Page 12 of 33
PH9.3 | PH9.3 | Heavy Metal Poisoning and Chelation — SDL Guide — SDL Guide
Learning Objectives
- Describe the mechanisms of toxicity for lead, mercury, arsenic, iron, and copper, with their characteristic clinical features
- Classify chelating agents by chemical type, route, target metals, and major adverse effects
- Construct a management plan for heavy metal poisoning using the correct chelating agent
- Identify contraindications in chelator use (BAL in iron/cadmium; deferoxamine for iron only) and monitoring parameters
INSTRUCTIONS
Heavy metal poisoning is a serious but often under-recognised clinical problem in India — lead exposure from old paint and informal industry, arsenic in groundwater in parts of West Bengal and Bihar, mercury in artisanal goldsmithing communities, and iron overdose in children who ingest iron tablets. Chelation pharmacology has a precise logic: each chelator forms a stable complex with specific metals and enhances their excretion. Getting the metal-chelator pairing correct is the difference between effective treatment and potentially worsening toxicity (e.g. BAL in iron poisoning causes a toxic complex). This module teaches you both the toxicology and the pharmacological rationale.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 63 (Heavy Metal Poisoning and Chelating Agents) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 4 (Principles of Toxicology) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 3-year-old boy is brought by his parents with a history of developmental regression — he was speaking in sentences at 18 months but has progressively lost words over the past year and now seems irritable and lethargic. He lives in a house with old, chipped paint. Physical examination reveals anaemia, and a blood film shows basophilic stippling of red cells. His blood lead level is 68 mcg/dL. This child has chronic plumbism — lead poisoning from paint ingestion (pica). The tragic part: cognitive deficits from childhood lead exposure are partly irreversible even after chelation, because the brain is permanently damaged during its critical developmental window. Treatment must begin immediately. But which chelator, and how?
WHY THIS MATTERS
Heavy metal poisoning remains clinically relevant across a wide spectrum of Indian settings. Occupational lead and arsenic exposure affects workers in battery manufacturing, smelting, pesticide production, and groundwater-affected agricultural communities. Paediatric lead poisoning from pica (ingestion of lead paint chips, soil) is a paediatric emergency with devastating neurodevelopmental consequences. Iron overdose in young children who ingest iron-containing supplements is the most common metallic poisoning presenting to paediatric emergency departments. Wilson's disease (inherited copper metabolism disorder) is managed with lifelong D-penicillamine. Understanding both the toxicology and the precise pharmacology of chelating agents is essential for correct management and prevention of treatment-related harm.
RECALL
From Year-1 Biochemistry, recall the haem synthesis pathway: the enzyme delta-aminolevulinic acid dehydratase (delta-ALAD) converts ALA to porphobilinogen; ferrochelatase inserts iron into protoporphyrin IX to form haem. Lead inhibits both enzymes — particularly ferrochelatase — causing accumulation of protoporphyrin IX and its zinc complex, and leading to microcytic anaemia with characteristic basophilic stippling of red blood cells (stippled RNA aggregates). Also recall that many enzyme active sites contain sulfhydryl (-SH) groups that are essential for catalytic activity. Heavy metals — particularly arsenic, mercury, and lead — form stable covalent bonds with -SH groups, inactivating these enzymes. The therapeutic strategy of chelation exploits the same affinity: chelating agents contain -SH or similar metal-binding groups that compete with enzyme SH groups for the metal, forming a stable, water-soluble complex that is excreted by the kidney.
How Heavy Metals Cause Toxicity
The common molecular mechanism of most heavy metal toxicity is disruption of sulfhydryl (-SH) group function. Metals form high-affinity covalent bonds with -SH groups on enzymes, structural proteins, and cofactors — inactivating them. The enzymes affected depend on which metals penetrate which compartments and which tissues have the highest SH-containing enzyme density.
Lead (Pb): Disrupts haem synthesis by inhibiting delta-ALA dehydratase and ferrochelatase, causing anaemia with basophilic stippling. Interferes with calcium-dependent processes in neurons — competitive inhibition of Ca²⁺ transport and signalling — disrupting neurotransmitter release and axonal conduction, causing both central (encephalopathy, cognitive impairment) and peripheral (motor neuropathy, foot/wrist drop) effects.
Mercury (Hg): All three forms (elemental, inorganic, organic/methylmercury) are toxic but differ in target and uptake. Elemental mercury vapour is absorbed through the lung and crosses the blood-brain barrier causing CNS toxicity. Inorganic mercury (HgCl₂) targets the proximal renal tubule — causing tubular proteinuria, glucosuria, and in severe cases Fanconi syndrome. Organic methylmercury bioaccumulates in fish; it preferentially damages the cerebellum and sensory cortex — causing ataxia, constriction of visual fields, peripheral sensory neuropathy, deafness, and in exposed foetuses, severe neurodevelopmental damage (congenital Minamata disease).
