Page 5 of 26
PH6.2 | PH6.2 | Prokinetics and Antiemetics — SDL Guide — SDL Guide
Learning Objectives
- Describe the vomiting reflex arc, identifying the receptor types at the CTZ, NTS, vestibular nucleus, and vagal afferents that drug classes target
- Classify prokinetic and antiemetic drugs by their primary receptor mechanism
- Distinguish metoclopramide from domperidone in terms of CNS penetration, EPS risk, and cardiac effects
- Select the appropriate antiemetic for a given clinical context: CINV, PONV, motion sickness, pregnancy nausea, and opioid-induced nausea
- Identify cisapride as a withdrawn prokinetic and explain why its use is contraindicated
INSTRUCTIONS
Nausea and vomiting are among the most distressing symptoms in clinical medicine — experienced by chemotherapy patients, post-operative patients, pregnant women, and travellers alike. The pharmacological management of these symptoms is nuanced because different aetiologies involve different receptor pathways, and the wrong drug chosen without understanding mechanism will be ineffective or harmful. This module builds on the neurophysiology of the vomiting reflex and equips you to match drug to mechanism and context with confidence.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 48 (Prokinetics and Antiemetics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch. 50 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman with breast cancer is starting her first cycle of doxorubicin-cyclophosphamide (AC) chemotherapy — a moderately-to-highly emetogenic regimen. She has heard from other patients that the nausea is unbearable and asks if there is 'anything to prevent it.' Meanwhile, in the next bay, a 70-year-old man with Parkinson's disease who was started on metoclopramide for nausea two weeks ago is now presenting with worsening tremor and a new involuntary facial grimacing. And in the emergency department, a 22-year-old woman with motion sickness on a long train journey is asking for 'anything to stop the vomiting' — she was given ondansetron at a pharmacy and reports it did nothing. Three different patients, three different types of nausea, three different pharmacological answers. By the end of this module, you will know why ondansetron fails in motion sickness, why metoclopramide worsened the Parkinson's patient's symptoms, and which combination to prescribe for CINV prevention.
WHY THIS MATTERS
Nausea and vomiting affect virtually every patient population you will treat — from chemotherapy-induced nausea (the most distressing symptom reported by cancer patients, often worse than the disease itself) to post-operative nausea and vomiting (PONV, affecting 30% of surgical patients), pregnancy nausea (affecting 80% of pregnant women in the first trimester), motion sickness, vestibular disease, and opioid-induced emesis. Antiemetic prescribing is high-stakes: choosing the wrong drug (ondansetron for motion sickness, metoclopramide in Parkinson's disease, domperidone in arrhythmia-prone patients) causes either treatment failure or direct harm. Understanding the receptor pharmacology is what separates rational prescribing from empirical guessing — and that distinction matters most when a patient is already suffering.
