Page 9 of 26
PH6.3 | PH6.3 | Diarrhoea Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Classify diarrhoea by pathophysiological mechanism and identify how each mechanism determines the pharmacological approach
- Explain the rationale for ORS as the cornerstone of diarrhoea management, including the sodium-glucose cotransport mechanism
- Distinguish the mechanism, appropriate use, and contraindications of loperamide from those of antibiotics in acute diarrhoea
- Devise a pharmacotherapeutic plan for acute diarrhoea in an adult and in a child under 5 years
- Select the appropriate antibiotic for specific diarrhoeal pathogens including C. difficile
INSTRUCTIONS
Diarrhoea kills approximately 500,000 children under five globally each year, and India carries one of the highest burdens. Yet the most life-saving intervention is not an antibiotic or a sophisticated drug — it is ORS, correctly prepared and given. This module teaches the pharmacology of antidiarrhoeal agents against the backdrop of this epidemiological reality, with particular attention to the critical distinction between secretory and invasive diarrhoea — a distinction that determines whether anti-motility agents such as loperamide are appropriate or potentially fatal.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 49 (Antidiarrhoeal Drugs) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch. 50 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A village health worker in rural Tamil Nadu presents two children to the PHC. The first is a 2-year-old with 10 loose stools since yesterday, sunken eyes, reduced skin turgor, and no blood in the stool — a classic case of acute watery diarrhoea, likely rotavirus. The second is an 8-year-old with 6 stools in 24 hours, each containing blood and mucus, with a temperature of 38.8°C — acute dysentery, likely Shigella. The health worker asks for 'a tablet to stop the diarrhoea' for both. By the end of this module you will know why: (a) loperamide is dangerous in the second child and potentially harmful in the first (under 2 years); (b) ORS is mandatory for both; (c) only the second child needs antibiotics; and (d) zinc supplementation should be given to both. The ability to make these distinctions — not to prescribe indiscriminately — is what saves lives in this setting.
WHY THIS MATTERS
Diarrhoeal disease is the second leading cause of death in children under five globally and a major cause of preventable morbidity in adults in low- and middle-income countries. In India, an estimated 300,000 children under five die from diarrhoeal diseases annually — largely from dehydration that is preventable with ORS. As a physician you will see diarrhoeal disease at every level of the health system: at the PHC, in the paediatric ward, in the emergency department (dehydration shock), and in the oncology unit (chemotherapy-induced or antibiotic-associated diarrhoea). The stakes are highest in children, immunocompromised patients, and the elderly. The pharmacological principles — when to use ORS, when to add antibiotics, when loperamide is life-saving vs life-threatening — have direct, immediate impact on outcomes.
RECALL
From Year-1 physiology and biochemistry, recall that intestinal fluid secretion is regulated by intracellular second messengers — cAMP (stimulated by cholera toxin, VIP, prostaglandins) and cGMP (stimulated by heat-stable enterotoxins of E. coli). Elevated cAMP and cGMP activate CFTR (cystic fibrosis transmembrane conductance regulator), a chloride channel — Cl⁻ floods into the lumen, drawing Na⁺ and water with it. This is the mechanism of secretory diarrhoea. The key physiological fact for ORS: the sodium-glucose cotransporter (SGLT1) on the apical membrane of enterocytes co-transports one Na⁺ with one glucose molecule into the cell, driving osmotic water absorption. This cotransport system remains functional even when cholera toxin has maximally activated CFTR — which is why ORS works even in cholera. Recall also that the myenteric plexus uses mu-opioid receptors to regulate intestinal motility — this is the target of loperamide.
Pathophysiology of Diarrhoea — Secretory, Osmotic, Inflammatory, and Motility Types
The pathophysiological mechanism of diarrhoea is the single most important determinant of treatment choice. Failure to classify diarrhoea correctly before prescribing can result in dangerous treatment decisions — particularly the use of anti-motility agents in invasive diarrhoea, which can cause toxic megacolon, bacteraemia, and haemolytic uraemic syndrome. Every pharmacotherapy decision in this module flows from correctly classifying the type of diarrhoea in front of you.
1. Secretory diarrhoea: Large-volume, watery stools without blood or mucus. The hallmark is continued stool output even when the patient is fasting (unlike osmotic diarrhoea, which resolves with fasting). Mechanism: bacterial enterotoxins (cholera toxin, E. coli LT and ST), viral infection (rotavirus — alters enterocyte brush-border enzymes + stimulates secretion), or hormonal (VIPoma — rare). cAMP- and cGMP-mediated CFTR activation drives massive Cl⁻ secretion. Stool Na⁺ is low (because the secretory fluid is essentially plasma ultrafiltrate-diluted intestinal fluid). ORS works perfectly here — SGLT1 is intact. Anti-motility agents (loperamide) reduce motility-related fluid loss and are appropriate in this non-invasive, afebrile context.
