Page 4 of 30
PH10.{3-4,6} | PH10.{3-4,6} | Rational Prescription Writing and Appraisal — SDL Guide — SDL Guide
Learning Objectives
- Apply the WHO six-step prescribing process to prepare a P-drug list for a given clinical condition
- Write a correct, rational, and legible prescription including all mandatory legal elements
- Perform a systematic critical appraisal of a given prescription and suggest evidence-based improvements
INSTRUCTIONS
Prescription writing is one of the most consequential clinical skills a doctor exercises — it converts a diagnosis into a therapeutic action that directly affects patient outcomes. Prescribing errors are the single largest preventable cause of medication harm in hospitals worldwide. The WHO Guide to Good Prescribing, which underpins this module, shows that systematic training in the six-step prescribing process and the P-drug concept measurably reduces prescribing errors. This module takes you through the methodology of rational drug selection, the mandatory elements of a legally compliant prescription in India, and a systematic framework for appraising a given prescription.
References
- WHO Guide to Good Prescribing, WHO/DAP/94.11 — six-step model and P-drug concept (guideline)
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 2 (Rational prescribing) (textbook)
- Drugs and Cosmetics Act 1940 — Schedule H, H1, and X prescription requirements (India) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
During your internal medicine posting, you admit a 55-year-old man with type 2 diabetes and a newly diagnosed uncomplicated lower urinary tract infection. Your senior asks you to prescribe an appropriate antibiotic and write a complete prescription on the hospital pad — 'the whole thing, as if you are the treating doctor.' You look at the blank prescription pad. What do you write first? How do you decide which drug, which dose, for how many days?
WHY THIS MATTERS
Medication errors cause an estimated 1.3 million injuries and 7,000 deaths annually in the United States alone, and Indian surveys of hospital prescriptions consistently show that 20–30% have at least one error — blank fields, illegible handwriting, incorrect doses, or irrational drug choices. As a final-year medical student, you are already expected to draft prescriptions under supervision; as an intern and junior resident, you will write them independently. The WHO P-drug methodology is not theory — studies show that internship cohorts trained in it make significantly fewer prescribing errors than those trained by observation alone. This module operationalises that skill.
RECALL
Recall from your pharmacology foundation year that drugs in India are broadly classified by prescription status: over-the-counter (OTC) drugs available without prescription, Schedule H drugs (requiring a physician's prescription and not stocked openly), and Schedule X drugs (narcotics, psychotropics) requiring a special prescription format. Recall also that most drugs have both a generic name (International Non-proprietary Name, INN) and one or more brand names assigned by manufacturers — and that prescribing by generic name is the standard recommended by WHO, the National List of Essential Medicines, and NMC.
The Problem with Prescribing: Why Good Prescription Writing Matters
Prescribing sits at the intersection of pharmacology, clinical reasoning, communication, and law. A prescription is simultaneously a clinical document, a legal instrument, and a patient safety mechanism. When any element is wrong or absent, patient harm can follow directly.
The types of prescribing errors are well-documented and fall into four categories:
1. Inappropriate drug selection — prescribing a drug that is contraindicated, irrational for the condition, or second-best when a safer or cheaper alternative exists
2. Dosing errors — wrong dose, wrong frequency, wrong duration, or failure to adjust for renal/hepatic impairment, age, or weight
3. Communication errors — illegible handwriting, ambiguous units (writing 'U' for 'units' with insulin, which has been misread as '0'), absent or incorrect patient instructions
4. Omission errors — missing mandatory elements (prescriber registration number, patient details, drug strength) that make the prescription legally invalid or impossible to dispense correctly
A growing body of evidence from WHO, the British Medical Journal, and Indian pharmacoepidemiological studies shows that these errors are not random — they are systematic and predictable, and they can be substantially reduced through structured prescribing training. This is the rationale for the six-step WHO model that forms the backbone of this module.
The consequences of poor prescribing extend beyond individual patient harm: irrational antibiotic prescribing drives antimicrobial resistance; unnecessary costly drug choices burden patients and health systems; subtherapeutic dosing leads to treatment failure; supratherapeutic dosing causes toxicity.
