Page 7 of 30
PH10.8 | PH10.8 | Essential Medicines and Formulary Choices — SDL Guide — SDL Guide
Learning Objectives
- Describe the concept of essential medicines and the criteria used for their selection by WHO and India's National List of Essential Medicines (NLEM)
- Explain the criteria for rational fixed-dose combinations and identify examples of rational and irrational FDCs
- Describe the criteria for OTC drug classification and explain steps to choose an essential medicine for a given clinical condition
INSTRUCTIONS
India has over 60,000 branded formulations available for prescribing, yet the WHO Model Essential Medicines List includes approximately 550 drugs that address the vast majority of healthcare needs. The essential medicines concept — selecting, procuring, and promoting the medicines that offer the greatest benefit at the lowest cost for the most people — is the foundation of rational national drug policy and equitable healthcare. This module explains how essential medicines are selected, what makes a fixed-dose combination rational or irrational, and how you can apply the essential medicines framework to make better formulary and prescribing choices.
References
- WHO Model List of Essential Medicines, 23rd edition (2023) (guideline)
- National List of Essential Medicines India 2022, Ministry of Health and Family Welfare (guideline)
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 4 (Essential medicines, FDCs) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the medical officer of a rural primary health centre. Your pharmacy has 80 drugs. A drug company representative visits and recommends adding an expensive fixed-dose combination antibiotic that 'covers more organisms' than the two separate antibiotics already on your shelf. The combination costs five times as much per course. The two individual drugs — both on the National Essential Medicines List — together cover the same organisms at separate doses. Do you add the combination to your formulary? What is your framework for this decision?
WHY THIS MATTERS
India's pharmaceutical market has one of the highest proportions of irrational fixed-dose combinations in the world — a 2019 Lancet analysis estimated that more than 30% of fixed-dose combination products available in India lacked rational justification. At the same time, access to even the most basic essential medicines remains uneven across India's geographic and economic spectrum. As a prescribing physician, you sit at both ends of this problem: you are simultaneously a consumer of the drug market and a steward of rational drug policy. The decisions you make daily — whether to prescribe an NLEM drug or a non-NLEM branded product, whether to use a fixed-dose combination or individual components, whether to guide a patient toward OTC self-medication — shape both individual patient outcomes and the broader healthcare system.
RECALL
Recall that in the P-drug selection framework (from the Rational Prescribing SDL), one of the four criteria is cost — and that the goal is always to achieve the therapeutic objective at the lowest cost that is safe and effective for the patient. The essential medicines concept operationalises this at the population level: instead of each prescriber independently deciding which drugs offer acceptable cost-effectiveness, a national expert body systematically evaluates the evidence and creates an approved list. Recall also from the Legal-Regulatory SDL that drug schedules (H, H1, X) determine prescription requirements — OTC drugs fall outside all schedule categories and are available without prescription.
The Essential Medicines Concept: Why Not Every Drug Can Be Essential
The essential medicines concept was introduced by the World Health Organization in 1977, when the WHO published its first Model List of Essential Medicines. The central insight was profound and practical: a relatively small number of carefully selected drugs — those that address the priority health needs of a population, have proven efficacy and safety, and are cost-effective — can meet the healthcare needs of the vast majority of patients in most clinical settings.
The WHO definition of essential medicines is: 'medicines that satisfy the priority health needs of the population. They are selected with due regard to public health relevance, evidence on efficacy and safety, and comparative cost-effectiveness.'
The essential medicines concept arose in response to a specific crisis: in the 1970s, many low- and middle-income countries were spending scarce healthcare budgets on hundreds or thousands of branded pharmaceutical products, many of which were duplicative, unproven, or significantly more expensive than generic alternatives for the same indication. By establishing a scientifically rigorous selection process, the EML framework allowed governments, health ministries, and hospital formulary committees to focus procurement, supply-chain management, price negotiation, and prescriber training on a manageable set of proven drugs.
In India, the National List of Essential Medicines (NLEM) is the domestically adapted equivalent. The NLEM 2022 lists approximately 384 medicines, revised from 376 in the previous 2015 list. Drugs on the NLEM are subject to price control under the Drug Price Control Order (DPCO) — making NLEM listings directly relevant to drug affordability for patients. Prescribers who default to NLEM medicines reduce the out-of-pocket burden on patients, which is the largest determinant of catastrophic health expenditure in India's mixed health financing system.
