Page 14 of 25
PH1.10 | PH1.10 | Individualized Pharmacotherapy in Special Populations — SDL Guide — SDL Guide
Learning Objectives
- Describe the pharmacokinetic and pharmacodynamic differences in paediatric patients and explain weight-based dosing principles.
- Explain age-related changes in drug handling in geriatric patients and identify drugs requiring dose adjustment or avoidance.
- Describe physiological changes in pregnancy that alter drug pharmacokinetics and classify drugs by teratogenic risk.
- Identify drugs safe and contraindicated during breastfeeding and explain the milk:plasma ratio concept.
- Apply the Cockcroft-Gault equation to estimate renal function and adjust drug doses in renal and hepatic impairment.
INSTRUCTIONS
The dose listed in a pharmacopoeia was derived from studies in healthy, average-weight adults — a population that excludes the very young, the very old, the pregnant, and those with organ impairment. Yet these are precisely the patients who most frequently need drugs. A dose that is therapeutic in a 35-year-old with normal kidneys may be toxic in a 75-year-old with reduced GFR, negligible in a neonate whose enzymes cannot yet metabolise it, or teratogenic in a 22-year-old in her first trimester. Individualising drug therapy for special populations is not a refinement — it is a foundational clinical skill.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 5 (Special Pharmacology) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 4-5 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-day-old neonate is admitted to the NICU with a serious gram-negative infection. The neonatologist reaches for chloramphenicol — a broad-spectrum antibiotic that was the treatment of choice for such infections before the era of third-generation cephalosporins. In the 1950s, before the PK differences of neonates were understood, babies given 'adult-proportional' doses of chloramphenicol developed a characteristic syndrome: grey skin colour, abdominal distension, vomiting, cardiovascular collapse, and death. The culprit was not the antibiotic's pharmacodynamics — it was the neonate's immature liver, unable to glucuronidate chloramphenicol, allowing the drug to accumulate to toxic levels. Grey baby syndrome was pharmacokinetics killing patients. This module exists so that does not happen on your watch.
WHY THIS MATTERS
Prescribing errors are among the most preventable causes of patient harm, and errors in special populations are disproportionately represented. Neonates and young children have PK profiles that differ fundamentally from adults; the elderly are the largest consumers of prescription drugs yet were largely excluded from the RCTs that established dosing guidelines; pregnant women require drugs for pre-existing conditions but face teratogenic risks that must be balanced against untreated disease risks for both mother and foetus; patients with renal or hepatic impairment accumulate drugs that healthy patients eliminate efficiently. The NMC competency framework explicitly requires that every Indian graduate be able to describe these changes and adjust treatment accordingly — because in each of these patient groups, the default adult dose is a starting point that requires active modification.
RECALL
From the ADME SDL (PH1.6), you know that drug elimination depends primarily on renal excretion (GFR + tubular secretion − reabsorption) and hepatic metabolism (Phase I CYP450 and Phase II conjugation). Both processes are immature in neonates, reduced in the elderly, altered in pregnancy, and impaired in hepatic or renal disease. From the formulations and routes SDL, you know that volume of distribution depends on body water and fat composition, which differ substantially across age groups and physiological states. These PK building blocks are what make dose adjustment in special populations a systematic, derivable skill rather than a set of memorised exceptions.
Why the 'Average Patient' Dose Does Not Fit All Patients
Standard drug dosing recommendations are derived from Phase III clinical trials conducted predominantly in healthy adults between 18 and 65 years of age, with normal renal and hepatic function, who are not pregnant, and who are not taking multiple interacting drugs. This is a pragmatic but narrow population. When a drug is prescribed to a patient outside this profile — a 3-week-old, an 84-year-old with a creatinine of 3.2 mg/dL, a woman at 22 weeks of gestation, or a patient with Child-Pugh C cirrhosis — the pharmacokinetic and pharmacodynamic assumptions built into the standard dose may no longer hold.
The consequences of failing to adjust doses in special populations are not hypothetical. Grey baby syndrome (chloramphenicol in neonates — described in the hook) was a preventable drug toxicity caused by immature glucuronidation. Thalidomide embryopathy (foetal limb malformations from a 'safe' sedative given to pregnant women in the 1950s–60s) triggered the modern teratogenicity classification system. Gentamicin nephrotoxicity in patients with pre-existing renal impairment occurs predictably when doses are not reduced for reduced GFR. Each of these was a pharmacokinetics problem that clinical knowledge could have prevented.
