Page 17 of 25
PH1.11-13 | PH1.11-13 | Adverse Drug Reactions, Pharmacovigilance and Drug Interactions — SDL Guide — SDL Guide
Learning Objectives
- Define adverse drug reactions (ADRs) and classify them using the A–E type framework.
- Assess causality of a suspected ADR using the WHO-UMC categories and the Naranjo Algorithm.
- Describe pharmacovigilance, its goals, and the structure of India's Pharmacovigilance Programme (PvPI), and demonstrate ADR reporting.
- Classify drug interactions as pharmacokinetic, pharmacodynamic, or pharmaceutical and explain the mechanisms of clinically important interactions.
- Apply a systematic approach to identify, manage, and report ADRs and drug interactions in a clinical scenario.
INSTRUCTIONS
Every drug causes adverse effects in some patients at some doses — the question is not whether ADRs exist but whether the prescriber knows how to recognise them, classify them, assess whether the drug caused them, report them, and prevent dangerous interactions. Pharmacovigilance is the organised scientific discipline that answers these questions at the population level. This SDL gives you the individual-patient clinical skills (ADR recognition, causality assessment, interaction management) and the public health reporting obligation (India's PvPI) that together constitute the safety arm of rational pharmacotherapy.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 6 (Adverse Drug Reactions) and Ch 7 (Drug Interactions) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 5 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman on carbamazepine for trigeminal neuralgia develops a painful blistering rash covering 30% of her body surface area. The dermatologist diagnoses Stevens-Johnson syndrome (SJS). Is this an ADR? Was the drug the cause? Should it be stopped? Does anyone need to be notified? As you work through the answers, you are practising pharmacovigilance at the bedside: identifying an adverse event, assessing causality, making a clinical decision, and initiating a report to the drug safety system. This is one of the most important clinical scenarios you will encounter — and it is entirely governed by the principles in this SDL.
WHY THIS MATTERS
Adverse drug reactions are not rare edge cases — they account for approximately 5–10% of all hospital admissions globally and are estimated to be the 4th to 6th leading cause of in-hospital death in developed countries. In India, a country with one of the world's highest prescription drug burdens and widespread over-the-counter antibiotic use, the ADR burden is substantial and systematically under-reported. The NMC explicitly includes ADR reporting as a clinical competency because every prescriber has both a professional and a legal obligation to report suspected ADRs to the Pharmacovigilance Programme of India (PvPI). Drug interactions are equally pervasive: a patient on four drugs has a >40% probability of experiencing at least one drug-drug interaction. Recognising and managing these interactions is a daily clinical skill.
RECALL
From the ADME SDL (PH1.6), you know that CYP450 enzyme induction and inhibition alter the plasma levels of co-administered drugs — this is the mechanistic basis of the majority of pharmacokinetic drug interactions. From the pharmacodynamics SDL (PH1.9), you know that synergism and antagonism between drugs produce combined effects greater or lesser than either drug alone — this is pharmacodynamic interaction. From the rational drug use SDL (PH1.2), you know that rational prescribing includes selecting drugs whose risk-benefit ratio is acceptable — which requires knowing what adverse effects to expect and monitoring for them.
When Drugs Harm: Framing the Safety Problem
An adverse drug reaction (ADR) is defined by the WHO as: 'a response to a drug which is noxious and unintended, and which occurs at doses normally used in man for prophylaxis, diagnosis, or therapy of disease, or for the modification of physiological function.' This definition distinguishes ADRs from three other categories of drug harm that are sometimes confused with them: (1) medication errors — harm caused by the wrong drug, wrong dose, or wrong route (prescribing or administration error — preventable and not an ADR by definition); (2) drug dependence and misuse — use beyond the prescribed therapeutic context; and (3) overdose toxicity — effects at doses above the therapeutic range.
The scale of the ADR problem justifies making it a clinical priority. An estimated 3.5–10% of all hospital admissions in developed countries are attributed to ADRs. A landmark study in the Lancet (Pirmohamed et al., 2004) found that 6.5% of all hospital admissions in the UK were ADR-related, and 72% of these ADRs were judged preventable. In India, the ADR burden is incompletely characterised because of historical under-reporting, but data from PvPI and hospital-based studies consistently identify antimicrobials, antiepileptics, NSAIDs, and cardiovascular drugs as the drug classes most frequently associated with reported ADRs.
As a prescriber, every new symptom in a patient on drug therapy should trigger the question: 'Could this be an adverse drug reaction?' The clinical discipline of answering that question — from definition and classification through causality assessment and management — is what this SDL teaches.
Governing Framework: ADR Definitions and the Pharmacovigilance System
Pharmacovigilance is defined by the WHO as 'the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other drug-related problems.' It operates at three levels: the individual clinician (recognising and reporting), the national regulatory authority (aggregating and analysing reports), and the WHO international system (coordinating global signal detection across member countries).