Selection Criteria for Essential Medicines: WHO and NLEM Framework
Essential medicines are not simply the cheapest drugs or the newest drugs — they are drugs that have passed a structured evidence review. Understanding the selection criteria makes you both a better prescriber (because you understand what 'essential' means) and a more critical evaluator of proposals to add or remove drugs from a formulary.
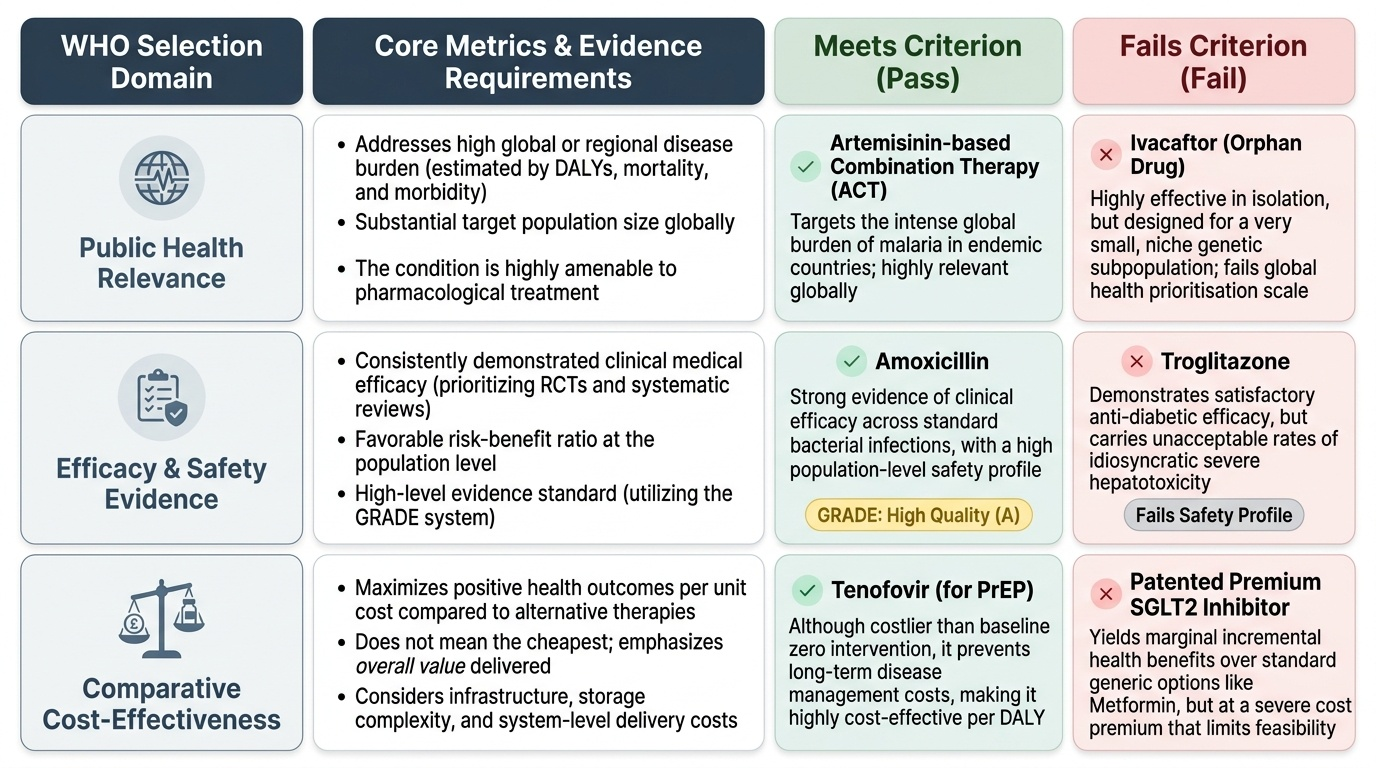
The WHO EML selection criteria operate across three domains:
1. Public health relevance. The disease or condition the drug addresses must be a priority health need — measured by burden of disease (DALY, mortality, morbidity), the population at risk, and whether the condition is amenable to pharmacological treatment. A drug for a rare disease in a high-income country may be essential in that context but not globally; a drug for malaria is essential globally.
2. Evidence on efficacy and safety. The drug must have demonstrated clinical efficacy (preferably from RCTs or systematic reviews) and an acceptable safety profile at the population level. Generic and originator products are evaluated equivalently — what matters is the active molecule's evidence base. A drug that is effective but has an unacceptable rate of serious adverse effects (e.g. hepatotoxicity, severe teratogenicity without adequate contraceptive management) may fail this criterion.
