Page 3 of 26
PH6.1 | PH6.1 | Acid Peptic Disease Pharmacotherapy — SDL Guide — SDL Guide (Part 3)
H. pylori Eradication and Management Plans
Constructing a management plan for acid peptic disease requires integrating the pharmacological knowledge above with clinical decision-making guided by the specific condition, H. pylori status, NSAID use, and comorbidities. The single most consequential clinical decision in PUD management is whether to test for and eradicate H. pylori — this transforms a recurring, relapsing disease into one that is cured in the majority of patients with a single course of antibiotic-based therapy. Without eradication, even optimal acid suppression leaves the bacterium in place to re-inflame the mucosa, and ulcer recurrence within a year approaches 80%. A systematic approach — diagnose the condition, identify causative factors, suppress acid, eradicate the organism, remove the offending agent, and confirm cure — is the framework that separates rational pharmacotherapy from symptom chasing.
H. pylori eradication — the cornerstone of PUD management:
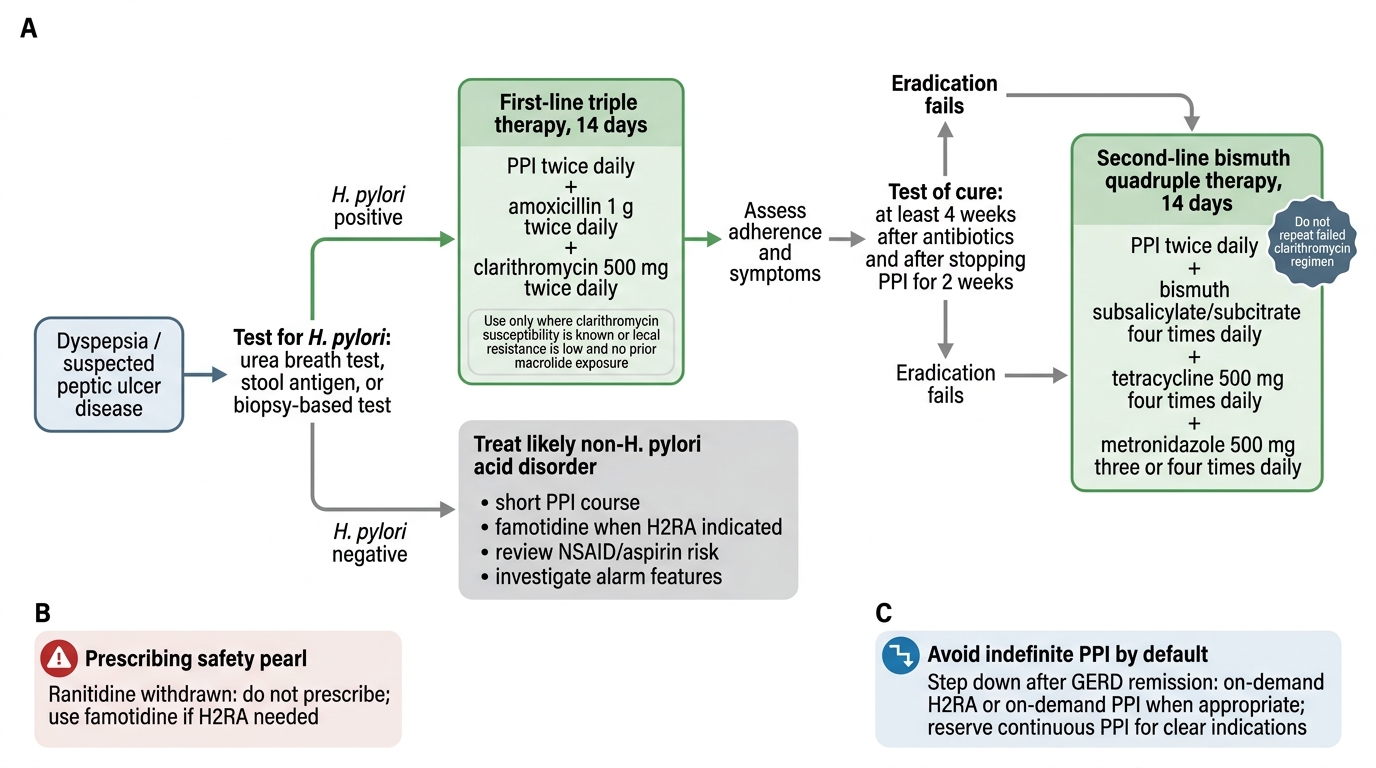
All patients with documented peptic ulcer disease should be tested for H. pylori (urea breath test, faecal antigen test, or rapid urease test on biopsy). If positive, eradication is mandatory. Without eradication, ulcer relapse within 1 year exceeds 80%; with successful eradication, it falls to <5%.
- First-line: Standard triple therapy — PPI (standard dose, e.g. omeprazole 20 mg) + amoxicillin 1 g + clarithromycin 500 mg, all twice daily × 14 days (14 days preferred over 7 days for higher eradication rates). Eradication rate ~80% in clarithromycin-susceptible regions.