2. Osmotic diarrhoea: Diarrhoea driven by non-absorbed solutes drawing water into the lumen osmotically. Examples: lactase deficiency (lactose intolerance), malabsorption syndromes (coeliac disease, Giardia), osmotic laxatives (lactulose, MgSO₄). Resolves with fasting (once the unabsorbed solute is gone, diarrhoea stops). Treatment targets the cause; symptomatic agents offer limited benefit if the solute continues.
3. Inflammatory/invasive diarrhoea (dysentery): Small-volume, bloody/mucoid stools with tenesmus, abdominal cramps, and fever. Mechanism: mucosal invasion and inflammation by organisms such as Shigella, Campylobacter, enteroinvasive E. coli, Entamoeba histolytica, Salmonella, Clostridium difficile. The inflammation is the disease — the diarrhoea is a symptom of mucosal destruction and immune response. ANTI-MOTILITY AGENTS ARE CONTRAINDICATED HERE (loperamide, diphenoxylate): trapping the invasive organism in the colon by reducing motility promotes bacteraemia, toxic megacolon, and systemic spread. Antibiotics are the primary treatment for bacterial invasive diarrhoea.
4. Motility disorders: Diarrhoea from accelerated intestinal transit (hyperthyroidism, post-gastrectomy dumping syndrome, IBS-D, diabetic autonomic neuropathy). The mucosa is intact; the problem is dysmotility. Loperamide is appropriate here.
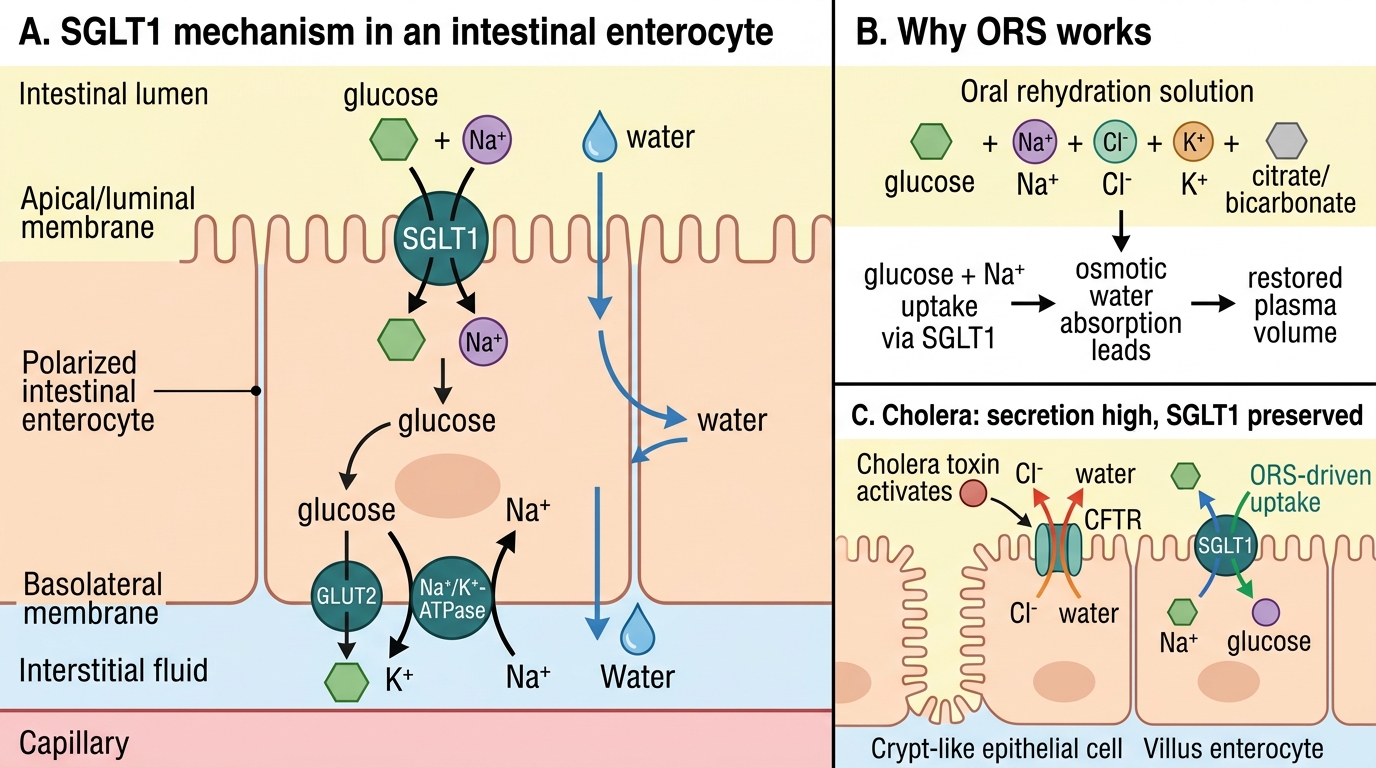
SGLT1-Mediated Oral Rehydration Mechanism
Therapeutic Goals — Acute and Chronic Diarrhoea
The therapeutic goals in diarrhoea management must be calibrated to the acuity, the aetiology, the age of the patient, and the setting. A single goal — 'stop the diarrhoea' — is not only pharmacologically naive but can cause harm if it leads to anti-motility agents being prescribed for invasive disease. The framework below prevents that error by separating what must always be done (restore fluid and electrolytes) from what is sometimes appropriate (antibiotics, anti-motility agents) and what is often counter-productive (antibiotics for viral diarrhoea, loperamide in children under 2).