P-Drug Methodology: The WHO Framework for Rational Drug Selection
The WHO Guide to Good Prescribing (1994, WHO/DAP/94.11) introduced the P-drug concept as the foundation of rational pharmacotherapy education. A P-drug (personal drug) is a drug that a prescriber has systematically selected as their first-line choice for a given clinical problem, based on explicit evaluation of four criteria: efficacy, safety, suitability, and cost. The act of building a personal P-drug list turns implicit habit into explicit, evidence-anchored decision-making.
The WHO framework defines six steps for every prescribing decision:
Step 1 — Define the patient's problem. Establish the diagnosis or clinical problem clearly. A vague problem produces a vague prescription. Is this uncomplicated lower UTI, or complicated UTI with fever and loin pain suggesting pyelonephritis?
Step 2 — Specify the therapeutic objective. What do you want to achieve? Symptom relief, cure, prevention, or palliation? The objective determines which outcome to optimise. For uncomplicated UTI: eradication of the causative organism with resolution of dysuria within 3–5 days.
Step 3 — Select your P-drug. Evaluate candidate drugs systematically against four criteria:
- Efficacy: Does it work for this problem in this patient? Is there RCT or guideline evidence?
- Safety: What are the serious adverse effects? Are there contraindications in this patient (e.g. quinolone avoidance in a patient with tendinopathy)?
- Suitability: Is the drug available locally? Can the patient take the oral formulation? Does it require refrigeration the patient cannot provide?
- Cost: Can the patient afford a full course? Is there an equivalent cheaper generic?
Step 4 — Write the prescription. Translate the P-drug choice into a legally complete, legible prescription (see next heading).
Step 5 — Inform the patient. Explain what the drug is, why it was chosen, how to take it, what to expect, what to avoid, and when to return if it is not working or if side effects occur.
Step 6 — Monitor the outcome. Plan a follow-up or clear instructions for when to seek review. Monitor for both efficacy (is the UTI resolving?) and safety (any rash suggesting allergy?).
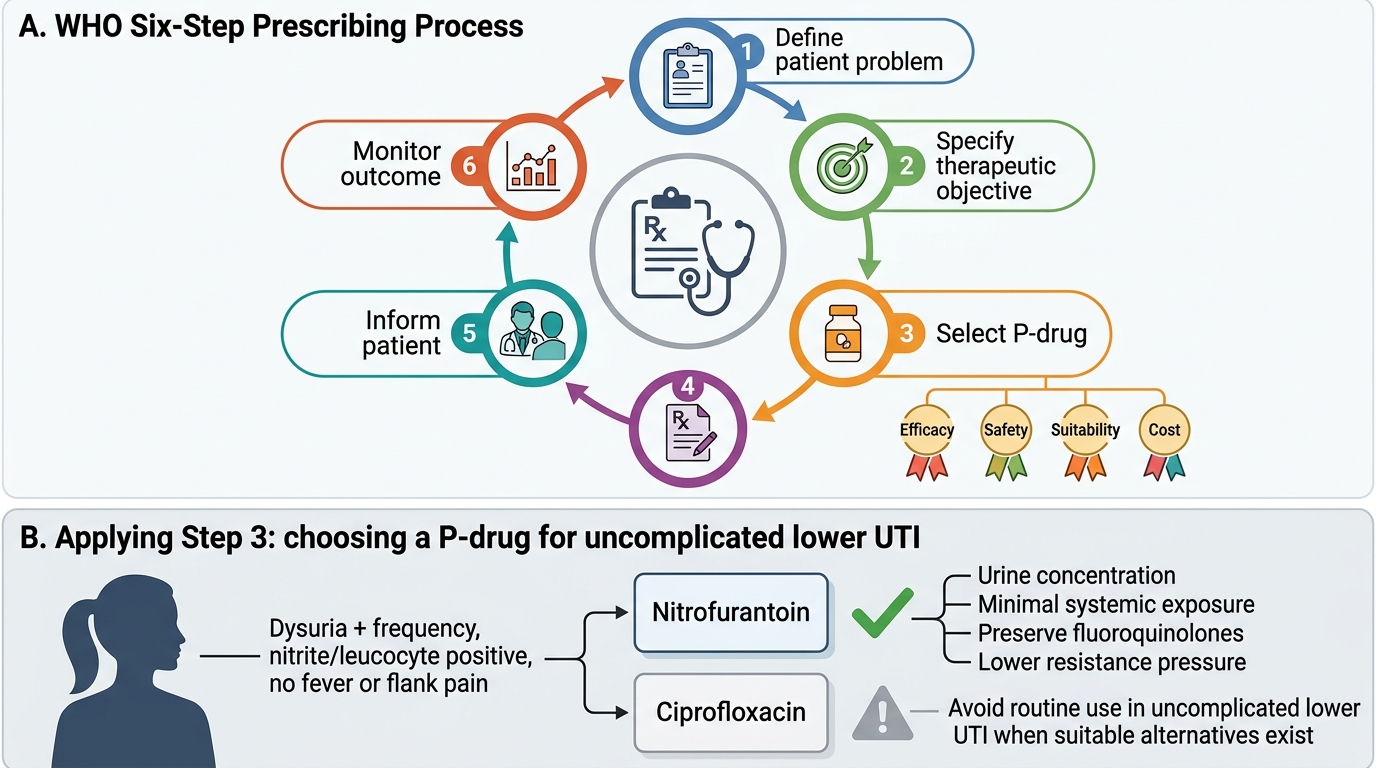
WHO Six-Step Prescribing Process and P-Drug Selection
