Page 13 of 26
PH6.4 | PH6.4 | Constipation Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Classify laxatives by their mechanism of action into bulk-forming, osmotic, stimulant, softener, and newer secretagogue groups
- Explain the pharmacological basis of ORS-mediated water absorption versus osmotic laxative-mediated water secretion into the gut lumen
- Identify the contraindications and ADRs of key laxative agents including bisacodyl, liquid paraffin, and stimulant laxatives in pregnancy
- Devise a stepwise management plan for chronic constipation, opioid-induced constipation, and constipation in pregnancy
- Distinguish the mechanisms of lubiprostone (ClC-2) and linaclotide (GC-C) from older laxative classes
INSTRUCTIONS
Constipation is among the most prevalent symptoms in clinical practice, affecting 14–17% of the global population and significantly impairing quality of life. It is also one of the most frequently mismanaged conditions — both undertreated (patients suffer in silence) and overtreated (inappropriate chronic stimulant laxative use causing dependence). This module provides the mechanistic pharmacological knowledge that enables rational laxative selection — matching the drug's mechanism to the pathophysiology of constipation in each clinical context.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 49 (Laxatives and Cathartics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch. 50 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients come to your outpatient clinic with constipation. The first is an 82-year-old woman on morphine for cancer pain who has not had a bowel movement in 6 days. The second is a 28-year-old woman at 20 weeks' gestation with hard, infrequent stools and fear of taking medication. The third is a 45-year-old man who has been taking senna tablets daily for 3 years for 'bowel regulation' and now finds he cannot pass stool without them. Each patient has constipation — but each requires a different pharmacological approach. The first needs an agent specifically designed for opioid-induced constipation. The second needs a safe option that will not harm the foetus. The third has laxative dependence and needs a plan for gradual withdrawal and replacement with a safe long-term agent. By the end of this module, you will have the pharmacological knowledge to manage all three.
WHY THIS MATTERS
Constipation is not a trivial complaint. In elderly patients, constipation causes faecal impaction, overflow diarrhoea, urinary retention, and falls (straining at stool causing Valsalva syncope). In hospitalised patients on opioids — a significant fraction of any medical or oncology ward — untreated opioid-induced constipation is so distressing that some patients reduce their analgesic dose, accepting pain to avoid the bowel symptoms. In pregnancy, constipation is near-universal, and the wrong laxative choice (stimulant anthraquinones with potential uterotonic effects) can have fetal consequences. Understanding the pharmacological classification of laxatives and matching each agent to the correct indication is a genuinely practical skill with daily clinical application.
RECALL
From your Year-1 physiology, recall that the colon is the primary site of water reabsorption from intestinal contents — approximately 1.5 litres of fluid enters the colon daily and only 100–200 mL is excreted in faeces. This efficient reabsorption is driven by active Na⁺ transport (via epithelial sodium channels, ENaC) with water following osmotically. Colonic transit time determines how much water is reabsorbed — slow transit results in hard, desiccated stools. The enteric nervous system (Meissner's/submucosal plexus + Auerbach's/myenteric plexus) controls peristaltic contractions; stimulant laxatives act directly on these plexuses. Recall also that chloride secretion into the gut lumen (via CFTR and ClC-2 channels) draws water into the lumen — the mechanism exploited by newer secretagogues (lubiprostone, linaclotide). The opposite of osmotic laxatives pulling water into the lumen is ORS exploiting SGLT1 to absorb water from the lumen — a conceptual pair that reinforces both mechanisms.
Pathophysiology of Constipation
Constipation is among the most prevalent gastrointestinal complaints in clinical practice, yet it is also one of the most misdiagnosed and undertreated — partly because patients underreport it (considering it embarrassing) and partly because physicians underestimate its impact on quality of life, especially in elderly and opioid-treated patients. Before prescribing any laxative, the physician must first determine whether the constipation is primary (functional) or secondary to an identifiable, treatable cause — because laxatives treat the symptom, not the cause, and in secondary constipation (hypothyroidism, opioids, hypercalcaemia, colorectal cancer), symptomatic treatment without addressing the cause is both incomplete and potentially dangerous (e.g., a new-onset constipation in an elderly patient that is actually a sign of colorectal malignancy).