Pharmacology's randomised clinical trials, which precede drug approval, are limited in their capacity to detect rare ADRs. A trial of 10,000 patients can detect an ADR with an incidence of 1 in 3,000 — but reactions occurring in 1 in 100,000 patients will not be detected until millions of patients are exposed post-approval. Post-marketing surveillance through pharmacovigilance fills this detection gap. The mechanism is spontaneous reporting: clinicians, pharmacists, and patients submit reports of suspected ADRs to a national collection system, which aggregates them and detects statistical signals — a disproportionate number of reports linking a drug and an adverse event.
India's Pharmacovigilance Programme (PvPI) was established by the Central Drugs Standard Control Organisation (CDSCO) in 2010 and is coordinated by the Indian Pharmacopoeia Commission (IPC) in Ghaziabad, which serves as the National Coordination Centre (NCC). The PvPI has a network of over 250 adverse drug reaction monitoring centres (AMCs) across India, including medical college hospitals. Suspected ADR reports are submitted using the CDSCO ADR reporting form (available online and at AMCs) and uploaded to the Vigiflow database, which is shared with the WHO's global pharmacovigilance database (VigiBase) in Uppsala. Healthcare professionals, patients, and the general public can all report.
Despite this infrastructure, under-reporting remains a major challenge. Studies in India consistently show under-reporting rates of 94–98% — less than 6% of suspected ADRs are formally reported. The barriers include lack of awareness of reporting pathways, uncertainty about causality ('is this definitely the drug's fault?'), time constraints, and fear of litigation. The NMC's inclusion of PvPI reporting as a competency explicitly addresses this: every Indian physician has a professional responsibility to report suspected ADRs. A report does not require certainty — a suspected association is sufficient and desirable, because the aggregated uncertainty of many reporters generates certainty at the population level.
ADR Classification by Type: A–E Framework and Clinical Recognition
The A–E classification of ADRs, developed by Rawlins and Thompson and extended by Edwards and Aronson, organises adverse drug reactions by their underlying mechanism and clinical behaviour. This classification is clinically useful because each type has distinct implications for management: Type A reactions can usually be managed by dose reduction or switching to an alternative within the same class, while Type B reactions require complete and permanent drug withdrawal with no rechallenge. Understanding the type of ADR before deciding on management prevents two common clinical errors: unnecessarily withdrawing a drug for a predictable, dose-adjustable effect; or dangerously re-prescribing a drug that caused an idiosyncratic immune-mediated reaction.
The classification also informs pharmacovigilance reporting priorities: Type B reactions — particularly new or unexpected ones — have the highest signal-detection value for post-marketing surveillance, because they are precisely the reactions that clinical trials (which enrol too few patients to detect rare immune-mediated events) cannot identify. Reporting a Type B reaction to PvPI contributes directly to the detection of safety signals that protect future patients. With this framework in mind, here are the five recognised ADR types with their key characteristics and clinical examples:
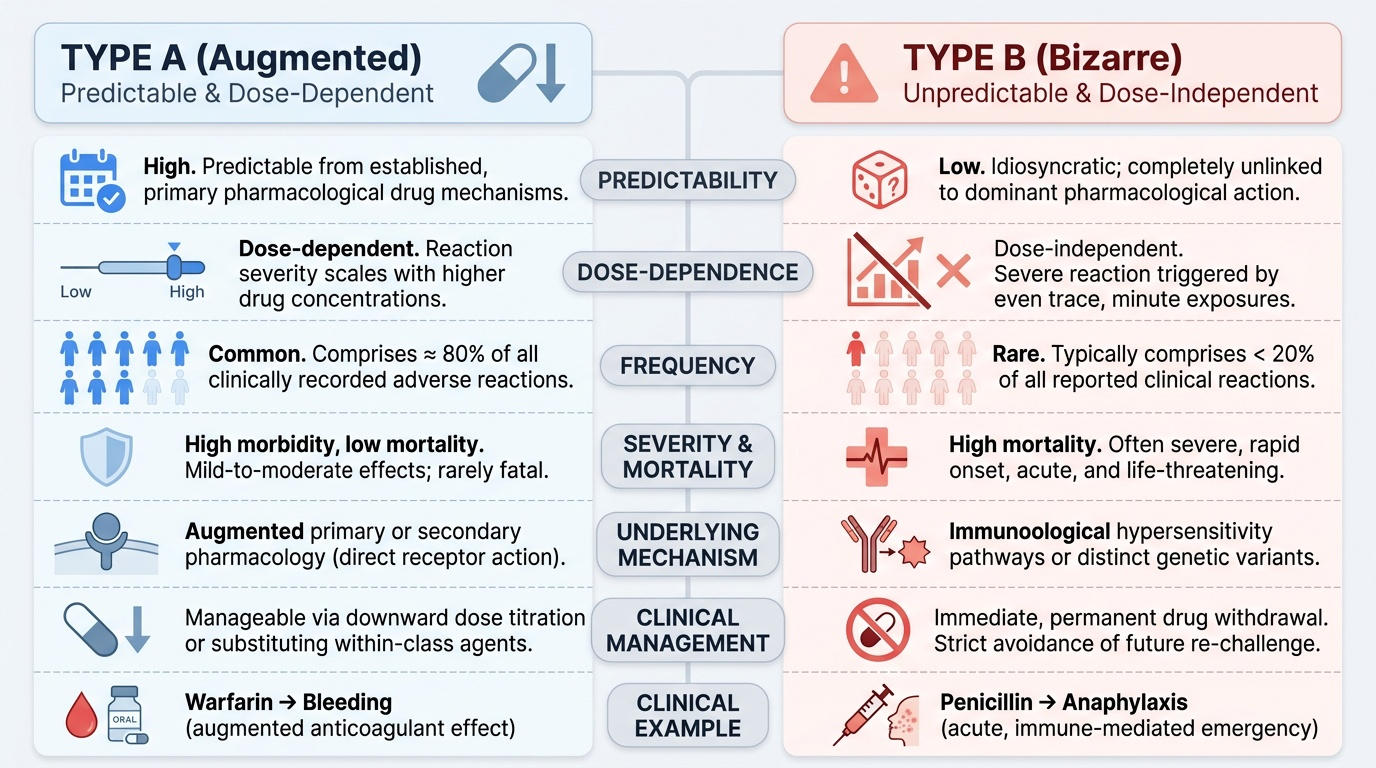