RECALL
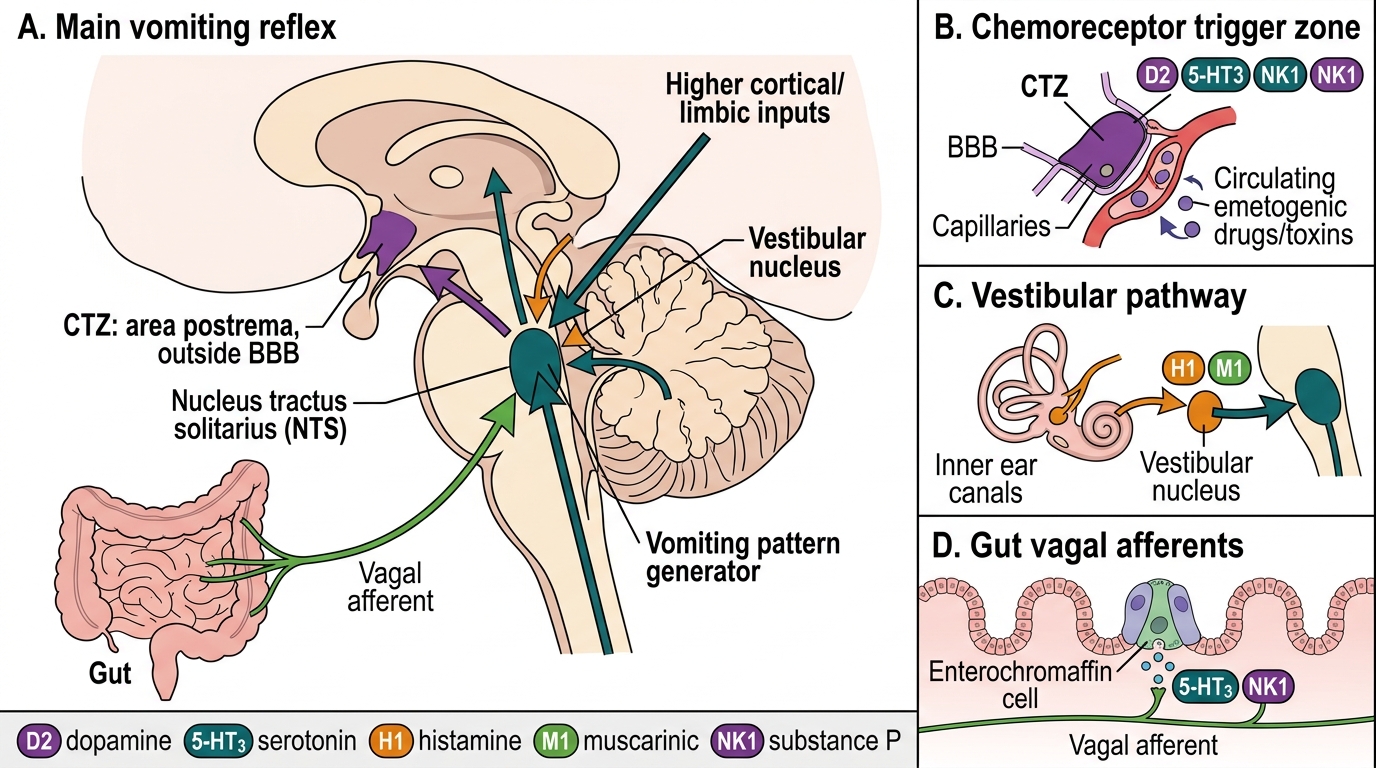
From your Year-1 physiology, recall the vomiting centre (now understood as a loose network in the medullary reticular formation, centred on the nucleus tractus solitarius/NTS) and the chemoreceptor trigger zone (CTZ), which lies in the area postrema on the floor of the fourth ventricle — a circumventricular organ outside the blood-brain barrier. The CTZ is therefore directly exposed to blood-borne emetic agents (drugs, toxins, uraemic metabolites) and expresses high densities of D₂ (dopamine), 5-HT₃ (serotonin), and NK₁ (neurokinin-1/substance P) receptors. Vestibular input (motion sickness, Ménière's disease) reaches the NTS primarily via H₁ (histamine) and M₁ (muscarinic) receptors. Vagal afferents from the gut — stimulated by mucosal irritation, distension, and serotonin released from enterochromaffin cells during chemotherapy or radiation — express 5-HT₃ receptors and project to the NTS. This receptor map is the direct blueprint for antiemetic drug classification.
Pathophysiology of Nausea, Vomiting, and Gastroparesis
Nausea and vomiting represent a coordinated protective reflex mediated by a distributed brainstem network, not a single anatomical vomiting centre. This distinction has profound pharmacological implications: different clinical causes of nausea engage different receptor populations at different nodes of the network, so an antiemetic that works brilliantly for one aetiology will be completely ineffective for another. The most common clinical error in antiemetic prescribing is selecting an agent without knowing which pathway is driving the symptom. Mapping the reflex arc onto its receptor pharmacology is therefore the direct foundation of every prescribing decision in this module.
