Page 5 of 33
PH9.4 | PH9.4 | Vaccine Pharmacology — SDL Guide — SDL Guide
Learning Objectives
- Describe the basis of active and passive immunisation and the rationale for vaccine scheduling
- Classify vaccines by type (live attenuated, inactivated, subunit, toxoid, conjugate, recombinant vector, mRNA) with examples
- Describe the pharmacokinetics and pharmacodynamics of different vaccine types
- Identify the contraindications to live vaccines and the principles of cold chain management
INSTRUCTIONS
Vaccines represent one of medicine's greatest public health achievements, responsible for eliminating smallpox and nearly eradicating polio. Understanding vaccine pharmacology — how different vaccine types produce immunity, why schedules are designed as they are, and the critical issue of cold chain — is essential for clinical practice, public health, and for understanding the immunosuppressant module you just completed (where live vaccine contraindications are a critical prescribing point).
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 62 (Vaccines and Immunisation) (textbook)
- Goodman & Gilman. The Pharmacological Basis of Therapeutics, 13th ed., Ch. 36 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 1988, global polio caused 350,000 cases annually. By 2023, fewer than 30 wild poliovirus cases were reported worldwide. This elimination was achieved primarily through one pharmacological intervention: the oral polio vaccine (OPV). Yet in 2022, a young adult in New York who was unvaccinated was paralysed by vaccine-derived poliovirus — a direct consequence of incomplete vaccination coverage. Vaccines are simultaneously the most cost-effective pharmacological interventions in history and agents that, when misunderstood or misapplied (wrong type, broken cold chain, contraindicated in immunocompromised patients), can cause harm. Understanding their pharmacology is not academic — it is clinically essential.
WHY THIS MATTERS
Vaccine pharmacology is directly relevant to clinical practice in multiple ways. As a prescribing physician, you will advise patients and caregivers on vaccine schedules, screen patients for contraindications before prescribing immunosuppressants or biologics (live vaccines must be administered before starting), manage cold chain in your clinic or district, and counsel hesitant patients with evidence-based information. Public health officers design vaccination programmes using herd immunity calculations. Understanding vaccine pharmacology enables you to make these decisions correctly and to explain vaccine science to patients in an accessible way.
RECALL
From Year-1 Physiology, recall the basics of adaptive immunity. A primary immune response occurs on first antigen encounter: a latency period of 1–2 weeks while naïve B-cells and T-cells are activated, clonally expand, and differentiate. Antibody titres rise slowly — initially IgM, then class-switching to IgG. After the threat clears, memory B-cells and memory T-cells persist. On second exposure (or vaccination boost), memory cells enable a rapid, high-titre IgG response within 2–3 days — this is the secondary (anamnestic) response and is the immunological basis of booster doses. Also recall: T-independent antigens (pure polysaccharides) activate B-cells without T-cell help and produce IgM without long-term memory — this is why plain polysaccharide vaccines are ineffective in infants under 2 years. T-dependent antigens (proteins and protein-conjugated polysaccharides) activate T-helper cells, produce class-switched IgG, and generate memory — the rationale for conjugate vaccines.
The Problem Vaccines Solve: Herd Immunity and Vaccine-Preventable Disease
Vaccine-preventable diseases collectively cause millions of deaths annually in unimmunised populations. Measles remains the leading cause of vaccine-preventable death in children globally, with >95% of cases occurring in low-coverage settings. Pertussis (whooping cough), Haemophilus influenzae type b (Hib) meningitis, tetanus, hepatitis B, and polio each account for substantial morbidity and mortality that disappears with high vaccination coverage.
The concept of herd immunity explains why vaccination of individuals protects the whole community. When a sufficient proportion of a population is immune (whether from prior infection or vaccination), transmission chains are broken and susceptible individuals who cannot be vaccinated (immunocompromised patients, neonates, those with contraindications) are protected by the surrounding immune majority. The herd immunity threshold — the proportion that must be immune to prevent sustained transmission — is directly determined by the pathogen's basic reproduction number (R₀). For measles (R₀ ≈ 12–18), the threshold is approximately 92–95%, meaning coverage below this level permits measles outbreaks even when most children are vaccinated. For polio (R₀ ≈ 5–7), the threshold is approximately 80–85%.
Active immunity induced by vaccines is distinct from passive immunity (transfer of preformed antibodies, e.g. immunoglobulin products, anti-tetanus serum, or maternal antibodies). Active immunity requires time to develop (weeks) but is long-lasting (years to lifetime) and self-reinforcing with boosters. Passive immunity is immediate but temporary (weeks to months), because transferred antibodies are catabolised. Vaccines produce active immunity; immunoglobulin preparations are passive.
