Page 1 of 26
PH6.1 | PH6.1 | Acid Peptic Disease Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Explain the pathophysiological basis of acid peptic disease, GERD, and Zollinger-Ellison syndrome
- Classify and compare the pharmacological agents used in acid peptic disease by mechanism, PK, and ADR profile
- Distinguish between the irreversible mechanism of PPIs and the reversible competitive block by H2RAs
- Construct a stepwise management plan for a patient with Hp-positive peptic ulcer, NSAID-induced ulcer, and erosive GERD
- Select the appropriate H. pylori eradication regimen (triple vs quadruple) and identify drug interactions relevant to PPIs
INSTRUCTIONS
Acid peptic disease encompasses peptic ulcer disease (PUD), gastro-oesophageal reflux disease (GERD), and stress-related mucosal injury — collectively among the most prevalent GI disorders seen in India. A thorough pharmacological understanding is essential not only for prescribing appropriately but also for avoiding common errors such as long-term PPI overuse, failure to test-and-treat H. pylori, or missing a drug interaction between clopidogrel and omeprazole. This module builds on gastric physiology you covered in Year 1 and equips you to construct evidence-based management plans.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 47 (Drugs for Acid Peptic Disorders) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch. 49 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old software engineer presents to your clinic with a 6-week history of epigastric pain that wakes him at night, temporarily relieved by food. He takes ibuprofen regularly for back pain and smokes half a pack of cigarettes daily. Upper GI endoscopy reveals a 1-cm duodenal ulcer and a positive rapid urease test for Helicobacter pylori. His previous doctor gave him a 2-week course of omeprazole alone, but the ulcer has not healed. He asks: 'Why is my ulcer not getting better, and what should I take now?' By the end of this module, you will be able to construct a complete, evidence-based answer — prescribing not just the right drug, but the right combination, duration, and strategy to ensure cure and prevent relapse.
WHY THIS MATTERS
Acid peptic disease affects an estimated 10–15% of the Indian population at some point in their lives, and peptic ulcer complications — haemorrhage and perforation — remain significant causes of emergency surgical admission. As a prescribing physician you will encounter these patients in internal medicine, surgery, and primary care every week. Beyond treating the acute episode, the key clinical skill is identifying and eradicating H. pylori (present in >70% of Indian PUD patients), stopping causative agents such as NSAIDs, and choosing the correct drug, dose, and duration. Pharmacological knowledge also helps you avoid iatrogenic harm: inappropriate long-term PPI use contributes to hypomagnesaemia, Clostridioides difficile colitis, and iron/B₁₂ malabsorption. Understanding the drug interaction between omeprazole (a CYP2C19 inhibitor) and clopidogrel (a prodrug requiring CYP2C19 for activation) can literally prevent a stent thrombosis in a cardiology patient.
RECALL
From your Year-1 physiology, recall that gastric acid secretion is controlled by three stimulants acting on the parietal cell: histamine (via H₂ receptors, the dominant pathway, cyclic AMP–mediated), acetylcholine (via M₃ muscarinic receptors), and gastrin (via CCK-B/gastrin receptors). All three pathways converge on the same final effector: the H⁺/K⁺-ATPase (the 'proton pump') on the luminal membrane of the parietal cell, which actively secretes H⁺ into the gastric lumen in exchange for K⁺. Mucus and bicarbonate from surface epithelial cells, stimulated by endogenous prostaglandins (especially PGE₂ and PGI₂), form the gastric mucosal defence. When you inhibit COX enzymes with NSAIDs, PGE₂ production falls, mucosal defence weakens, and acid becomes an aggressor rather than a digestive tool.
Pathophysiology of Acid Peptic Disease
Acid peptic disease results from an imbalance between aggressive luminal factors and the mucosal defence. Understanding this imbalance is essential because pharmacotherapy targets each element precisely.
The aggressive factors are gastric acid (HCl, with intraluminal pH as low as 1–2), pepsin (maximally active at pH <3, and inactivated above pH 6), bile reflux in some patients, and crucially, Helicobacter pylori — a Gram-negative, urease-positive, spiral-shaped bacterium that colonises the gastric antrum in >70% of Indian PUD patients. H. pylori damages the mucosa by producing ammonia (urease-generated), vacuolating cytotoxin A (VacA), and cytotoxin-associated gene A (CagA) protein, and by eliciting a chronic inflammatory response. It also suppresses somatostatin (D-cell) function, increasing gastrin-driven acid output.