The framework for special population dosing rests on two questions: (1) How does this patient's physiology alter the drug's pharmacokinetics? and (2) How do I adjust the dose, route, formulation, or frequency to compensate? Answering both requires a patient-specific understanding of absorption, distribution, metabolism, and excretion — which is why this SDL is placed after the ADME module in the teaching sequence.
Therapeutic Goals: Individualised Dosing to Maintain the Therapeutic Window
The therapeutic goal in all special populations is identical to the goal in any other patient: maintain the drug's plasma concentration within the therapeutic window — above the minimum effective concentration and below the minimum toxic concentration — throughout the dosing interval. What changes is the dosing strategy required to achieve this, because the pharmacokinetic parameters (Vd, CL, t½) are different.
Three general dosing adjustment strategies are used in special populations. The first is weight-based dosing (mg/kg), used primarily in paediatrics, where the absolute organ masses and body fluids scale with body weight. A child weighing 20 kg requires approximately 20/70 = 29% of an adult dose (by body weight fraction), though this is a rough approximation — immature enzymes may require further reduction and reduced clearance prolongs effect. The second is organ-function-adjusted dosing, used in renal and hepatic impairment: the dose is reduced (or interval extended) proportionally to the reduction in the relevant clearance organ's function, using validated equations such as the Cockcroft-Gault formula for renal clearance or Child-Pugh score for hepatic function. The third is age-adjusted empirical modification, used in geriatrics and pregnancy, where quantitative organ function may be relatively preserved but physiological changes (altered body composition, protein binding, GI motility) alter distribution and absorption in ways that require prescribing caution and monitoring.
All three strategies share a common principle: the standard dose is a reference point, not a fixed prescription, and the prescriber's responsibility is to adjust it for the individual patient and monitor the response.
Paediatric Pharmacology: Age-Dependent PK and Dose Calculation
Paediatric pharmacology is not simply scaled-down adult pharmacology. Children — and especially neonates and infants — differ from adults in ways that profoundly alter all four phases of ADME, and some of these differences are not merely quantitative but qualitative.
Absorption in neonates is altered by reduced gastric acid secretion (higher gastric pH than adults → acid-labile drugs better absorbed, acid-stable drugs less reliably absorbed), delayed gastric emptying, and reduced intestinal motility. Topical absorption is increased because neonatal skin is thinner and more permeable — corticosteroid creams applied to large skin areas can cause systemic effects.
Distribution is affected by neonatal body composition: neonates have a higher proportion of total body water (75–80% vs 55–60% in adults), a lower proportion of body fat, and lower plasma albumin and alpha-1-acid glycoprotein. Higher body water fraction means a larger Vd for water-soluble drugs (requiring relatively higher mg/kg doses). Lower protein binding means a higher free drug fraction for highly protein-bound drugs — relevant for drugs like phenytoin.
Metabolism is the most critical PK difference in neonates. The CYP450 enzyme system is incompletely developed at birth; CYP3A7 (fetal isoform) is expressed but CYP3A4 (the dominant adult isoform) reaches adult activity only at 6–12 months. Phase II glucuronidation (UGT enzymes) is particularly immature in neonates — reaching adult levels only at 6–18 months depending on the enzyme. This immaturity directly caused 'grey baby syndrome': chloramphenicol is normally glucuronidated and excreted renally, but neonates cannot glucuronidate it efficiently. Chloramphenicol accumulates to toxic levels, causing cardiovascular collapse and the characteristic grey discolouration.
Excretion via the kidneys is also immature: neonatal GFR is ~20–40% of adult values (corrected for body surface area), reaching adult levels by 6–12 months. Renally eliminated drugs (aminoglycosides, penicillins, vancomycin) require substantially reduced doses and extended intervals in neonates.
