotics (principally benzodiazepines) are the second most common class of drugs presenting to de-addiction services in India, largely acquired through prescriptions. Tramadol misuse — often starting with a legitimate orthopaedic or postoperative prescription — has been documented as a significant abuse drug in several Indian states. As a prescriber, you are both a primary preventer of prescription-drug dependence and a critical responder when it occurs.
RECALL
Recall from general pharmacology that tolerance is the pharmacological adaptation in which a progressively larger dose is needed to produce the same effect — it occurs through receptor down-regulation and compensatory changes. Recall also that opioid analgesics act on mu, kappa, and delta opioid receptors; their therapeutic effects (analgesia, cough suppression) and their misuse potential (euphoria, respiratory depression) arise from the same receptor system. Recall from the legal-regulatory SDL that both opioids and benzodiazepines are Schedule X drugs under the NDPS Act, with specific prescription requirements.
Dependence-Producing Drugs in Clinical Practice: The Prescriber's Responsibility
Drug dependence is not a failure of patient willpower — it is a predictable physiological and psychological consequence of sustained exposure to drugs that activate the brain's reward circuitry or produce compensatory physiological adaptations. As a prescriber, you hold significant power in this relationship: your prescription initiates the exposure, your monitoring detects early dependence development, and your clinical judgment determines whether to continue, reduce, or stop the drug.
The prescriber's responsibility for dependence-producing drugs operates on three levels:
1. Prevention: prescribing only when genuinely indicated, at the lowest effective dose, for the shortest necessary duration — and with a clear plan for cessation from the outset
2. Detection: monitoring for features of developing dependence — dose escalation requests, reports of lost or stolen prescriptions, multiple prescriber patterns, withdrawal symptoms on missed doses
3. Management: when dependence is identified, engaging a supervised tapering and/or referral plan rather than abruptly stopping (which precipitates severe withdrawal) or continuing indefinitely
The legal framework is clear: Schedule X drugs require specific prescription formats and are subject to limits on quantity per prescription. These regulations exist precisely to constrain inappropriate prescribing patterns. However, they cannot substitute for clinical judgment — the best protection against prescription drug dependence is a prescriber who understands the pharmacology of dependence and applies it systematically.