Arsenic (As): Inhibits the pyruvate dehydrogenase complex (binds the lipoic acid -SH groups), disrupting the TCA cycle and energy production. Also uncouples oxidative phosphorylation (arsenate substitutes for phosphate, forming unstable arsenate esters that hydrolyse without generating ATP). Acute arsenic poisoning presents as a GI emergency (nausea, vomiting, profuse 'rice water' diarrhoea, garlic odour on breath). Chronic arsenic exposure causes Mees lines (white transverse bands on fingernails), peripheral neuropathy, arsenical keratosis (punctate palmar/plantar thickening), hyperpigmentation, and — critically — is a human carcinogen for lung, bladder, and skin cancers (Bowen's disease, squamous cell carcinoma).
Iron (Fe): Unlike the SH-binding metals, iron toxicity is primarily through free radical generation (Fenton reaction: Fe²⁺ + H₂O₂ → Fe³⁺ + OH• + OH⁻). Hydroxyl radicals cause lipid peroxidation of cell membranes, protein oxidation, and DNA damage. Acute iron ingestion in children causes five recognisable stages: Stage 1 (0–6 h): direct GI mucosal injury — vomiting, haematemesis, diarrhoea; Stage 2 (6–24 h): apparent improvement (systemic iron being taken up by cells — deceptively quiet); Stage 3 (24–48 h): systemic toxicity — metabolic acidosis (from mitochondrial failure + lactic acid from iron disruption of oxidative phosphorylation), shock, hepatotoxicity, coagulopathy; Stage 4 (2–5 days): hepatic necrosis peak; Stage 5 (2–6 weeks): GI strictures from healing of mucosal injury — gastric outlet obstruction.
Copper (Cu) — Wilson's disease: Autosomal recessive deficiency of ATP7B (copper-transporting ATPase in the liver), causing copper accumulation in the liver (hepatitis, cirrhosis), brain (neuropsychiatric features: dysarthria, tremor, personality change), and the cornea (Kayser-Fleischer rings — copper deposits in Descemet's membrane, visible on slit-lamp examination). Diagnosis: low serum ceruloplasmin, elevated 24-hour urinary copper, elevated hepatic copper on biopsy.
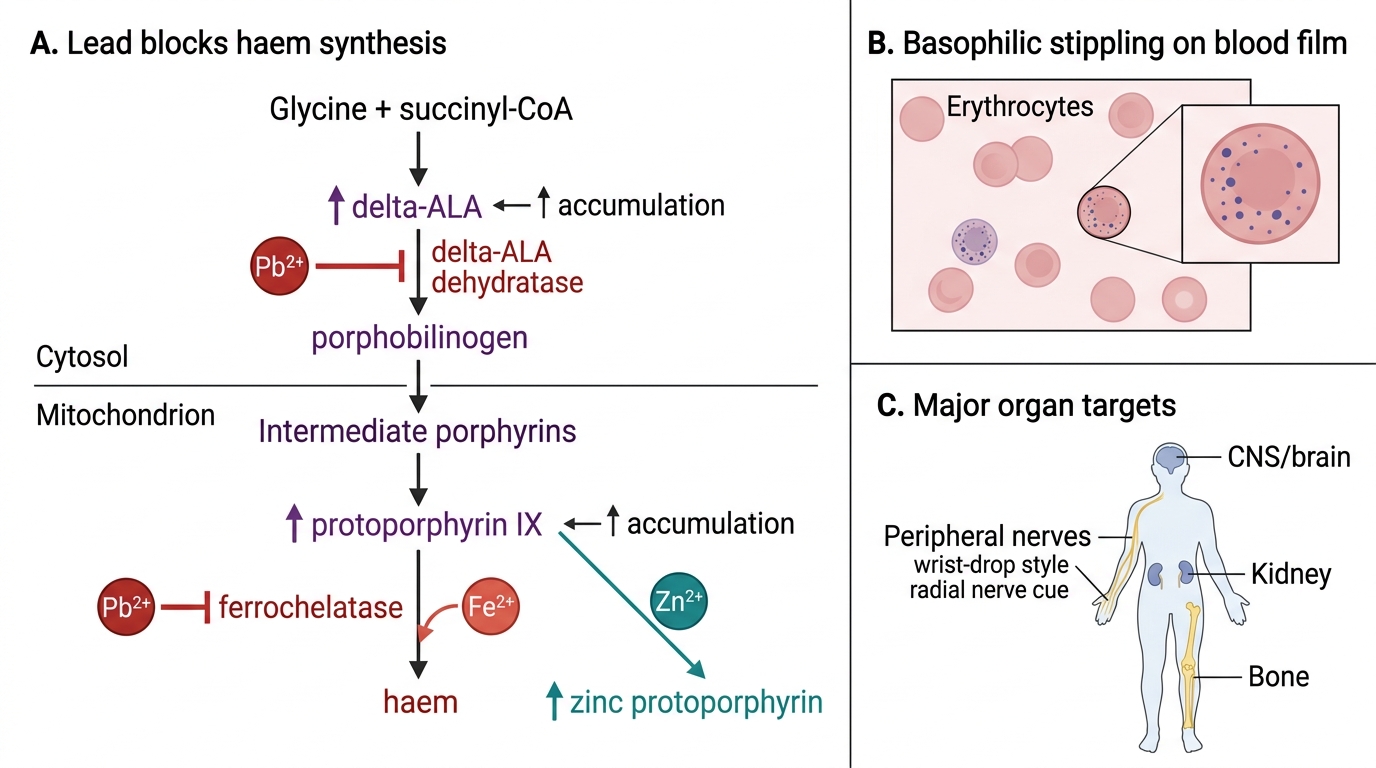
Lead Poisoning: Haem Synthesis Block and Organ Toxicity
Therapeutic Goals of Chelation
The therapeutic goal of chelation therapy is to reduce the body burden of a toxic metal by forming a stable, water-soluble metal-chelator complex that is then excreted — primarily in the urine, and for some chelators also in the bile and faeces — faster than the metal can be mobilised and re-deposited in target organs.