Nausea and vomiting represent a coordinated protective reflex mediated by a distributed brainstem network, not a single 'vomiting centre.' Recognising the distinct afferent pathways and receptor populations at each node is the foundation of rational antiemetic prescribing — because blocking the wrong receptor at the wrong node achieves nothing.
The vomiting reflex arc has four principal afferent inputs that converge on the nucleus tractus solitarius (NTS), which integrates signals and co-ordinates the efferent motor output (diaphragmatic, abdominal wall, and pharyngeal contractions producing vomiting):
- Chemoreceptor trigger zone (CTZ) / area postrema: Located outside the blood-brain barrier on the floor of the fourth ventricle, the CTZ is exposed to circulating emetic agents — drugs (opioids, cytotoxic agents, digoxin), uraemic toxins, and metabolic disturbances. It expresses high densities of D₂, 5-HT₃, and NK₁ receptors. Dopaminergic drugs and uraemia trigger emesis predominantly through this route.
- Vagal and splanchnic afferents from the gut: The intestinal mucosa contains enterochromaffin cells that release serotonin (5-HT) during mechanical distension, mucosal irritation, or after cytotoxic chemotherapy/radiation. This 5-HT activates 5-HT₃ receptors on vagal afferents, which signal the NTS. This is the dominant pathway for chemotherapy-induced nausea and vomiting (CINV) — particularly the acute phase.
- Vestibular system: Motion and positional changes stimulate vestibular hair cells, which project to the NTS via H₁ and M₁ receptor-expressing afferents. This is why antihistamines (promethazine) and anticholinergics (scopolamine) are effective for motion sickness but ondansetron (5-HT₃) is not — the vestibular pathway does not prominently involve 5-HT₃.
- Higher cortical centres: Anticipatory nausea (conditioned response to chemotherapy environment), anxiety, and unpleasant stimuli (smell, sight) modulate the NTS via cortical input.
Gastroparesis — delayed gastric emptying without mechanical obstruction — results from impaired co-ordination of the interstitial cells of Cajal and enteric neurones. Dopamine (D₂) activation in the myenteric plexus reduces antral contractions and pyloric tone; prokinetics that block D₂ receptors (metoclopramide, domperidone) or activate 5-HT₄ receptors (metoclopramide, prucalopride) restore coordinated peristalsis.
Vomiting Reflex Arc and Antiemetic Receptor Targets
Therapeutic Goals in Nausea, Vomiting, and GI Dysmotility
The therapeutic goals in managing nausea, vomiting, and GI dysmotility vary substantially by clinical context, and the failure to match the goal to the context is the most common reason antiemetics fail. A drug that works brilliantly for CINV may be completely ineffective for motion sickness — not because it is a poor drug, but because the aetiology engages a different receptor pathway entirely.
For CINV (chemotherapy-induced nausea and vomiting), the goal is prophylaxis across three phases: the acute phase (0–24 hours post-chemotherapy, predominantly 5-HT₃-mediated), the delayed phase (24–120 hours, predominantly NK₁/substance P-mediated, worse than the acute phase for many patients), and the anticipatory phase (conditioned reflex, requires behavioural intervention ± benzodiazepine). For PONV (post-operative nausea and vomiting), the goal is prevention before emergence from anaesthesia using a multimodal approach (5-HT₃ antagonist + dexamethasone ± droperidol or transdermal scopolamine). For motion sickness, the goal is prophylaxis and early symptom relief using agents that block the vestibular pathway (H₁ antihistamines, scopolamine) — NOT 5-HT₃ antagonists. For pregnancy nausea (hyperemesis gravidarum), the goal is symptom control with the safest available agent for gestational age, avoiding teratogenic drugs. For gastroparesis, the goal is restoration of gastric emptying with the shortest effective course of a prokinetic, minimising EPS risk.
