Page 10 of 34
PH3.4 | PH3.4 | Opioid Analgesics and Safe Use Instructions — SDL Guide — SDL Guide
Learning Objectives
- Classify opioid analgesics by receptor activity (full agonist, partial agonist, mixed agonist-antagonist, antagonist) and identify key agents in each class
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of major opioid analgesics
- Identify dangerous drug interactions and contraindications for specific opioids (pethidine + MAOI; tramadol + SSRI; pethidine in renal failure)
- Explain the pharmacological basis of opioid overdose recognition and management with naloxone
INSTRUCTIONS
Opioids are among the most powerful analgesics available and are essential for managing severe acute pain, cancer pain, and palliative care. They are also among the most misused drugs worldwide. Rational opioid prescribing — choosing the right agent, dose, and monitoring plan — requires understanding receptor pharmacology, dangerous drug interactions, and the recognition and reversal of overdose. This module builds that framework.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 32 (Opioid Analgesics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 18 (Opioids) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old man with chronic renal failure and moderate post-operative pain is prescribed pethidine for analgesia. Over the next 24 hours he develops tremors, myoclonus, and eventually a generalised seizure. The ward team is baffled — it was 'just a painkiller'. The culprit: norpethidine, the active metabolite of pethidine, accumulated in renal failure and reached neurotoxic levels. This is one of several life-threatening opioid-specific interactions and contraindications — the reason that special instructions for safe opioid use exist and matter.
WHY THIS MATTERS
You will prescribe opioids. You will encounter overdoses. You will be asked to write a prescription for post-operative pain, cancer pain, or chronic pain, and you must know which opioid to choose, which to avoid in which patient, and how to recognise and reverse an overdose with naloxone. The pharmacological distinctions among opioids — receptor activity, metabolite toxicity, duration, interactions — are not fine print; they are the safety margin between adequate analgesia and iatrogenic catastrophe.
RECALL
Recall from Year-1 physiology: nociception involves peripheral nociceptors (Aδ and C fibres), spinal cord dorsal horn (substantia gelatinosa), ascending spinothalamic tract, and supraspinal pain centres (thalamus, cortex, limbic system). The descending inhibitory pathway (from periaqueductal grey → raphe nuclei → dorsal horn) modulates pain via serotonin and noradrenaline. The endogenous opioid system consists of three families of peptides — enkephalins (δ-receptor), endorphins (μ-receptor), and dynorphins (κ-receptor) — released during pain and stress. Recall that G-proteins couple receptors to intracellular signalling — the Gi protein inhibits adenylyl cyclase (reducing cAMP), which will be central to understanding opioid mechanism.