Constipation is defined clinically as fewer than 3 spontaneous complete bowel movements per week, or the presence of straining, hard stools, sensation of incomplete evacuation, or need for manual manoeuvres — with at least 2 of these symptoms present for ≥12 weeks in the preceding year (Rome IV criteria). Normal bowel frequency ranges from 3 times per day to 3 times per week — this wide range is important for patient counselling, as many patients define 'constipation' incorrectly as anything less than daily stools.
Primary (functional) constipation includes three subtypes:
- Slow-transit constipation: reduced colonic propulsive activity (low-amplitude propagated contractions). Often responds to lifestyle interventions and stimulant laxatives.
- Defaecatory (outlet) dysfunction / pelvic floor dyssynergia: the external anal sphincter paradoxically contracts rather than relaxes during attempted defaecation; pharmacological laxatives do not help here — biofeedback therapy is first-line.
- IBS-C (constipation-predominant IBS): constipation with abdominal pain/discomfort that improves with defaecation; newer secretagogues (linaclotide, lubiprostone) address both components.
Secondary constipation (must identify and treat the cause):
- Drugs (most common secondary cause in hospitalised patients): opioids (mu-opioid receptors in myenteric plexus → reduced propulsive motility — the most clinically important), anticholinergics (TCA, antipsychotics, antihistamines), calcium channel blockers (verapamil most prominent), iron supplements, antacids (Al(OH)₃).
- Metabolic/endocrine: hypothyroidism (myxoedematous colon), hypercalcaemia, hypokalaemia.
- Neurological: Parkinson's disease (intrinsic enteric neuropathy + dopaminergic medication effects), spinal cord injury, multiple sclerosis.
- Structural: colorectal cancer (new-onset constipation in an elderly patient requires colonoscopy), diverticular stricture, Hirschsprung's disease (children).
The clinical implication: before prescribing a laxative, identify and address the secondary cause. Treating hypothyroid constipation with laxatives without replacing thyroxine is symptomatic management of a correctable cause.
Therapeutic Goals in Constipation Management
The therapeutic goals in constipation management must be negotiated with the patient, because 'normal' bowel function varies widely and patient expectations often differ from physiological reality. An overly rigid therapeutic goal (daily bowel movement for every patient) can lead to chronic laxative overuse; an insufficiently ambitious goal (accepting hard, infrequent stools) causes ongoing suffering and complications.
The primary goals are: (1) restore comfortable, complete defaecation with soft stools occurring at least 3 times per week; (2) relieve associated symptoms — straining, bloating, abdominal discomfort, sensation of incomplete evacuation; (3) identify and treat the secondary cause if present; (4) avoid laxative dependence — stimulant laxatives should be short-term rescue agents, not indefinite daily maintenance.
A stepwise therapeutic approach is the standard of care:
- Step 1: Lifestyle first — increase dietary fibre (25–30 g/day), adequate fluid intake (1.5–2 L/day), regular physical activity, timed toileting after meals (exploiting the gastrocolic reflex).
- Step 2: Bulk-forming or osmotic laxatives — for patients not responding to lifestyle measures; safe for long-term use; preferred for chronic constipation.
- Step 3: Stimulant laxative — for acute episode relief or as short-term adjunct; not for indefinite daily use.
- Step 4: Newer agents — lubiprostone, linaclotide, or prucalopride for refractory constipation or IBS-C after conventional agents fail.
- Specific interventions: opioid-induced constipation → peripherally acting mu-opioid antagonists (PAMORA: methylnaltrexone, naloxegol) — block the gut mu-opioid receptor without reversing central analgesia.
SELF-CHECK
A 70-year-old man on morphine 30 mg twice daily for cancer pain develops severe constipation despite adequate dietary fibre and regular PEG. He has not passed stool in 8 days. Which agent specifically targets the mechanism of opioid-induced constipation?