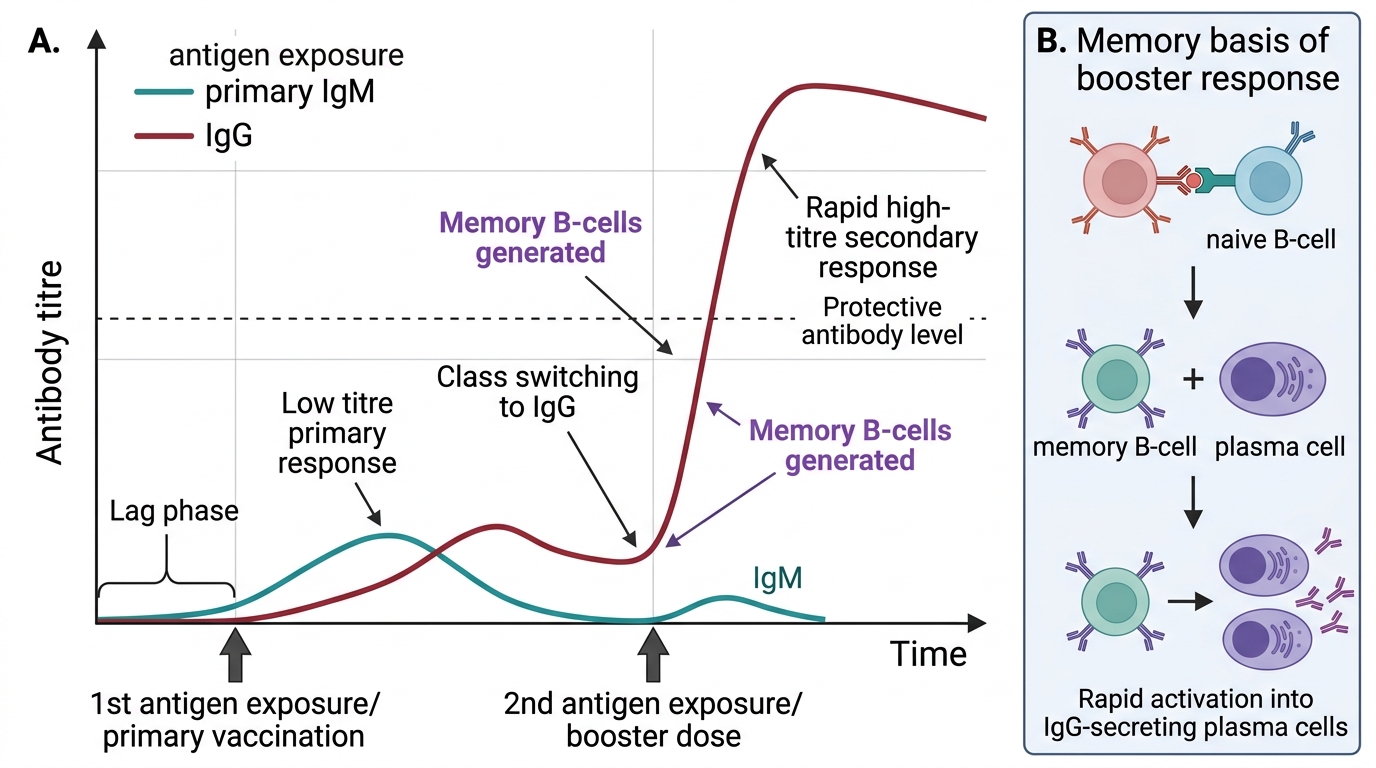
Primary and Secondary Immune Response After Vaccination
The Goals of Vaccination
The primary pharmacological goal of vaccination is to prime the immune system with a safe version of the antigen, generating immunological memory without causing disease. This is achieved by presenting the immune system with an antigenic stimulus — whether a live attenuated organism, killed pathogen, purified protein subunit, inactivated toxin, or antigen-encoding nucleic acid — in a form that is immunogenic but not pathogenic.
Primary vaccination produces a modest but real level of protection and, crucially, establishes a population of memory B-cells and memory T-cells. Booster doses take advantage of the secondary immune response — the accelerated, high-magnitude IgG production that occurs when memory cells are re-exposed to antigen. This is why tetanus vaccination requires a primary 3-dose series to establish memory, followed by boosters every 10 years to maintain protective antibody levels.