Pathophysiology of Pain — Opioid Receptor Biology
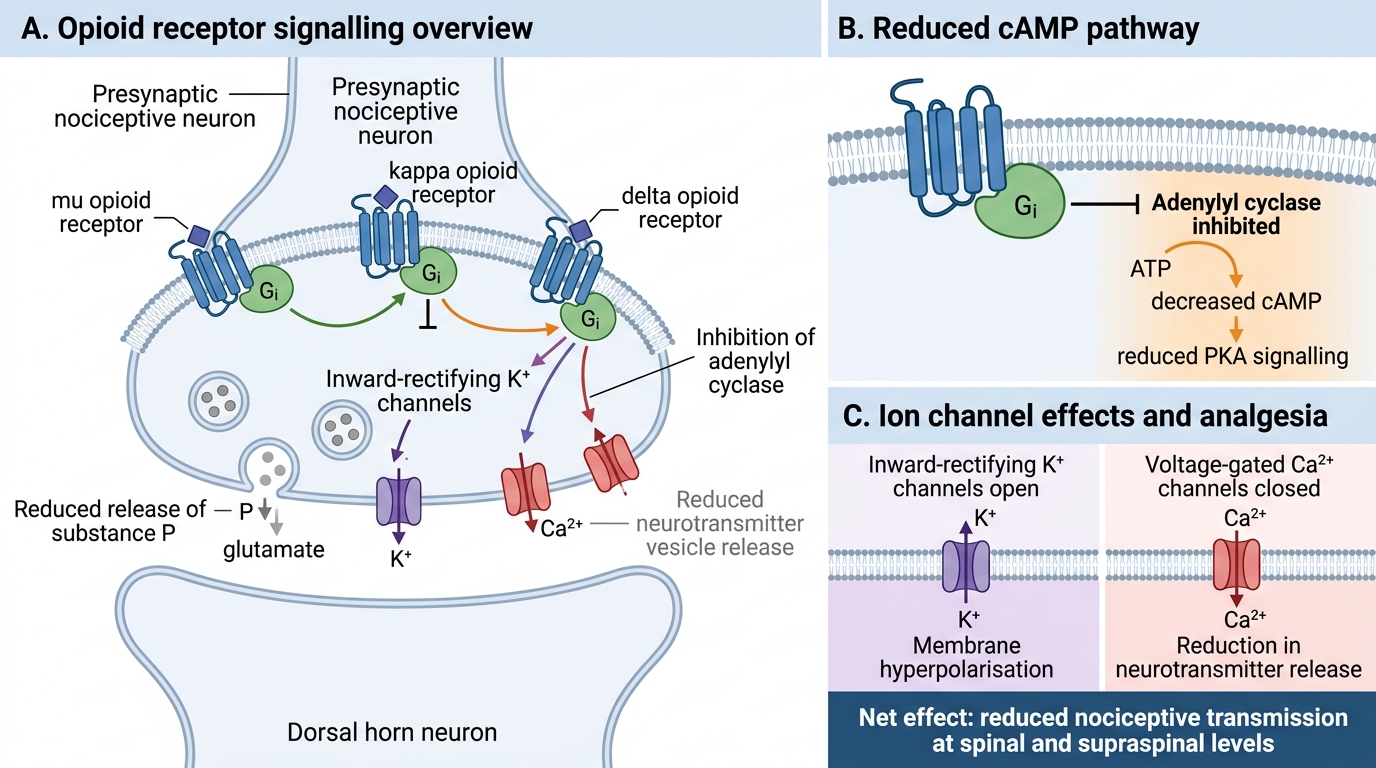
Pain transmission depends on the balance between excitatory nociceptive input and endogenous inhibitory controls. Opioid receptors (μ, κ, δ — all GPCRs coupled to Gi protein) are expressed at three strategic levels: peripheral nociceptors (peripheral analgesia), spinal cord dorsal horn (spinal analgesia — pre-synaptic inhibition of neurotransmitter release; post-synaptic hyperpolarisation), and supraspinal centres including the periaqueductal grey, limbic system, and brainstem (supraspinal analgesia and emotional modulation of pain).
All three receptor types couple to Gi protein, producing three convergent intracellular effects:
1. Inhibition of adenylyl cyclase → reduced intracellular cAMP → reduced protein kinase A activity → reduced neuronal excitability
2. Opening of inward-rectifying K⁺ channels → K⁺ efflux → hyperpolarisation → reduced action potential firing
3. Closure of voltage-gated Ca²⁺ channels (pre-synaptic) → reduced Ca²⁺ influx → reduced neurotransmitter (substance P, glutamate) release
The μ receptor mediates the principal analgesic, euphoric, respiratory depressant, and constipating effects of opioids. The κ receptor contributes to spinal analgesia, sedation, and dysphoria (κ agonism produces dysphoria/psychotomimesis — explains why pentazocine causes hallucinations). The δ receptor contributes to spinal analgesia and mood regulation.
Opioid Receptor Signalling and Analgesia
Goals of Opioid Analgesic Therapy
The therapeutic goal of opioid analgesia is to achieve adequate pain control — enabling function, sleep, and quality of life — using the minimum effective dose for the minimum necessary duration, while monitoring for adverse effects, dependence, and misuse. These goals are operationalised by the WHO analgesic ladder (originally for cancer pain, now widely applied):
Step 1 (mild pain): Non-opioid analgesics — paracetamol, NSAIDs ± adjuvants (antidepressants, anticonvulsants for neuropathic pain).
Step 2 (moderate pain): Weak opioids (codeine, tramadol) ± non-opioids.
Step 3 (severe pain): Strong opioids (morphine, fentanyl, oxycodone) ± non-opioids ± adjuvants.
Key principles of rational opioid prescribing:
- By mouth (oral route preferred where possible), by the clock (regular dosing — not PRN for constant pain), by the ladder (titrate upward only when the current step fails), for the individual (dose is titrated to effect), with attention to detail (specify drug, dose, route, frequency, breakthrough dose).
- Opioids are appropriate for acute severe pain (post-operative, trauma), cancer pain, and palliative care. Chronic non-cancer pain: use is more contested — consider opioid rotation, dependence risk assessment.
- Avoid opioids entirely when: respiratory depression is already present, the patient is acutely intoxicated with CNS depressants, raised ICP without airway protection, or in specific drug interactions described below.