The defensive factors are the mucus–bicarbonate barrier secreted by surface mucous cells, prostaglandin E₂ and I₂ (produced by COX-1 in gastric mucosa, stimulating mucus and bicarbonate secretion and mucosal blood flow), the tight junctions of surface epithelial cells, and the rapid cell-turnover repair capacity of the gastric epithelium.
GERD (gastro-oesophageal reflux disease) arises primarily from a dysfunctional lower oesophageal sphincter (transient relaxations or globally reduced tone) allowing acid to reflux into the lower oesophagus, which lacks the mucus–bicarbonate defence of the stomach. The pathological consequence ranges from non-erosive reflux disease (NERD) through erosive oesophagitis to Barrett's oesophagus. Zollinger-Ellison syndrome (ZES) is caused by a gastrin-secreting neuroendocrine tumour (gastrinoma), leading to massively elevated gastric acid output and multiple refractory peptic ulcers.
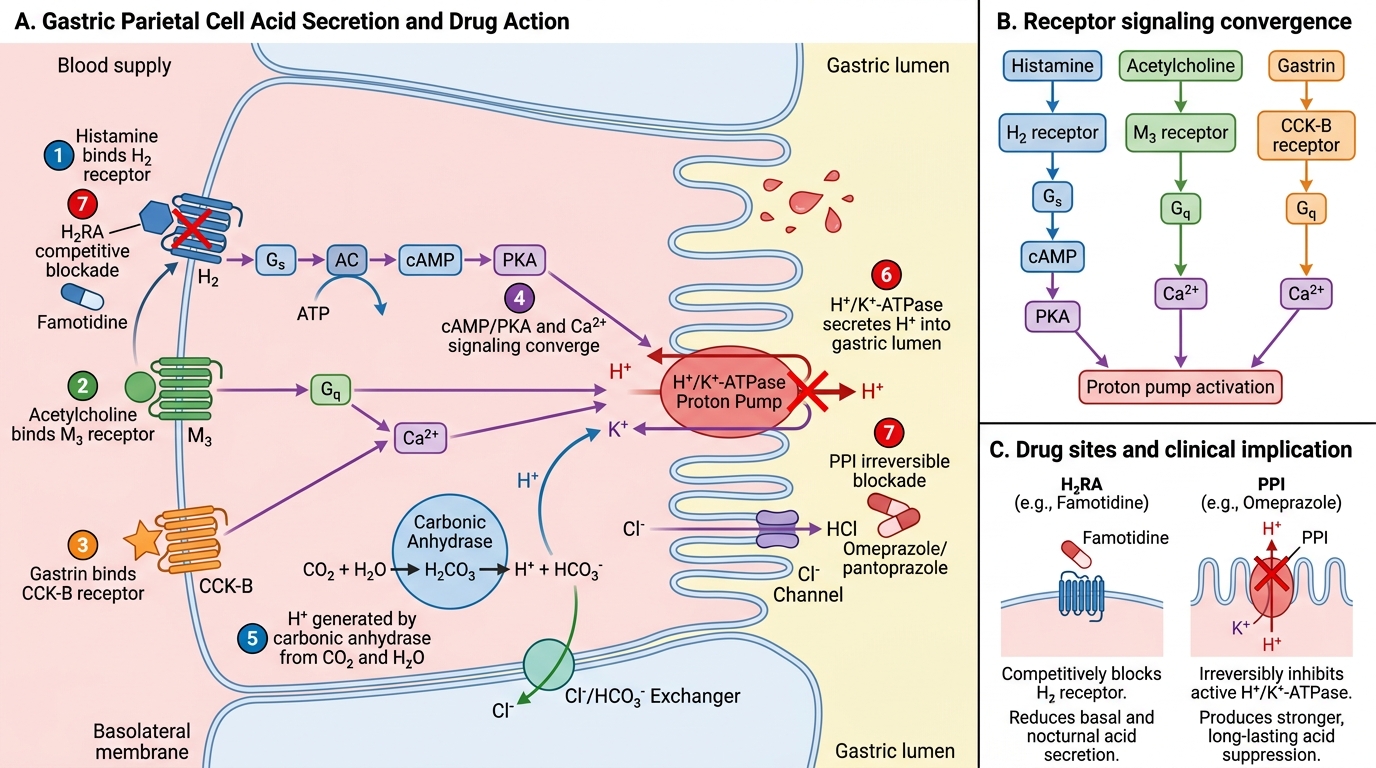
Parietal Cell Acid Secretion and Drug Blockade
Therapeutic Goals and the Rationale for Drug Choice
The therapeutic goals in acid peptic disease are shaped by the underlying condition and its severity. A clear hierarchy of goals prevents the common error of treating only the symptom while leaving the root cause unaddressed.