- Second-line (clarithromycin-resistant regions, or after first-line failure): Bismuth-based quadruple therapy — PPI + bismuth subcitrate + tetracycline 500 mg + metronidazole 400 mg, all twice or thrice daily × 10–14 days. Also used as first-line in regions with >15% clarithromycin resistance (which includes parts of India).
- Alternative second-line: PPI + amoxicillin + levofloxacin (× 14 days) — used after clarithromycin failure; increasing levofloxacin resistance is a concern.
- Confirm eradication with a urea breath test or faecal antigen test ≥4 weeks after stopping antibiotics AND PPIs (PPIs suppress H. pylori density and can cause false-negative results if not stopped).
Condition-specific management plans:
| Condition | First-line | Duration | Additional notes |
|---|---|---|---|
| Hp⁺ duodenal ulcer | Triple therapy (PPI + amox + clarithr) | 14 days | Continue PPI 4 weeks after antibiotics for uncomplicated ulcer; 8 weeks if large ulcer |
| Hp⁺ gastric ulcer | Triple therapy | 14 days | Continue PPI 8 weeks; repeat endoscopy to confirm healing + rule out malignancy |
| Hp⁻ PUD (NSAID-induced) | Stop NSAID + PPI | 4–8 weeks | If NSAID cannot be stopped, use PPI co-therapy; consider COX-2 selective NSAID + PPI |
| Erosive GERD | PPI once daily before breakfast | 4–8 weeks | Maintenance PPI if recurrence; step-down to on-demand after remission |
| NERD (non-erosive GERD) | PPI on-demand or H2RA | — | Step-up if insufficient |
| Zollinger-Ellison syndrome | PPI high dose (40–120 mg/day) | Long-term | Twice-daily PPI; titrate to gastric pH >4; investigate for MEN1 |
| Stress ulcer (ICU) | IV famotidine or IV PPI | During critical illness | Step-down on recovery |
Key drug interaction to remember: Avoid prescribing omeprazole or esomeprazole with clopidogrel — both are potent CYP2C19 inhibitors, reducing conversion of clopidogrel (prodrug) to its active thiol form, potentially compromising antiplatelet protection. Prefer pantoprazole or rabeprazole in clopidogrel-treated patients (less CYP2C19 inhibition).
H. pylori Eradication Management Flowchart
CLINICAL PEARL
Two common prescribing errors that cause real harm:
- Ranitidine in 2026 is not acceptable. Ranitidine was withdrawn from the global market in 2020 due to unacceptable levels of NDMA (a probable carcinogen) that increase over time in storage. When an H2RA is clinically indicated, use famotidine. If you encounter a patient still on ranitidine, switch them.
- PPIs are not the first choice for indefinite long-term use in every acid-related complaint. Step-down therapy after GERD remission (from PPI to on-demand H2RA or proton pump inhibitor on-demand) reduces cumulative exposure and long-term ADR risk (hypomagnesaemia, vitamin B₁₂ depletion, C. difficile risk). Reserve continuous PPI for erosive GERD, high-risk NSAID co-therapy, ZES, and post-eradication maintenance of complicated ulcers — not for every patient with heartburn who feels better on omeprazole.
Self-Assessment — Acid Peptic Disease Pharmacotherapy
Self-assessment is not merely an examination exercise — it is the mechanism through which you consolidate pharmacological knowledge into reliable clinical judgment. The scenarios below are constructed around real prescribing decision points that a Year-2 student should be able to navigate: choosing between a PPI and an H2RA, selecting the correct H. pylori eradication regimen, identifying a drug interaction that could harm a cardiac patient, and determining the best gastroprotective strategy for a patient who cannot stop an NSAID. Work through each question by applying the taxonomy and mechanisms covered in this module, rather than guessing from drug name recognition alone. Read the explanation fully even if you answer correctly — the reasoning behind the answer is what matters for OSCE and clinical practice.
Use the micro-quiz below to test the key decision points: selection of eradication regimen, mechanism of action distinctions, drug interactions, and choosing the correct agent for the clinical context.
SELF-CHECK
A 62-year-old patient with rheumatoid arthritis requires long-term diclofenac. She has no active GI symptoms but has a history of peptic ulcer. What is the MOST appropriate gastroprotective strategy?
A. Switch to a COX-2 inhibitor (celecoxib) alone
B. Co-prescribe omeprazole 20 mg daily with diclofenac
C. Prescribe misoprostol 200 µg four times daily with diclofenac
D. Co-prescribe famotidine 40 mg twice daily
Reveal Answer
Answer: B. Co-prescribe omeprazole 20 mg daily with diclofenac
In a high-risk patient (history of PUD) requiring long-term NSAID therapy, co-prescription of a PPI is the standard gastroprotective strategy. Omeprazole 20 mg once daily effectively prevents NSAID-induced gastric and duodenal ulcers. While COX-2 inhibitor switching reduces GI risk compared to non-selective NSAIDs, a COX-2 inhibitor alone without PPI is not adequate in a patient with prior ulcer history — guidelines recommend PPI + COX-2 inhibitor in the highest-risk patients. Misoprostol is effective but poorly tolerated (diarrhoea, cramps) and requires four-times-daily dosing. Famotidine at standard doses is inferior to PPIs for NSAID ulcer prevention.