A chelating agent (from the Greek chele, 'claw') is a molecule with two or more electron-donating groups that can coordinate with a metal ion, encircling it and forming a ring-like (chelate) complex. The stability of the chelate complex determines both the efficacy of metal removal and the selectivity of the chelator. The goal is for the chelator to have higher affinity for the toxic metal than the metal has for the body's own SH-containing enzymes, effectively 'out-competing' the enzyme-metal interaction.
Chelation does not 'cure' metal poisoning — it reduces ongoing toxicity and prevents further accumulation, but it cannot restore already-damaged neurons (as in lead encephalopathy or Minamata disease) or reversed fibrosis (as in chronic arsenic or copper liver disease). The goal is to halt progression and allow partial recovery of reversible damage.
The clinical decision to initiate chelation is based on documented metal exposure and either symptomatic poisoning or blood/urine metal levels exceeding treatment thresholds. For lead in children, blood lead level (BLL) >45 mcg/dL requires chelation; BLL >70 mcg/dL with symptomatic encephalopathy requires emergency combined therapy. For iron, a serum iron level >300–500 mcg/dL at 4–6 hours post-ingestion, or presence of systemic toxicity, indicates deferoxamine.
Classification — Heavy Metals and Chelating Agents
The metal-chelator pairing is the single most important piece of pharmacological knowledge in this topic. Each chelator has a specific affinity profile — using the wrong chelator is not just ineffective, it can be harmful.
Chelating agents by class and primary metal targets:
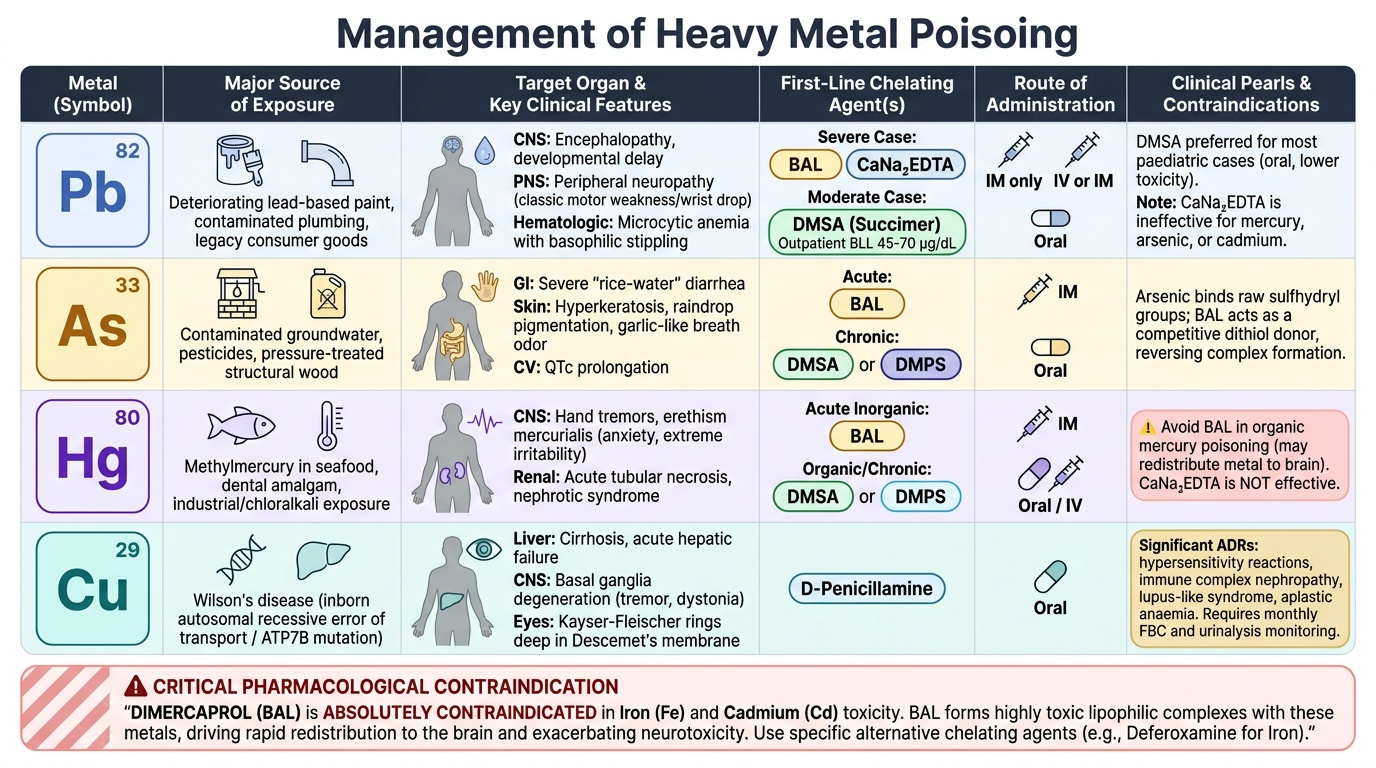
- Dimercaprol (BAL — British Anti-Lewisite): Dithiol (two -SH groups); IM only; originally developed as antidote for arsenic-based chemical warfare agent (lewisite). Metals: arsenic, mercury, lead, gold. ABSOLUTELY CONTRAINDICATED for iron and cadmium — forms toxic metal-BAL complexes that redistribute metal to the brain.
- Calcium disodium EDTA (CaNa₂EDTA): Aminopolycarboxylic acid chelator; IV or IM. Primary use: lead poisoning. Does NOT effectively chelate mercury, arsenic, or cadmium. Often combined with BAL in severe lead poisoning (synergistic).