A. Lactulose 30 mL twice daily — osmotic laxative will overcome the opioid effect
B. Senna 2 tablets at night — stimulate the myenteric plexus directly
C. Methylnaltrexone subcutaneously — peripheral mu-opioid antagonist that blocks gut opioid receptors without reversing analgesia
D. Stop morphine and switch to a non-opioid analgesic
Reveal Answer
Answer: C. Methylnaltrexone subcutaneously — peripheral mu-opioid antagonist that blocks gut opioid receptors without reversing analgesia
Opioid-induced constipation (OIC) is caused by mu-opioid receptor activation in the enteric nervous system — reducing propulsive contractions and increasing anal sphincter tone. Methylnaltrexone is a peripherally acting mu-opioid receptor antagonist (PAMORA): its high polarity prevents it from crossing the BBB, so it blocks mu-opioid receptors in the gut but not in the CNS. This reverses the constipating effect of opioids without reversing their analgesic effect. Standard laxatives (lactulose, senna, PEG) address stool consistency and colonic secretion but do not block the causative receptor mechanism — they are often inadequate in severe OIC. Stopping morphine in a cancer patient is not appropriate when OIC can be managed pharmacologically.
Classification of Laxatives
Laxatives are classified by their primary mechanism of action — a classification that directly guides clinical selection because it maps each class to the physiological variable it targets: stool bulk, luminal osmolality, motor activity, ion-channel secretion, or prokinetic stimulation. This is not academic taxonomy — it determines which drug will work for a given patient's pathophysiology, which ones are safe for long-term use, and which ones carry specific risks that must be communicated. A prescriber who cannot classify laxatives by mechanism will default to prescribing stimulant laxatives for every indication because they are the fastest-acting, leading to dependence, enteric neuropathy, and missed opportunities to use safer long-term alternatives.
Laxatives are classified by their primary mechanism of action — a classification that directly guides clinical selection because it maps each class to the physiological variable it targets (stool bulk, luminal osmolality, motor activity, or secretion). Understanding the full taxonomy prevents both errors of omission (not knowing that newer secretagogues exist for refractory constipation) and errors of commission (using liquid paraffin long-term when safer alternatives exist).
The full classification of laxatives by mechanism:
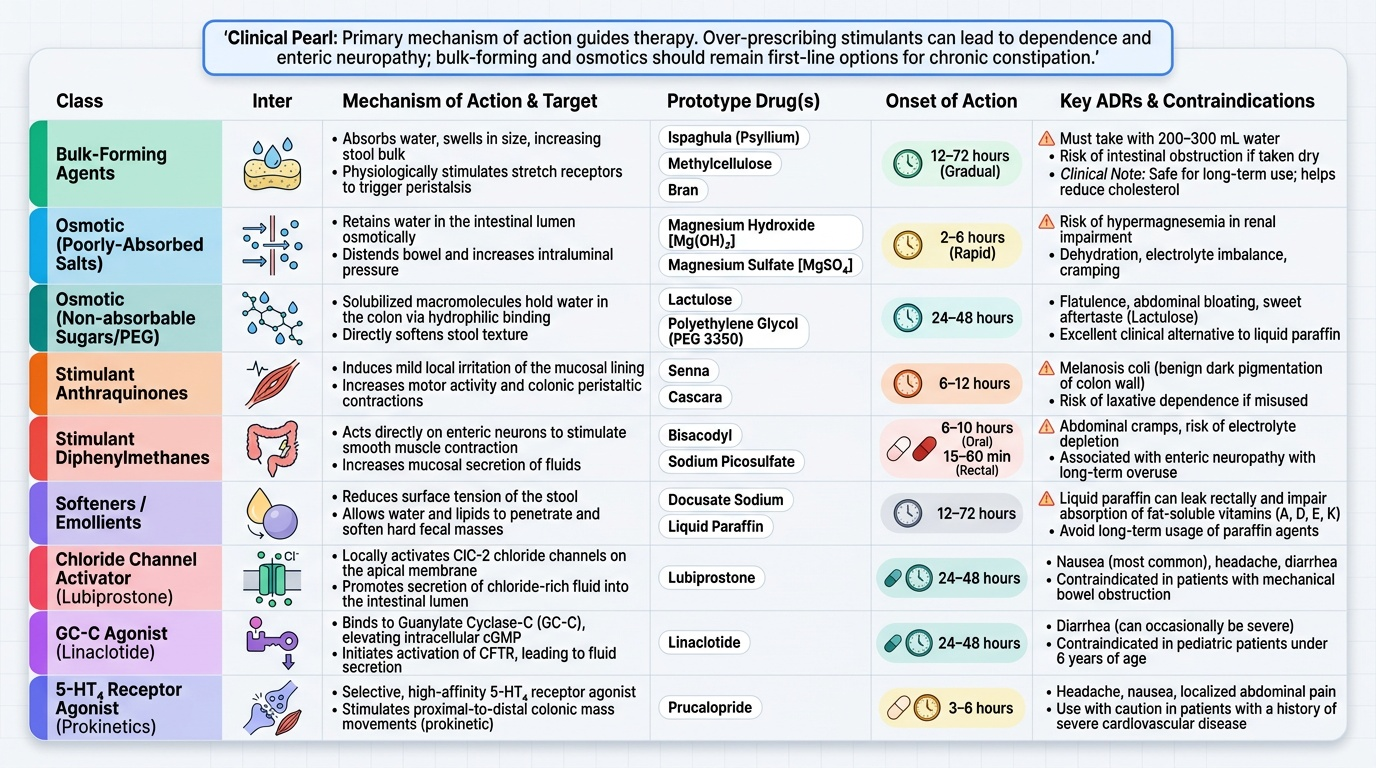
1. Bulk-forming agents:
- Ispaghula (psyllium husk), methylcellulose, bran.
- Mechanism: absorb water and swell → increase stool bulk → stimulate peristalsis physiologically.
- Must be taken with adequate water (at least 200–300 mL); risk of intestinal obstruction if taken dry.
- Safest class for long-term use; also reduce cholesterol (psyllium) and improve glycaemic control.
2. Osmotic agents:
- Poorly absorbed salts: Mg(OH)₂ (milk of magnesia), MgSO₄ (Epsom salt), sodium phosphate enema — rapid osmotic water draw into lumen; short-term/rescue use; avoid in renal failure (Mg²⁺ or PO₄³⁻ accumulation).
- Non-absorbable sugars/alcohols: Lactulose (fermented by colonic bacteria → SCFA + gas; acidifies colon for hepatic encephalopathy; onset 24–48 h; gas/bloating common ADR); Sorbitol; PEG/macrogol (inert polymer, not fermented, no gas, preferred for long-term use and bowel prep).
3. Stimulant/irritant laxatives:
- Anthraquinone glycosides: Senna (sennosides), cascara — converted to active anthranols by colonic bacteria; stimulate myenteric plexus → increased propulsive contractions; onset 6–12 h oral; safe in short courses.
- Diphenylmethane derivatives: Bisacodyl — converted to active form by gut bacteria and intestinal esterases; stimulates myenteric plexus; oral (onset 6–12 h) and rectal suppository (onset 30–60 min); sodium picosulfate (similar mechanism, used in bowel prep).
4. Stool softeners:
- Docusate sodium — anionic surfactant; reduces stool surface tension; allows water and fat to penetrate stool; mild effect; used with stimulant for opioid-induced constipation.
- Liquid paraffin (mineral oil) — lubricant laxative; coats stool; NOT recommended for long-term use: risk of aspiration pneumonia (lipoid pneumonia), impairs absorption of fat-soluble vitamins (A, D, E, K), soils clothing (anal leakage). Largely replaced by safer agents.
5. Newer secretagogues:
- Lubiprostone — ClC-2 channel activator (apical Cl⁻ secretion → water follows into lumen); approved for chronic idiopathic constipation and IBS-C; nausea is the main ADR.
- Linaclotide — GC-C (guanylate cyclase-C) receptor agonist; increases cGMP → activates CFTR + inhibits visceral pain afferents; approved for IBS-C and chronic idiopathic constipation; diarrhoea is the main ADR.
6. Colonic prokinetics:
- Prucalopride — selective high-affinity 5-HT₄ receptor agonist; promotes high-amplitude propagated contractions in the colon; approved for chronic constipation in adults who have not responded to other laxatives.
Provided image