For peptic ulcer disease, the primary goals are: (1) relieve symptoms (pain, nausea); (2) heal the mucosal lesion — endoscopically confirmed healing in 4–8 weeks; (3) eradicate H. pylori if positive — this is the single most important step for preventing relapse; (4) remove causative agents (NSAIDs, smoking, alcohol); (5) prevent complications (haemorrhage, perforation, obstruction). For GERD, the goals are: symptom control (heartburn, regurgitation), healing of erosive oesophagitis (in erosive disease), and maintenance of remission to prevent Barrett's change and adenocarcinoma. For ZES, the goal is to achieve an intragastric pH >4 continuously — which requires high-dose PPI therapy, often twice daily at double doses.
The rationale for choosing acid suppression over other approaches lies in the physiology: acid is the common denominator in symptom generation and mucosal injury. Raising intragastric pH above 4 (for ulcer healing) or above 6 (for optimal haemostasis in bleeding ulcer) creates the chemical environment for mucosal repair. The choice between a PPI and an H2RA depends on depth of suppression needed: PPIs achieve >90% suppression of 24-hour acid output, far exceeding H2RAs (~70% maximal suppression), and are superior for erosive disease and H. pylori eradication background.
SELF-CHECK
A patient with a newly diagnosed H. pylori-positive duodenal ulcer is prescribed omeprazole alone for 4 weeks. The ulcer fails to heal at follow-up. What is the MOST important missing element of therapy?
A. Switching to a higher-dose PPI twice daily
B. Adding sucralfate for mucosal protection
C. Adding antibiotics to eradicate H. pylori
D. Adding an H2RA for nighttime acid suppression
Reveal Answer
Answer: C. Adding antibiotics to eradicate H. pylori
H. pylori eradication is the cornerstone of PUD treatment when the organism is present. Without antibiotic-based eradication, the bacterium sustains the mucosal inflammation and inhibits healing, and the ulcer recurrence rate approaches 80% within 1 year. PPI alone can suppress acid and relieve symptoms but does not eliminate the organism. Triple therapy (PPI + amoxicillin + clarithromycin × 14 days) is the standard first-line approach in India. Higher-dose PPI, sucralfate, or H2RA addition are not substitutes for eradication when H. pylori is positive.