Classification of Opioid Analgesics
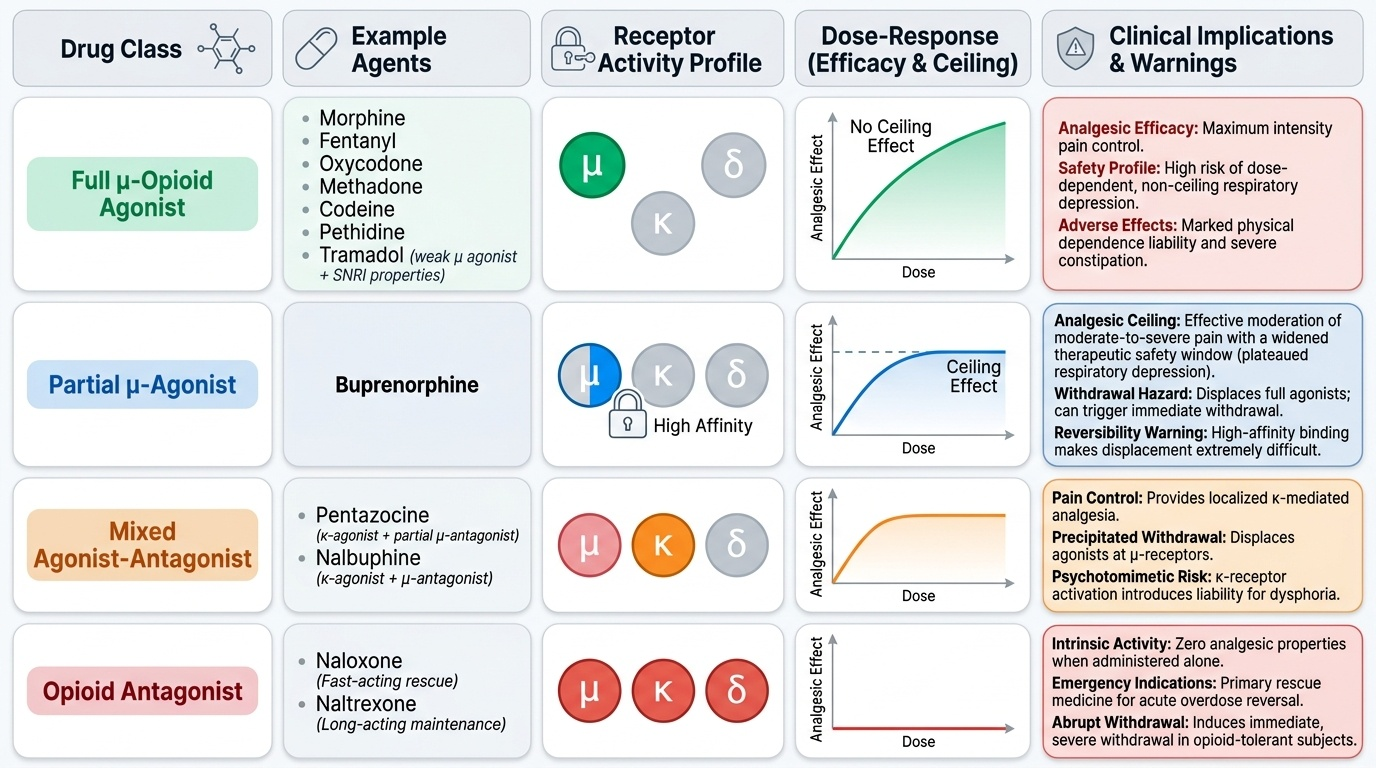
Opioid analgesics are classified by their receptor activity at μ, κ, and δ receptors, which determines their maximum analgesic efficacy, ceiling on respiratory depression, and their ability to precipitate withdrawal in opioid-dependent patients.
Full μ-opioid agonists: morphine, codeine, fentanyl, pethidine/meperidine, methadone, oxycodone, tramadol (though tramadol has weak μ activity plus SNRI properties). These produce full activation of μ receptors — maximum analgesic efficacy but also maximum respiratory depression, constipation, and dependence potential. No ceiling effect on respiratory depression.
Partial μ-agonist: buprenorphine — activates μ receptors but to a sub-maximal level (partial agonism). Consequences: (a) ceiling effect on respiratory depression (safer in overdose than full agonists), (b) analgesic ceiling (adequate for moderate pain, but at high doses further dose increases add no analgesic benefit), (c) very high receptor affinity — displaces full agonists from μ receptors, meaning it can precipitate withdrawal if given to a fully opioid-dependent patient, and naloxone has difficulty reversing it at standard doses.
Mixed agonist-antagonists: pentazocine (κ agonist + partial μ antagonist), nalbuphine (κ agonist + μ antagonist). These have analgesic activity (κ-mediated) but can precipitate withdrawal in opioid-dependent patients (by antagonising μ receptors). Pentazocine causes dysphoria and psychotomimetic effects (κ agonism).
Pure antagonists: naloxone (short t½, IV/IM/IN — acute overdose reversal); naltrexone (long t½, oral — maintenance of opioid/alcohol abstinence).
Provided image