For acute watery diarrhoea in all ages: the primary goal is prevention and correction of dehydration and electrolyte loss. ORS is first-line — it is not a 'second choice while waiting for antibiotics.' Anti-motility agents (loperamide) may be added in adults with non-invasive diarrhoea to reduce stool frequency and allow normal activity during travellers' diarrhoea. For acute invasive/dysenteric diarrhoea (blood, mucus, fever): the goal is pathogen eradication with the appropriate antibiotic. Anti-motility agents are actively harmful. For diarrhoea in children under 5: ORS + zinc supplementation (20 mg/day × 10–14 days) is the WHO standard. Loperamide is not recommended by the WHO for children with acute diarrhoea (insufficient evidence of benefit; risk of CNS toxicity, especially under 2). For chronic diarrhoea: the goal is identifying and treating the underlying cause (IBD, IBS-D, malabsorption, parasitic infection) — symptomatic antidiarrhoeal agents are adjuncts, not replacements for aetiology-directed therapy.
SELF-CHECK
A 3-year-old child presents with 12 episodes of watery diarrhoea in 24 hours, moderate dehydration, no blood in stools, temperature 37.2°C. Which is the MOST appropriate immediate management?
A. Loperamide 1 mg three times daily to reduce stool frequency
B. Oral rehydration solution (ORS) and zinc supplementation 20 mg/day for 14 days
C. Ciprofloxacin oral for 3 days to cover possible bacterial cause
D. IV normal saline and withhold oral fluids until diarrhoea stops
Reveal Answer
Answer: B. Oral rehydration solution (ORS) and zinc supplementation 20 mg/day for 14 days
ORS is the cornerstone of management for acute watery diarrhoea in children. The WHO/UNICEF protocol for children under 5 is ORS for rehydration + zinc 20 mg/day for 10–14 days (zinc reduces the duration and severity of the episode and prevents recurrence for 2–3 months by restoring intestinal mucosal immunity). Loperamide is not recommended by WHO in children with acute diarrhoea — it carries CNS toxicity risk (BBB more permeable in young children) and is absolutely contraindicated under 2 years. Ciprofloxacin is not indicated for non-bloody, afebrile watery diarrhoea without bacteriological evidence. IV fluids are for severe dehydration — moderate dehydration with an alert child is managed with ORS.
Classification of Antidiarrhoeal Agents
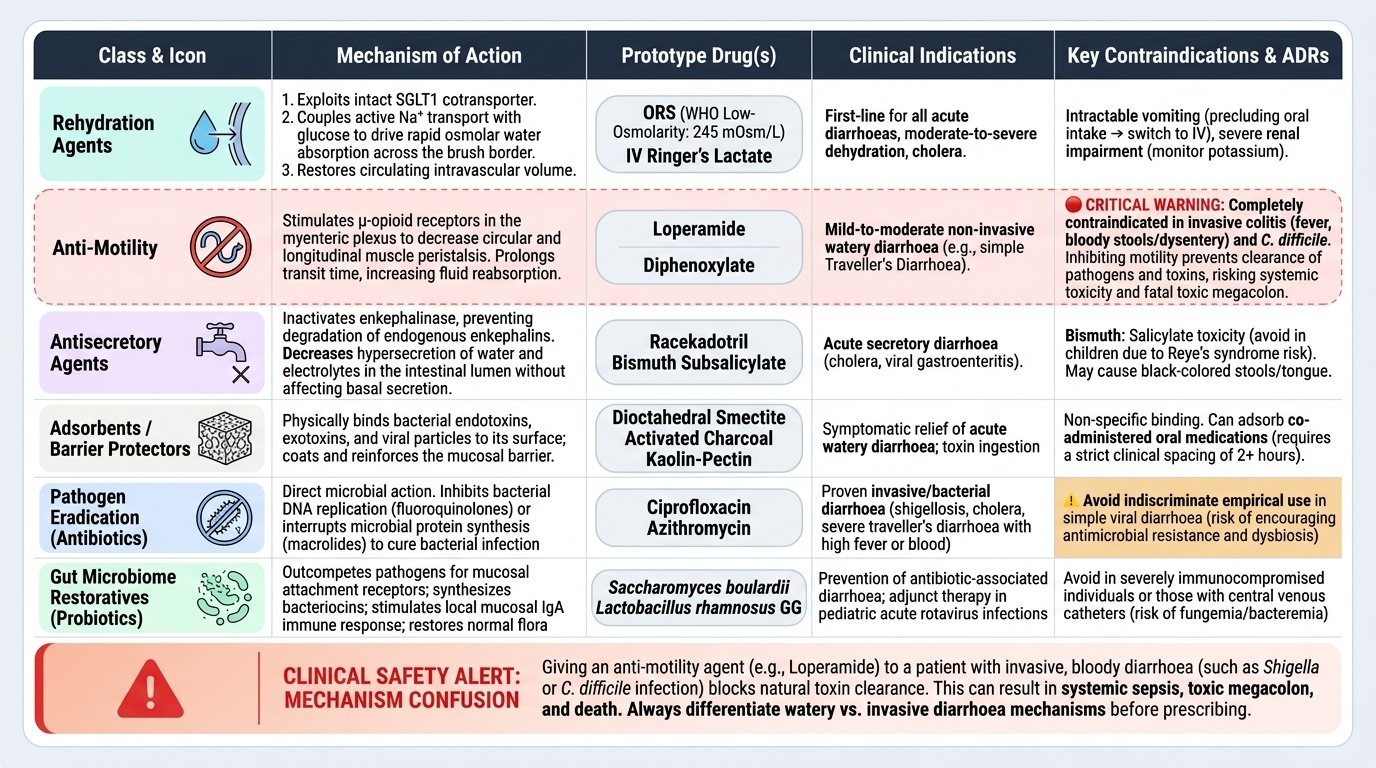