The vaccine schedule is designed to balance several immunological realities: (1) maternal antibodies — passively transferred from the mother — are present in neonates and can neutralise vaccine antigens if vaccination begins too early; (2) the neonatal immune system is relatively immature; (3) T-independent antigens (pure polysaccharides) are ineffective until about 2 years of age when T-independent immune competence matures. The National Immunisation Programme (NIP/UIP) schedule in India uses combinations of live and inactivated vaccines, timed to optimise protection while avoiding interference from maternal antibodies.
Adjuvants are added to many non-live vaccines to enhance immunogenicity by activating the innate immune system (acting as a 'danger signal') and promoting more robust antigen presentation. Common adjuvants: aluminium hydroxide (alum) — the most widely used; AS04 (alum + TLR4 agonist MPL) used in HPV vaccine; MF59 squalene emulsion in some influenza vaccines. Adjuvants do NOT contain pathogen antigens and are not vaccines themselves.
Classification of Vaccines
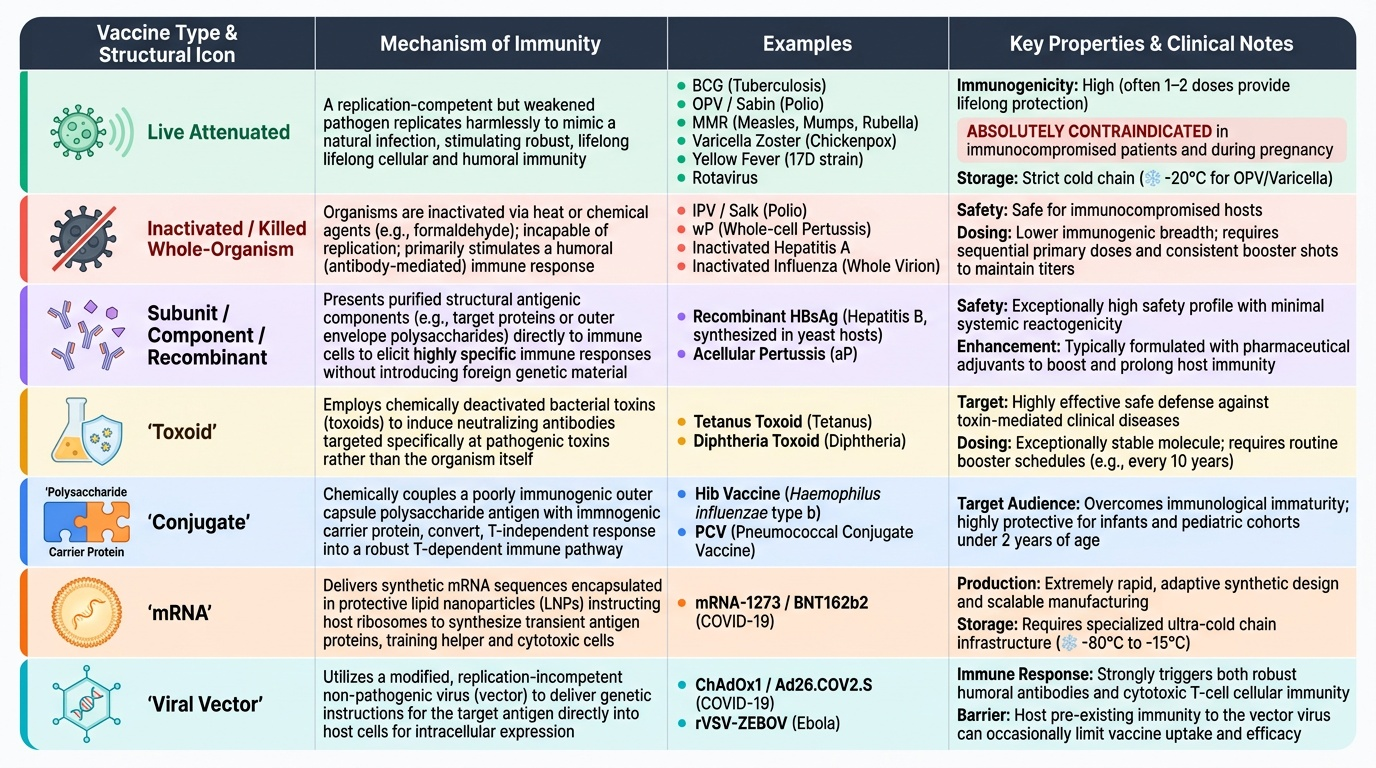
Vaccines are classified by the nature of their antigenic component and production method. Each type has distinct immunological properties, advantages, disadvantages, and contraindications. Understanding the classification is essential for prescribing, storage, and schedule decisions.