Classification of Prokinetics and Antiemetics
Prokinetics and antiemetics can be classified in two complementary ways: by their functional role (prokinetic vs antiemetic) and by their primary receptor mechanism (which determines clinical application and adverse effect profile). These two classification systems overlap in an important and instructive way, because several drugs serve both roles simultaneously. Most importantly, metoclopramide acts as a prokinetic through its 5-HT4 agonism on the myenteric plexus while simultaneously acting as a central antiemetic through its D2 antagonism at the CTZ. Mapping every drug to both its mechanism and its target receptor node is the key intellectual step that converts rote memorisation into clinical reasoning and prevents prescribing errors such as giving metoclopramide to a Parkinson's patient or ondansetron for motion sickness.
Prokinetics and antiemetics can be classified in two complementary ways: by their functional role (prokinetic vs antiemetic) and by their primary receptor mechanism (which determines clinical application and adverse effect profile). The functional and mechanistic classifications overlap, because several drugs serve both roles — most importantly metoclopramide, which is both a prokinetic (D₂ + 5-HT₄ action on myenteric plexus → improved gastric emptying) and an antiemetic (D₂ antagonism at the CTZ → suppresses vomiting). Mapping every drug to both its mechanism and its target receptor node is the key intellectual step that prevents prescribing errors.
Prokinetic agents (enhance coordinated GI motility):
- Metoclopramide — D₂ antagonist + 5-HT₄ agonist; prokinetic + antiemetic; crosses BBB
- Domperidone — peripheral D₂ antagonist; prokinetic; minimal CNS penetration
- Prucalopride — selective 5-HT₄ agonist; colon-selective; used for chronic constipation (not nausea)
- Itopride — D₂ antagonist + cholinesterase inhibitor; upper GI prokinetic
- Cisapride — 5-HT₄ agonist; WITHDRAWN globally in 2000 (fatal torsades de pointes from hERG channel block → QT prolongation → VF); do not prescribe under any circumstances