- DMSA (dimercaptosuccinic acid/succimer): Oral dithiol chelator; used for lead, mercury, arsenic. Preferred over BAL for most paediatric lead poisoning cases because it is oral, less toxic, and can be given outpatient for BLL 45–70 mcg/dL.
- DMPS (sodium 2,3-dimercapto-1-propanesulfonate): Related to DMSA; oral or IV; used for mercury, arsenic, lead.
- D-penicillamine: Oral thiol chelator derived from penicillin; used for Wilson's disease (copper), lead, mercury, and cystinuria. Significant ADR profile: hypersensitivity reactions, immune complex nephropathy, lupus-like syndrome, aplastic anaemia, myasthenia gravis-like syndrome — requires monthly monitoring of FBC and urinalysis.
- Deferoxamine (desferrioxamine, DFO): Hydroxamate chelator; highly selective for iron (and aluminium in dialysis patients). IM or slow IV infusion. Forms the pink/red complex ferrioxamine excreted in urine — 'vin rosé' urine (a useful clinical sign confirming iron chelation). NEVER used for lead, mercury, or arsenic — no efficacy and potentially harmful.
- Trientine: Copper-specific chelator; used as second-line for Wilson's disease when D-penicillamine is not tolerated.
Provided image
SELF-CHECK
A 2-year-old child accidentally ingests 20 adult iron supplement tablets. Which chelating agent is indicated, and which chelating agent is CONTRAINDICATED in this situation?
A. Indicated: dimercaprol (BAL); contraindicated: deferoxamine
B. Indicated: calcium disodium EDTA; contraindicated: DMSA
C. Indicated: deferoxamine; contraindicated: dimercaprol (BAL)
D. Indicated: D-penicillamine; contraindicated: EDTA
Reveal Answer
Answer: C. Indicated: deferoxamine; contraindicated: dimercaprol (BAL)
Deferoxamine is the specific chelating agent for iron poisoning — it forms a stable, water-soluble ferrioxamine complex that is excreted in urine (turning it 'vin rosé' pink). Dimercaprol (BAL) is absolutely contraindicated in iron poisoning because BAL forms a highly toxic iron-BAL complex that can redistribute iron to the brain and other organs, worsening toxicity. BAL is indicated for arsenic, mercury, lead, and gold poisoning, but NOT for iron or cadmium. Deferoxamine has no role in lead, arsenic, or mercury poisoning.