Classification of Drugs in Acid Peptic Disease
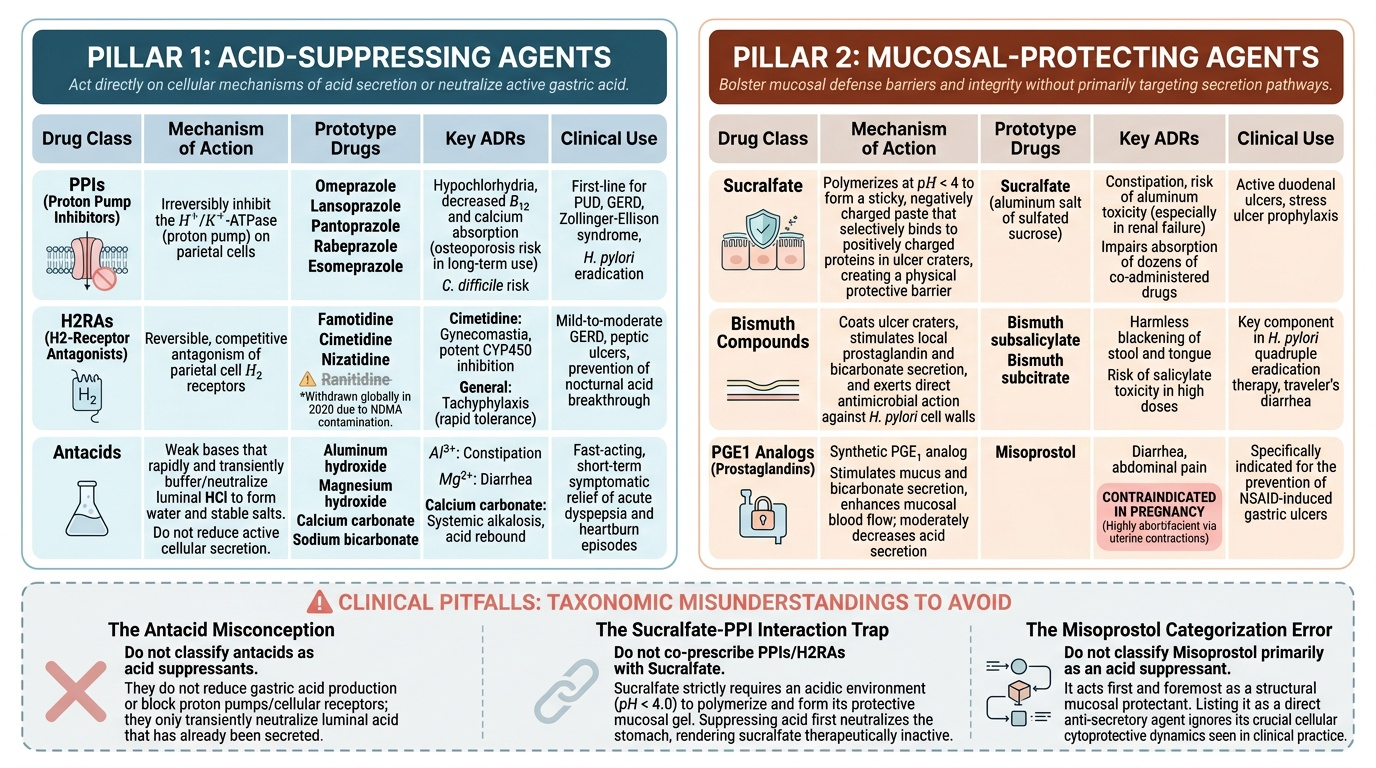
The drugs used in acid peptic disease fall into two major pharmacological pillars: those that reduce acid secretion (acid-suppressing agents) and those that protect or restore the mucosa (mucosal-protecting agents). Understanding this two-pillar taxonomy prevents the common error of treating every peptic condition with the same drug without considering the pathophysiological target. Most clinical prescribing errors in this disease area stem from not knowing which pillar a drug belongs to: for example, antacids are sometimes mistakenly described as 'acid suppressants,' sucralfate is sometimes combined with PPIs despite needing acid pH for activation, and misoprostol is sometimes listed under 'acid-suppressing' agents when it is actually a mucosal protectant with only a modest antisecretory component. A clear taxonomy prevents these category errors before they reach the patient.
Pillar 1 — Acid-Suppressing Agents act directly on the mechanisms of acid secretion:
- Proton pump inhibitors (PPIs): omeprazole, lansoprazole, pantoprazole, rabeprazole, esomeprazole — the most potent acid suppressants available; irreversibly inhibit H⁺/K⁺-ATPase.
- H₂-receptor antagonists (H2RAs): famotidine, cimetidine, nizatidine (ranitidine withdrawn globally in 2020 due to NDMA contamination) — reversible competitive blockers at parietal cell H₂ receptors.
- Antacids: aluminium hydroxide, magnesium hydroxide, calcium carbonate, sodium bicarbonate — neutralise luminal acid rapidly but transiently; do not reduce acid secretion.
- Anticholinergics (M1 blockers): pirenzepine — reduce acid secretion via M1 block but largely replaced by PPIs due to adverse effects.
Pillar 2 — Mucosal-Protecting Agents act on the defence side:
- Sucralfate — forms a viscous, adherent barrier over the ulcer base.
- Bismuth compounds — bismuth subcitrate/subsalicylate; local bactericidal action against H. pylori; combine with antibiotics in quadruple therapy.
- Prostaglandin analogues: misoprostol (synthetic PGE₁ analogue) — enhances mucus/bicarbonate secretion and reduces acid output; primarily used for NSAID-induced ulcer prevention.
Provided image