Building a personal formulary — a curated list of P-drugs for the conditions you commonly treat — is the practical product of applying this methodology repeatedly. Senior physicians' prescribing expertise is partly their deeply internalised P-drug list, refined by years of experience and literature updates.
SELF-CHECK
A 24-year-old non-pregnant woman presents with dysuria, frequency, and suprapubic discomfort for 2 days, no fever, no flank pain. Urine dipstick is positive for nitrites and leucocytes. You are selecting a P-drug for uncomplicated lower UTI. Which criterion would MOST appropriately lead you to prefer nitrofurantoin over ciprofloxacin in this specific case?
A. A) Efficacy — nitrofurantoin has broader spectrum than ciprofloxacin for UTI
B. B) Safety and suitability — nitrofurantoin concentrates in urine with minimal systemic exposure, preserving fluoroquinolones for complicated infections and reducing resistance pressure
C. C) Cost — nitrofurantoin is universally cheaper than ciprofloxacin in all Indian settings
D. D) Efficacy — nitrofurantoin has been proven superior in randomised trials for E. coli UTI
Reveal Answer
Answer: B. B) Safety and suitability — nitrofurantoin concentrates in urine with minimal systemic exposure, preserving fluoroquinolones for complicated infections and reducing resistance pressure
B is correct. Nitrofurantoin achieves high urine concentrations with minimal systemic levels, is effective for uncomplicated lower UTI, and avoids exposing patients and community bacteria to fluoroquinolone pressure (fluoroquinolones are reserved for complicated infections). The safety/suitability criterion here incorporates antimicrobial stewardship — a key component of rational prescribing. Option A is wrong: ciprofloxacin has a broader spectrum. Option D is misleading: the preferred choice is based on antimicrobial stewardship principles, not superiority trials.
Writing a Correct, Rational, and Legible Prescription
A prescription is a legal document. In India, the Drugs and Cosmetics Act 1940 and its schedules define what constitutes a valid prescription for different drug categories, and a prescription that is missing mandatory elements may be refused by a pharmacist — or worse, dispensed incorrectly.