1. Live attenuated vaccines contain living organisms (bacteria or viruses) that have been weakened through serial passage in culture to abolish pathogenicity while retaining immunogenicity. They closely mimic natural infection and produce the strongest, most long-lasting immunity — often after just 1–2 doses. Examples: BCG (tuberculosis), OPV (oral polio, Sabin), MMR (measles-mumps-rubella — all three components are live attenuated), varicella zoster vaccine, yellow fever (17D strain), rotavirus vaccines. Key property: absolutely contraindicated in immunocompromised patients (can cause disseminated disease); generally contraindicated in pregnancy; require strict cold chain (often -20°C for OPV, varicella).
2. Inactivated/killed whole-organism vaccines contain pathogens killed by heat or chemical treatment (formaldehyde, beta-propiolactone). They cannot replicate and cannot cause disease. They produce less robust immunity than live vaccines and typically require multiple doses + boosters. Examples: IPV (inactivated polio vaccine, Salk), whole-cell pertussis (wP), inactivated hepatitis A vaccine, inactivated influenza (whole virion). Key property: safe in immunocompromised patients.
3. Subunit/component vaccines contain purified antigenic components — proteins or polysaccharides — without the whole organism. Examples: hepatitis B vaccine (recombinant HBsAg produced in yeast — NOT a live or killed whole virus), acellular pertussis (aP, purified pertussis toxoid + fimbriae), influenza subunit, typhoid Vi polysaccharide (Vi). Key property: high safety; less immunogenic than live vaccines; require adjuvants and boosters.
4. Toxoid vaccines use inactivated bacterial exotoxins (toxins chemically or heat-detoxified). The immune response targets the toxin, not the organism. Examples: tetanus toxoid (TT), diphtheria toxoid (DT). Key property: highly effective; safe; require booster every 10 years for tetanus.
5. Conjugate vaccines link a polysaccharide antigen (normally T-independent, ineffective in infants) to a carrier protein (CRM197, tetanus toxoid, diphtheria toxoid), converting it to a T-dependent antigen that generates immunological memory even in infants under 2 years. Examples: Haemophilus influenzae type b (Hib) — PRP conjugated to carrier; meningococcal conjugate (MenACWY); pneumococcal conjugate vaccine (PCV13). Key property: enables infant immunisation against encapsulated bacteria.
6. Recombinant viral vector vaccines use a live (but non-replicating) viral vector — typically a modified adenovirus — to deliver the gene encoding the target antigen. The host's cells synthesise the antigen and present it to the immune system. Examples: ChAdOx1 (AstraZeneca COVID-19 vaccine — non-replicating chimpanzee adenovirus expressing spike protein), rVSV-ZEBOV (Ebola vaccine — vesicular stomatitis virus vector). Key property: strong cellular and humoral immunity; complex manufacturing.
7. mRNA vaccines encapsulate antigen-encoding mRNA in lipid nanoparticles for cell entry. Host ribosomes translate the mRNA into the antigen protein, which is expressed on the cell surface and presented to the immune system. Examples: BNT162b2 (Pfizer-BioNTech COVID-19), mRNA-1273 (Moderna COVID-19). Key property: rapid development; no live organism; intrinsically activates innate immunity; mRNA is transient (does not integrate into the genome); require ultra-cold storage (-20°C to -70°C).
Provided image
SELF-CHECK
A 2-year-old child received only the plain polysaccharide typhoid vaccine (Vi) but showed poor immune response. Which immunological principle explains why conjugate vaccines are preferable in infants?
A. Infants lack B-cells and cannot respond to any antigens
B. Plain polysaccharides are T-independent antigens — they activate B-cells without T-cell help, producing little class-switched IgG and no immunological memory in infants under 2 years
C. Plain polysaccharide vaccines cannot be administered intramuscularly in infants
D. Polysaccharide vaccines cause more severe adverse effects in young children
Reveal Answer
Answer: B. Plain polysaccharides are T-independent antigens — they activate B-cells without T-cell help, producing little class-switched IgG and no immunological memory in infants under 2 years
Pure polysaccharides are T-independent antigens — they activate B-cells directly without T-helper cell involvement, producing mainly IgM without class-switching to IgG and without generating immunological memory. In infants under 2 years, T-independent immune competence is immature. Conjugate vaccines solve this by linking the polysaccharide to a carrier protein, converting the antigen to T-dependent, enabling T-helper cell activation, class switching, and memory B-cell generation. This is why Hib conjugate vaccine is used in the infant schedule while plain Hib polysaccharide vaccine fails to protect infants.