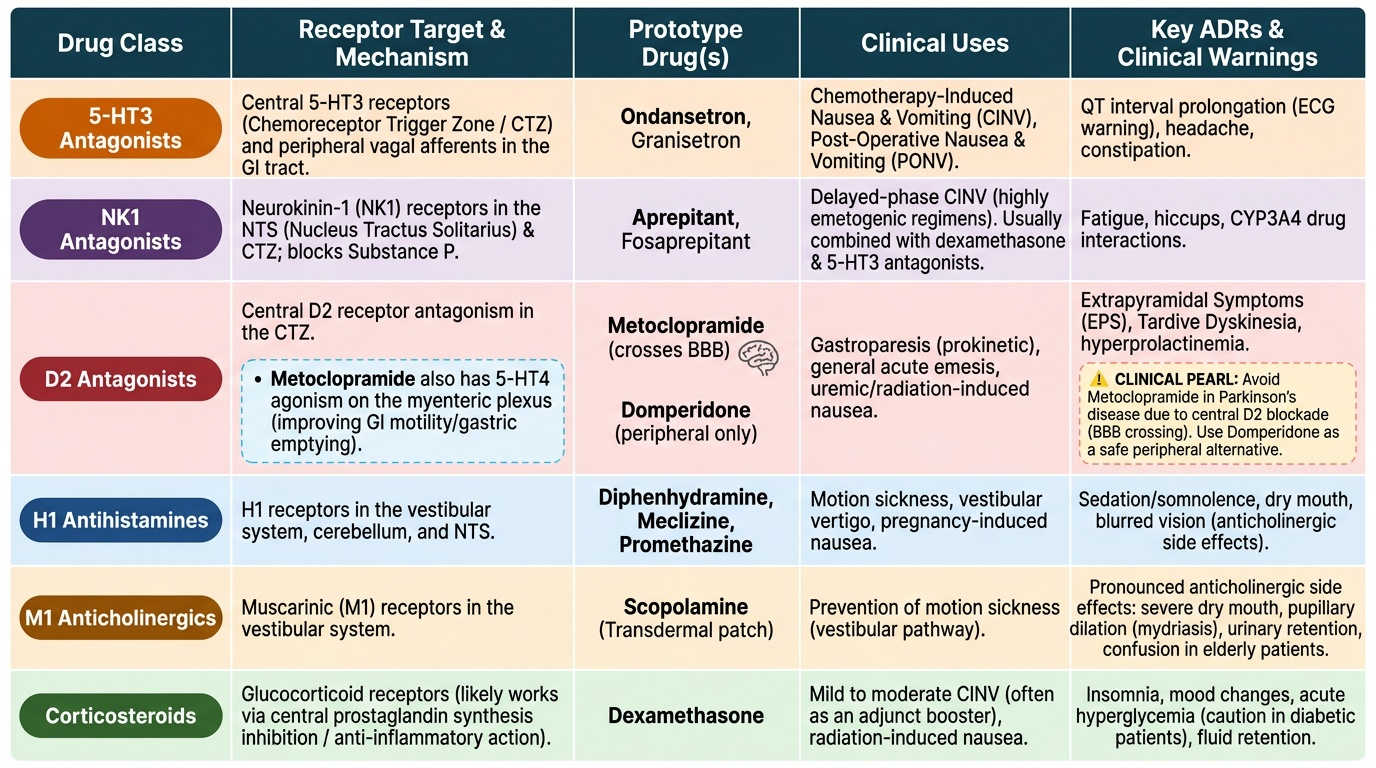
Antiemetics by mechanism (receptor-matched to aetiology):
- 5-HT₃ antagonists — ondansetron, granisetron, palonosetron; block vagal 5-HT₃ + CTZ; CINV/PONV
- NK₁ antagonists — aprepitant, fosaprepitant; block substance P at NK₁; delayed CINV
- D₂ antagonists — metoclopramide, prochlorperazine, haloperidol, domperidone; broad antiemetic
- H₁ antihistamines — promethazine, cyclizine, dimenhydrinate; motion sickness, pregnancy nausea
- M₁ anticholinergics — hyoscine/scopolamine; motion sickness (transdermal)
- Corticosteroids — dexamethasone; adjunct in CINV/PONV (mechanism not fully established)
- Cannabinoids — nabilone; refractory CINV (appetite stimulation + antiemetic)
Provided image
SELF-CHECK
A patient with motion sickness is given ondansetron by a pharmacist. She reports that it had no effect on her vomiting during the car journey. What is the MOST pharmacologically accurate explanation?
A. Ondansetron was the correct drug but the dose was insufficient
B. Motion sickness uses the vestibular H1/M1 pathway, not the 5-HT3 pathway that ondansetron blocks
C. Ondansetron was absorbed too slowly because she took it on an empty stomach
D. Motion sickness is best treated with D2 antagonists, not 5-HT3 antagonists
Reveal Answer
Answer: B. Motion sickness uses the vestibular H1/M1 pathway, not the 5-HT3 pathway that ondansetron blocks
Motion sickness engages the vestibular afferent pathway to the NTS, which operates predominantly via H1 (histamine) and M1 (muscarinic) receptors — not the 5-HT3 receptors that ondansetron blocks. Ondansetron is effective for CINV and PONV because those aetiologies involve 5-HT3-mediated vagal afferents from the gut and the CTZ. Blocking 5-HT3 has no effect on the vestibular afferent signals triggering motion sickness. The correct agents are H1 antihistamines (promethazine, cyclizine, dimenhydrinate) or the M1 antagonist hyoscine/scopolamine (transdermal patch). D2 antagonists (metoclopramide) have some antiemetic effect but are not specific for motion sickness and carry EPS risk.