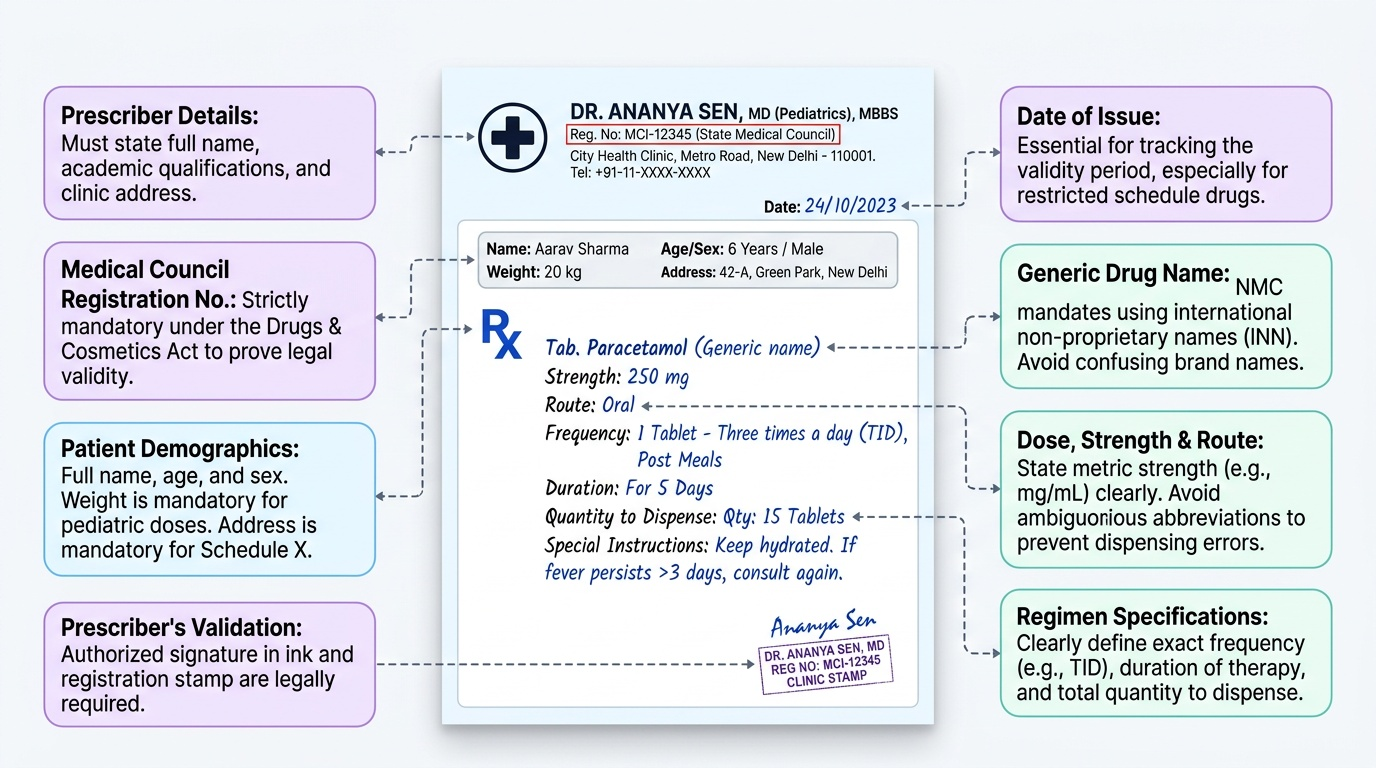
Every prescription in India must include the following elements:
Patient information:
- Full name of the patient
- Age (and weight for paediatric prescriptions)
- Sex
- Address (for controlled substances under Schedule X; recommended for all)
Prescriber information:
- Full name of the prescribing doctor
- Qualifications
- Medical registration number (mandatory for validity)
- Address of the clinic/hospital
- Date of prescription
Drug information (the Rx body):
- Drug name: generic (INN) name preferred — in India, NMC mandates that medical graduates write in generic names; if a brand is specified, the generic must also be stated
- Strength/dose (in unambiguous units — milligrams, not 'tabs' alone; never abbreviate 'units' as 'U' for insulin)
- Formulation: tablet, capsule, syrup, injection, inhaler, etc.
- Route of administration
- Frequency (e.g. twice daily, TID after meals)
- Duration of treatment
- Quantity to dispense (total number of tablets/mL)
- Special instructions: with food/fasting, avoid sunlight (for doxycycline), refrigeration required
Prescriber's signature and stamp (for Schedule H; signature in ink for Schedule X)
For Schedule X drugs (psychotropics, narcotics including opioid analgesics), the prescription must additionally state: the quantity in words, the purpose, and the patient's address — and must be retained as a duplicate by the pharmacist.
Provided image
Common avoidable errors include:
- Illegible handwriting (accounts for more than 20% of dispensing errors in Indian audits)
- Writing the dose without strength (e.g. 'Tab Amoxicillin 1 tab TID' — which strength?)
- Omitting duration (an antibiotic written without duration may be taken for days, weeks, or months)
- Using abbreviations not universally understood (QD/QID confusion; OD = once daily is less ambiguous)
- Missing the prescriber registration number, which pharmacists for Schedule H drugs must verify