Note also that dependence-producing drugs include drugs not routinely thought of in this category: chronic alcohol use, tobacco (nicotine dependence), cannabis (particularly regular high-potency use), and in some patients, gabapentinoids (pregabalin, gabapentin) — all have established dependence profiles and prescribing caution is warranted.
Pharmacology of Dependence: Tolerance, Withdrawal, and Addiction
Precise use of terminology is essential for communicating about drug dependence clinically. Three related but distinct concepts are frequently confused:
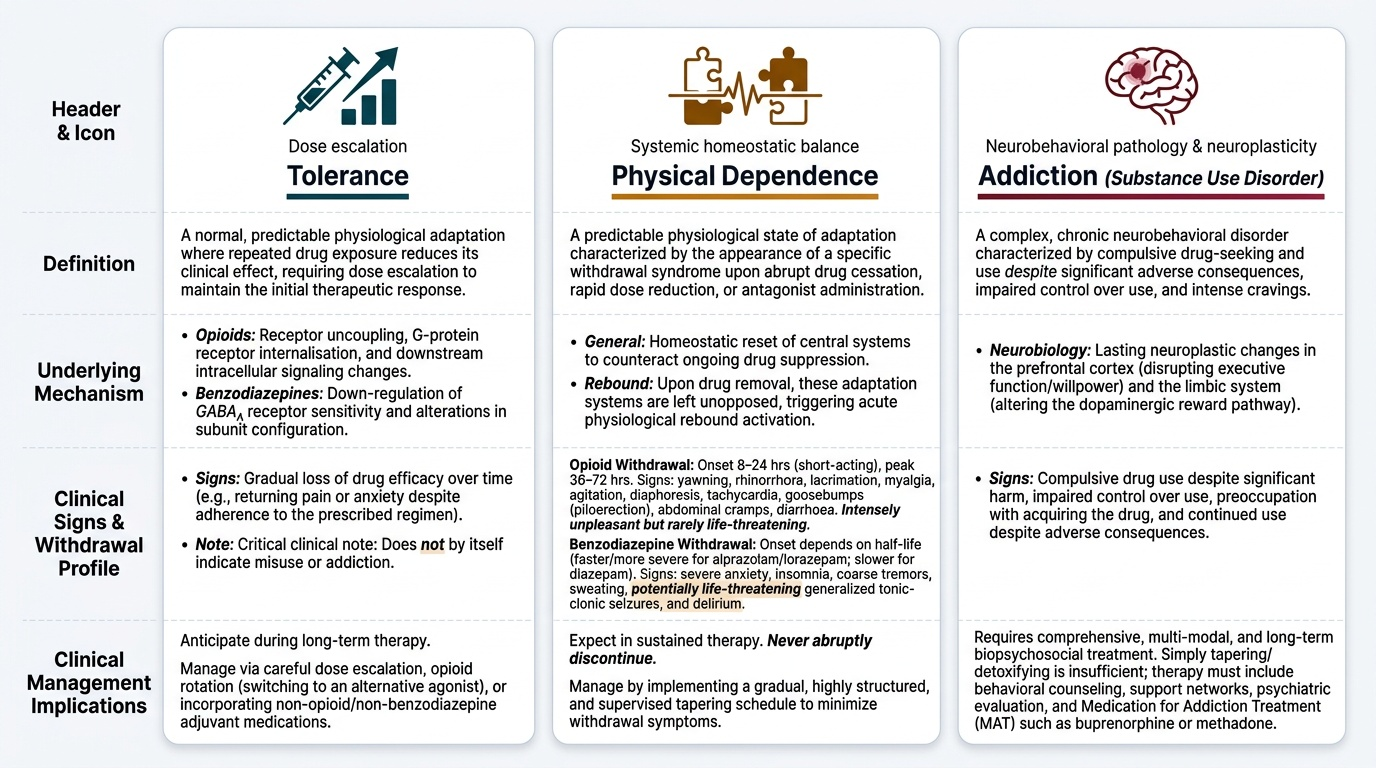
Tolerance: A physiological adaptation in which repeated drug exposure reduces the drug's effect, requiring dose escalation to maintain the same response. The mechanism varies by drug class — for opioids, tolerance involves receptor uncoupling, internalisation, and downstream signalling changes; for benzodiazepines, it involves down-regulation of GABA-A receptor sensitivity. Tolerance is expected in patients on long-term opioid or benzodiazepine therapy and does not by itself indicate misuse or addiction.
Physical dependence: A state in which abrupt discontinuation of the drug produces a withdrawal syndrome — a cluster of physiological and psychological symptoms reflecting rebound activation of systems previously suppressed by the drug. This is also a predictable physiological consequence of sustained use and is distinct from addiction.
- Opioid withdrawal: begins 8–24 hours after last dose (short-acting opioids); symptoms include yawning, rhinorrhoea, lacrimation, myalgia, agitation, piloerection ('goose bumps'), diaphoresis, tachycardia, abdominal cramps, diarrhoea; peaks 36–72 hours; rarely life-threatening (unlike alcohol/benzodiazepine withdrawal) but intensely unpleasant
- Benzodiazepine withdrawal: potentially life-threatening — includes anxiety, insomnia, tremor, sweating, and in severe cases, generalised tonic-clonic seizures and delirium; onset and severity depend on half-life (lorazepam/alprazolam withdrawal is faster and more severe than diazepam withdrawal due to shorter half-life)
Addiction (substance use disorder): A complex neurobehavioral disorder characterised by compulsive drug use despite significant harm; impaired control over use; preoccupation with acquiring the drug; and continued use despite adverse consequences. Addiction involves neuroplastic changes in the prefrontal cortex and limbic system. It is distinct from physical dependence — a cancer patient on long-term morphine who is physically dependent is not necessarily addicted.