Type A (Augmented) ADRs are dose-dependent, pharmacologically predictable consequences of the drug's primary or secondary mechanism of action. They account for approximately 80% of all ADRs and are the most common type. Because they are predictable, they can usually be managed by dose reduction. Examples:
- Warfarin → bleeding (augmented anticoagulant effect at supratherapeutic doses)
- Insulin → hypoglycaemia (augmented glucose-lowering)
- Morphine → respiratory depression and constipation (augmented opioid effects)
- Beta-blockers → bradycardia and bronchospasm (augmented beta-adrenergic blockade)
Type B (Bizarre/Idiosyncratic) ADRs are dose-independent, pharmacologically unpredictable, and not related to the drug's primary mechanism. They are less common (~10–15%) but typically more severe and more frequently life-threatening. They are often immunological (IgE-mediated anaphylaxis, delayed hypersensitivity) or due to pharmacogenetic variation (unusual metabolic pathways). Management almost always requires drug withdrawal, and rechallenge is usually contraindicated. Examples:
- Penicillin → anaphylaxis (IgE-mediated type I hypersensitivity)
- Carbamazepine → Stevens-Johnson syndrome (immune-mediated — HLA-B*1502 association in Asian patients)
- Clozapine → agranulocytosis (immune-mediated bone marrow suppression)
- Halothane → halothane hepatitis (immunologically mediated hepatic necrosis)
Type C (Chronic/Cumulative) ADRs develop with prolonged use and are related to total cumulative dose. Examples: analgesic nephropathy with prolonged NSAID use; posterior column demyelination with long-term metronidazole; tardive dyskinesia with prolonged antipsychotics.
Type D (Delayed) ADRs appear long after exposure, often years. Examples: carcinogenicity (chlorambucil, cyclophosphamide causing secondary malignancies), teratogenicity (thalidomide — structural effects months after conception), and organ toxicity appearing after treatment ends.
Type E (End-of-use/Withdrawal) ADRs occur when a drug is stopped abruptly after prolonged use. Examples: benzodiazepine or alcohol withdrawal syndrome; rebound tachycardia and angina after abrupt beta-blocker withdrawal (receptor up-regulation); adrenal insufficiency after abrupt corticosteroid withdrawal.
Provided image
SELF-CHECK
A patient develops anaphylaxis after receiving IV ampicillin for the first time. She has never taken a penicillin before. This reaction is best classified as:
A. Type A — augmented penicillin effect causing vasodilation at high dose.
B. Type B — bizarre/idiosyncratic IgE-mediated hypersensitivity, dose-independent and unpredictable from the drug's mechanism.
C. Type C — cumulative toxicity from repeated penicillin exposure.
D. Type E — withdrawal phenomenon from prior antibiotic use.
Reveal Answer
Answer: B. Type B — bizarre/idiosyncratic IgE-mediated hypersensitivity, dose-independent and unpredictable from the drug's mechanism.
Penicillin anaphylaxis is a Type B (Bizarre) ADR: it is an IgE-mediated hypersensitivity reaction that is dose-independent (can occur with the first dose), pharmacologically unpredictable from penicillin's mechanism (cell wall synthesis inhibition has nothing to do with mast cell degranulation), and not related to cumulative exposure. It is caused by prior sensitisation to penicillin epitopes. The first clinical exposure may be sensitising without producing symptoms; the second exposure triggers the anaphylactic response. Management: immediate withdrawal, adrenaline, antihistamines, corticosteroids; rechallenge absolutely contraindicated.