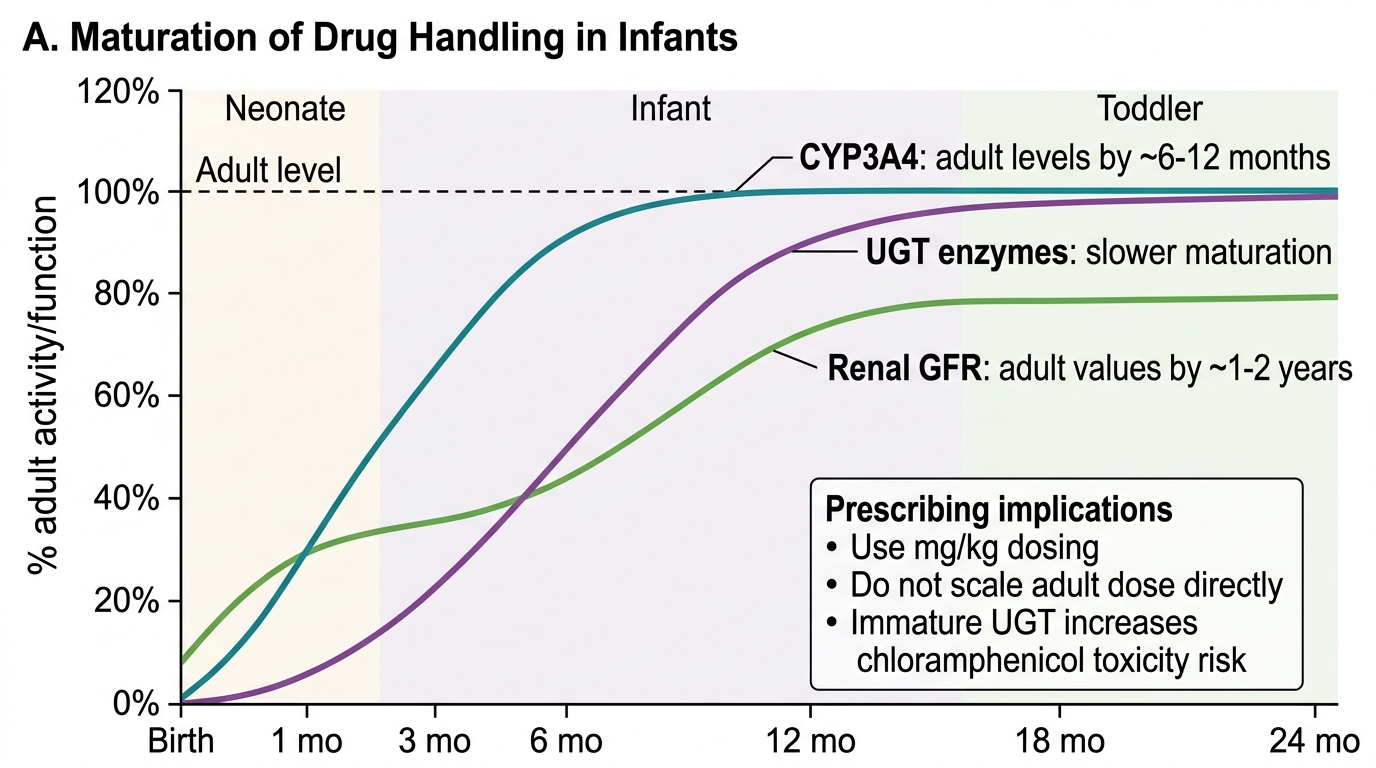
Maturation of Drug Metabolism and Excretion in Infants
Clinical rules for paediatric prescribing:
- Always use weight-based dosing (mg/kg) for children. Never simply halve or quarter an adult dose.
- Use age-specific formulations (liquids and dispersible tablets for young children; solid forms with swallowing capability from approximately 6 years).
- Tetracyclines are contraindicated in children under 8 years and in pregnancy — they chelate calcium in developing bones and teeth, causing permanent discolouration ('staining') and impaired bone growth. This is a pharmacodynamic (not PK) contraindication.
- Aspirin is contraindicated in children under 16 with viral illness due to risk of Reye's syndrome — a rare but severe hepatic encephalopathy associated with aspirin use in viral infections.
SELF-CHECK
A neonate develops grey discolouration, cardiovascular instability, and abdominal distension after chloramphenicol was prescribed at an adult-equivalent weight-based dose. The most likely pharmacokinetic mechanism is:
A. Increased renal excretion of chloramphenicol in neonates, reducing plasma levels to toxic range.
B. Immature hepatic glucuronidation (UGT enzymes) in neonates prevents chloramphenicol conjugation, causing toxic drug accumulation in plasma and tissues.
C. Increased plasma protein binding in neonates traps chloramphenicol, releasing it suddenly and causing toxicity.
D. CYP3A4 over-expression in neonates converts chloramphenicol to a toxic metabolite not seen in adults.
Reveal Answer
Answer: B. Immature hepatic glucuronidation (UGT enzymes) in neonates prevents chloramphenicol conjugation, causing toxic drug accumulation in plasma and tissues.
Grey baby syndrome is caused by immature hepatic UGT (UDP-glucuronosyltransferase) enzymes in neonates. Chloramphenicol is normally glucuronidated in the liver and excreted renally. In neonates, glucuronidation capacity is 5–10% of adult levels at birth, so the parent compound accumulates to toxic plasma concentrations. The syndrome was the driving case for recognising that neonates require not just weight-proportional doses but enzyme-maturation-adjusted doses.