Provided image
Major dependence-producing drug categories:
- Opioids (Schedule X NDPS): morphine, codeine, pethidine, fentanyl, buprenorphine, tramadol (Schedule H1) — all mu-opioid receptor agonists with strong physical dependence and addiction potential
- Benzodiazepines (Schedule X): diazepam, alprazolam, lorazepam, clonazepam — GABA-A positive allosteric modulators; strong physical dependence with continued use >4 weeks; Z-drugs (zolpidem, zopiclone) have similar profiles
- Alcohol and tobacco: not scheduled but with profound dependence profiles — alcohol withdrawal can be fatal
SELF-CHECK
A 62-year-old woman with cancer has been on oral morphine 60 mg 12-hourly for 6 months for bone pain control. She requires dose escalation to 80 mg 12-hourly to maintain pain control. The oncology team worries she is 'becoming addicted.' Which statement BEST describes her clinical situation?
A. A) She has developed morphine addiction — the dose escalation is dose-seeking behaviour
B. B) She has developed opioid tolerance (a physiological adaptation causing reduced analgesic effect at the same dose), which requires dose escalation; this is not addiction
C. C) She has developed physical dependence — the dose escalation is due to withdrawal between doses
D. D) Morphine doses above 60 mg/day are always a sign of misuse in non-terminal patients
Reveal Answer
Answer: B. B) She has developed opioid tolerance (a physiological adaptation causing reduced analgesic effect at the same dose), which requires dose escalation; this is not addiction
B is correct. Opioid tolerance is the expected physiological adaptation to sustained opioid use — repeated exposure reduces receptor sensitivity, requiring dose escalation to maintain the same analgesic effect. This is a predictable pharmacological consequence of chronic opioid therapy and does not indicate addiction (which requires compulsive use despite harm, loss of control, and neuroplastic changes in reward circuits). In cancer pain management, dose escalation to maintain pain control is appropriate and is not misuse. Physical dependence means she would experience withdrawal if the drug were abruptly stopped — which is also expected and managed by tapering, not by withholding the drug.
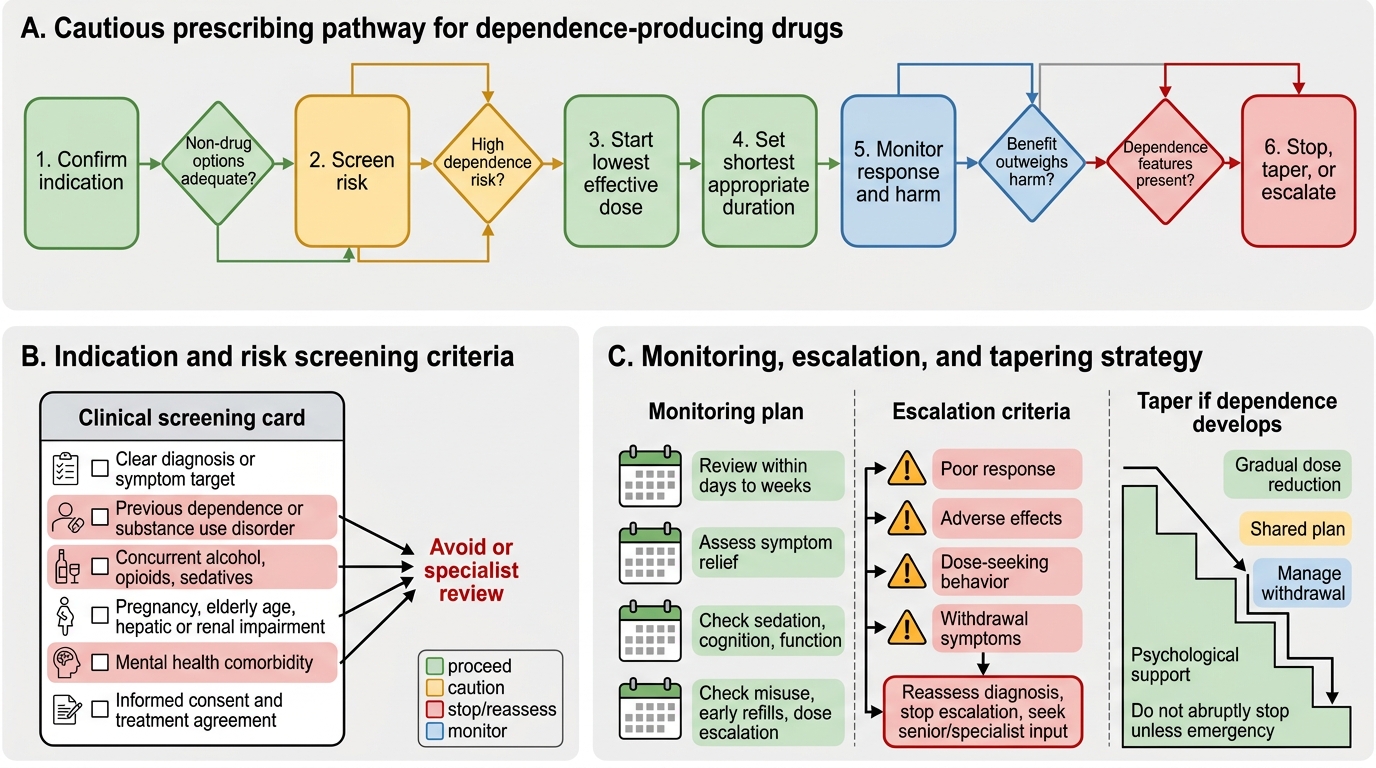
Framework for Cautious Prescribing: Opioids and Benzodiazepines