3. Comparative cost-effectiveness. The drug must offer acceptable value compared to alternatives for the same indication. This is not the cheapest drug wins — it is the drug that delivers the best health outcome per unit cost. A more expensive drug may be selected if it offers substantially better efficacy or safety than cheaper alternatives.
Additional pragmatic considerations include: regulatory status (must be approved by a national regulatory authority), quality assurance (must be available in acceptable quality), and supply reliability.
Provided image
India NLEM process: The NLEM is revised approximately every 5–7 years by an expert committee constituted by the Ministry of Health and Family Welfare. The 2022 revision added new vaccines, insulin analogues (including biosimilar insulin glargine), and newer fixed-dose TB regimens, while removing several drugs no longer considered first-line. The DPCO 2013 and its subsequent amendments provide the legal mechanism for price capping of NLEM medicines.
SELF-CHECK
A new antimalarial drug has excellent efficacy in RCTs but costs 50 times as much as the current first-line artemisinin-based combination therapy (ACT), with a similar safety and efficacy profile. Applying WHO EML selection criteria, what would be the MOST likely basis for NOT including it on the Model Essential Medicines List?
A. A) Insufficient public health relevance — malaria is not a priority disease
B. B) Inadequate safety evidence — RCTs are not sufficient for safety evaluation
C. C) Unfavourable comparative cost-effectiveness — similar outcomes at 50 times the cost of existing EML drug
D. D) Lack of regulatory approval — EML listing requires WHO pre-qualification only
Reveal Answer
Answer: C. C) Unfavourable comparative cost-effectiveness — similar outcomes at 50 times the cost of existing EML drug
C is correct. The comparative cost-effectiveness criterion would be the main basis for exclusion: if the new drug provides no additional efficacy or safety benefit over the existing ACT (which is already on the EML), then its 50-fold higher cost makes it unfavourable on cost-effectiveness grounds. Public health relevance is not an issue (malaria is a priority disease). RCTs are the preferred evidence type, not insufficient. Regulatory approval requires national authority approval, not WHO pre-qualification alone.
Fixed-Dose Combinations: Rational vs Irrational
A fixed-dose combination (FDC) is a pharmaceutical product containing two or more active substances combined in a fixed dose ratio in a single dosage form. FDCs are marketed for convenience, improved adherence, and sometimes for genuine pharmacological synergy — but they are also widely used for commercial reasons, and many available in India lack rational justification.
The criteria for a rational FDC are:
1. Both components are clinically indicated for the same patient at the same time
2. The combined use produces better therapeutic outcomes (greater efficacy, better safety, improved adherence) than the components given separately
3. The fixed-dose ratio is clinically appropriate for the vast majority of patients who need both drugs
4. The combination is not more expensive than the individual components without justification
Examples of rational FDCs:
- Levodopa + Carbidopa: carbidopa inhibits peripheral decarboxylation of levodopa, increasing central availability and reducing nausea — the combination is fundamentally superior to levodopa alone
- Artemether + Lumefantrine (Coartem): dual mechanism reduces the risk of resistance development in malaria; both components are needed together
- Isoniazid + Rifampicin + Pyrazinamide + Ethambutol (4FDC): all four required simultaneously in TB therapy; FDC improves adherence and prevents selective monotherapy
- Co-trimoxazole (Trimethoprim + Sulfamethoxazole): synergistic action against dihydrofolate pathway; the combination is more effective than either component alone
Examples of irrational FDCs (common in India):
- Analgesic + vitamins (paracetamol + Vitamin B complex): no evidence that adding vitamins improves pain outcomes; separate prescribing allows dose titration
- Two antibiotics in a fixed ratio for conditions where the ratio needed varies by pathogen and sensitivity
- Antidiabetic + vitamins at fixed dose: patient's vitamin requirements cannot be fixed at the same time and same ratio as their antidiabetic dose
- High-dose enzyme combinations (e.g. multiple digestive enzymes at arbitrary dose ratios) — often marketed without evidence
| FDC Type | Example | Rational? | Reason |
|---|---|---|---|
| Pharmacological synergy | Trimethoprim + Sulfamethoxazole | Yes | Sequential blockade of folate pathway; proven superior to monotherapy |
| Adherence improvement | 4-drug TB FDC | Yes | All 4 drugs needed together; FDC prevents selective non-adherence |
| Peripheral conversion inhibition | Levodopa + Carbidopa | Yes | Carbidopa prevents peripheral dopamine conversion, improving efficacy and tolerability |
| Analgesic + vitamin | Paracetamol + Vitamin B complex | No | No evidence for vitamin supplementation in pain management; prevents dose titration |