Antidiarrhoeal agents form a heterogeneous group that act through fundamentally different mechanisms — rehydration, motility inhibition, secretion reduction, pathogen binding or eradication, or restoration of the intestinal microbiome. A clear classification is essential because the wrong mechanism applied to the wrong type of diarrhoea is not just ineffective but potentially fatal. This is one of the few areas in clinical pharmacology where a prescribing error based on mechanism confusion — giving an anti-motility agent to a patient with invasive colitis — carries life-threatening consequences. Every practitioner who manages diarrhoea must be able to map a drug to its class and from the class immediately know its indications and contraindications without looking them up under emergency conditions.
Antidiarrhoeal agents form a heterogeneous group that act through fundamentally different mechanisms — rehydration, motility inhibition, secretion reduction, pathogen binding or eradication, or restoration of the intestinal microbiome. A clear classification is essential because the wrong mechanism applied to the wrong type of diarrhoea is not just ineffective but potentially fatal. This is one of the few areas in clinical pharmacology where a prescribing error based on mechanism confusion (giving an anti-motility agent to a patient with invasive colitis) carries life-threatening consequences.
The full classification of antidiarrhoeal agents by mechanism:
1. Rehydration agents:
- Oral rehydration solution (ORS) — WHO low-osmolarity formula (245 mOsm/L); exploits the intact SGLT1 cotransporter to drive Na⁺ and water absorption.
- IV fluids (normal saline, Ringer's lactate) — for severe dehydration, vomiting precluding oral intake, or shock.
2. Anti-motility agents:
- Loperamide — peripheral mu-opioid agonist; reduces motility + increases sphincter tone; no CNS effects at therapeutic doses.
- Diphenoxylate + atropine — mixed opioid + anticholinergic; partial CNS access; atropine added in subtherapeutic dose to deter abuse (causes dysphoria/dry mouth if supra-therapeutic doses taken).
3. Antisecretory agents:
- Racecadotril (acetorphan) — enkephalinase inhibitor; prevents breakdown of enkephalins in the gut → reduced cAMP-driven Cl⁻ secretion. No anti-motility effect; preferred antisecretory in children (WHO-endorsed alternative to loperamide in paediatric acute diarrhoea).
4. Adsorbents/mucosal protectants:
- Kaolin-pectin — adsorbs toxins and bacteria in the gut lumen; reduces stool water content (more cosmetic than curative).
- Bismuth subsalicylate — anti-secretory + mild anti-bacterial; used for travellers' diarrhoea mild cases and as part of H. pylori quadruple therapy.
5. Antimicrobial agents — pathogen-matched; see dedicated heading.
6. Probiotics — Lactobacillus species, Saccharomyces boulardii — reduce duration of acute infective diarrhoea by 1 day; useful in antibiotic-associated diarrhoea prevention.
Provided image