A systematic framework for cautious prescribing of dependence-producing drugs allows their therapeutic benefits to be realised while minimising the risk of iatrogenic dependence. The framework applies to both opioids and benzodiazepines, with some drug-class-specific considerations.
Step 1 — Indication screening (Is this drug genuinely needed?):
For opioids: Is there objective evidence of pain severity that cannot be managed by non-opioid analgesics (NSAIDs, paracetamol, adjuvants)? Is the pain expected to have a limited duration, or is it chronic (which carries higher dependence risk)? Does the patient have a history of substance use disorder (which dramatically increases dependence risk with any opioid)?
For benzodiazepines: Is this a genuine acute anxiety/insomnia crisis, or a chronic symptom that would be better served by CBT, antidepressants, or social intervention? Has the patient already used benzodiazepines previously (indicating risk of physical dependence)?
Step 2 — Dose minimisation:
Start at the lowest dose that achieves the therapeutic objective. Avoid immediately titrating to higher doses based on patient report alone — assess objectively (pain scores, functional assessment, sleep diary).
Step 3 — Duration limitation:
For benzodiazepines: prescribe for a defined, limited duration — typically 2–4 weeks for acute anxiety/insomnia. Prescriptions beyond 4 weeks require explicit re-evaluation; beyond 3 months, physical dependence is very likely and a tapering plan must be initiated. For acute pain opioids: align duration with expected recovery (7–14 days is appropriate for most acute pain). Document the intended duration explicitly.
Step 4 — Monitoring for aberrant behaviour:
On every renewal request, screen for: dose escalation requests beyond the agreed plan; reports of lost/stolen medications; obtaining the drug from multiple prescribers; using opioids/benzodiazepines for sleep, mood, or anxiety rather than the stated indication; intoxicated presentations; evidence of intravenous use or crushing tablets.
Step 5 — Tapering strategy:
If dependence develops or the drug is being discontinued, never stop abruptly. For benzodiazepines: taper by 10–25% of the dose every 1–2 weeks (or slower for patients on long-term high-dose therapy); a conversion to a long-acting benzodiazepine (diazepam) facilitates smoother tapering due to its longer half-life. For opioids: reduce by 10–20% of the dose per week with close monitoring of pain and withdrawal symptoms.
Cautious Prescribing of Dependence-Producing Drugs