Page 16 of 34
PH3.6 | PH3.6 | Anxiolytics and Goals of Anxiety Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Classify anxiolytic agents by mechanism and identify their role in short-term vs long-term anxiety management
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of benzodiazepines, buspirone, and SSRIs as anxiolytics
- Explain the general goals of pharmacotherapy for anxiety disorders, including why benzodiazepines are not appropriate as long-term monotherapy
- Select the appropriate anxiolytic for specific anxiety disorders (GAD, panic disorder, social anxiety, performance anxiety)
INSTRUCTIONS
Anxiety disorders are the most prevalent mental health conditions worldwide. While benzodiazepines provide rapid symptom relief, their long-term use carries serious risks of dependence and cognitive impairment. This module explains why the pharmacological goals of anxiety treatment favour SSRIs and buspirone over long-term BZD use — and how to match drug to disorder.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 30 (Antidepressants) and Ch 27 (Sedative-Hypnotics — Anxiolytic use) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 17 (Drug Therapy of Depression and Anxiety Disorders) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old software engineer presents to your clinic with a 6-month history of excessive worry about his job, family, and health, persistent muscle tension, sleep difficulty, and an inability to relax. He has been managing with alprazolam (a short-acting BZD) prescribed by a colleague, taking it 3-4 times daily. He says it 'helps in the moment' but he cannot function without it now, and feels more anxious between doses. He has generalised anxiety disorder — and he is on exactly the wrong long-term pharmacological strategy. Understanding why requires knowing the pharmacological goals of anxiety treatment and how drug mechanisms map to them.
WHY THIS MATTERS
Anxiety disorders affect roughly 1 in 5 adults at some point in their lives. As a prescriber you will be confronted with patients requesting or already using benzodiazepines for anxiety. You must be able to explain why BZDs are appropriate only for short-term (≤4 weeks) symptomatic relief, why buspirone and SSRIs are the pharmacologically defensible long-term choices, and how the pharmacology of each agent determines its role. Prescribing BZDs indefinitely for anxiety is a common clinical error with real patient harm — dependence, cognitive decline, falls, and discontinuation seizures.
RECALL
Recall from your study of sedative-hypnotics (PH3.2): benzodiazepines potentiate GABA-A by increasing the frequency of Cl⁻ channel opening; they require GABA to be present (ceiling effect). Physical dependence develops with regular use beyond 4 weeks. Recall from PH3.5: SSRIs block the serotonin transporter (SERT), increasing synaptic 5-HT; onset of clinical effect is delayed by 2-4 weeks due to downstream neuroplastic changes. Recall from Year-1 physiology: the amygdala is the brain's fear-processing centre, driving the 'fight-or-flight' response via the HPA axis and sympathetic nervous system. Dysregulated amygdala activity underlies most anxiety disorders.
Pathophysiology of Anxiety Disorders — Neurobiology
Anxiety disorders arise from dysregulation of the fear circuit — a network centred on the amygdala and its connections with the prefrontal cortex (cognitive modulation of fear), hippocampus (contextual fear memory), hypothalamus (HPA axis activation), and brainstem autonomic centres (sympathetic arousal). In pathological anxiety, this circuit is hyperactivated for threats that are disproportionate or absent — resulting in excessive worry, autonomic arousal, and avoidance behaviour.
Three neurobiological mechanisms are pharmacologically relevant:
1. Deficient GABAergic inhibition: the amygdala and cortex receive dense GABAergic innervation that normally dampens fear circuit activity. Reduced GABA-A receptor function (due to stress, genetics, or chronic benzodiazepine use and subsequent receptor down-regulation) allows hyperactivation. Benzodiazepines exploit this by potentiating residual GABA-A activity — this explains their rapid efficacy and why chronic use leads to receptor down-regulation (tolerance).
2. Dysregulated 5-HT₁A signalling: serotonin has a complex role in anxiety; the 5-HT₁A receptor is a Gi-coupled autoreceptor (on dorsal raphe serotonin neurons) and postsynaptic receptor (in amygdala, hippocampus). Its partial agonism by buspirone and its increased activation by SSRIs (via increased 5-HT availability) produce anxiolytic effects through slow neuroplastic remodelling of the fear circuit.
3. Hyperactive HPA axis and noradrenergic arousal: chronic stress increases cortisol and activates locus coeruleus noradrenergic neurons — contributing to generalised arousal, insomnia, and the somatic symptoms of anxiety (palpitations, tremor, sweating).
IMPORTANT understanding for prescribing: GABAergic strategies (BZDs) provide rapid but non-curative symptom relief; serotonergic strategies (SSRIs, buspirone) address the circuit-level dysregulation with delayed but more durable benefit.
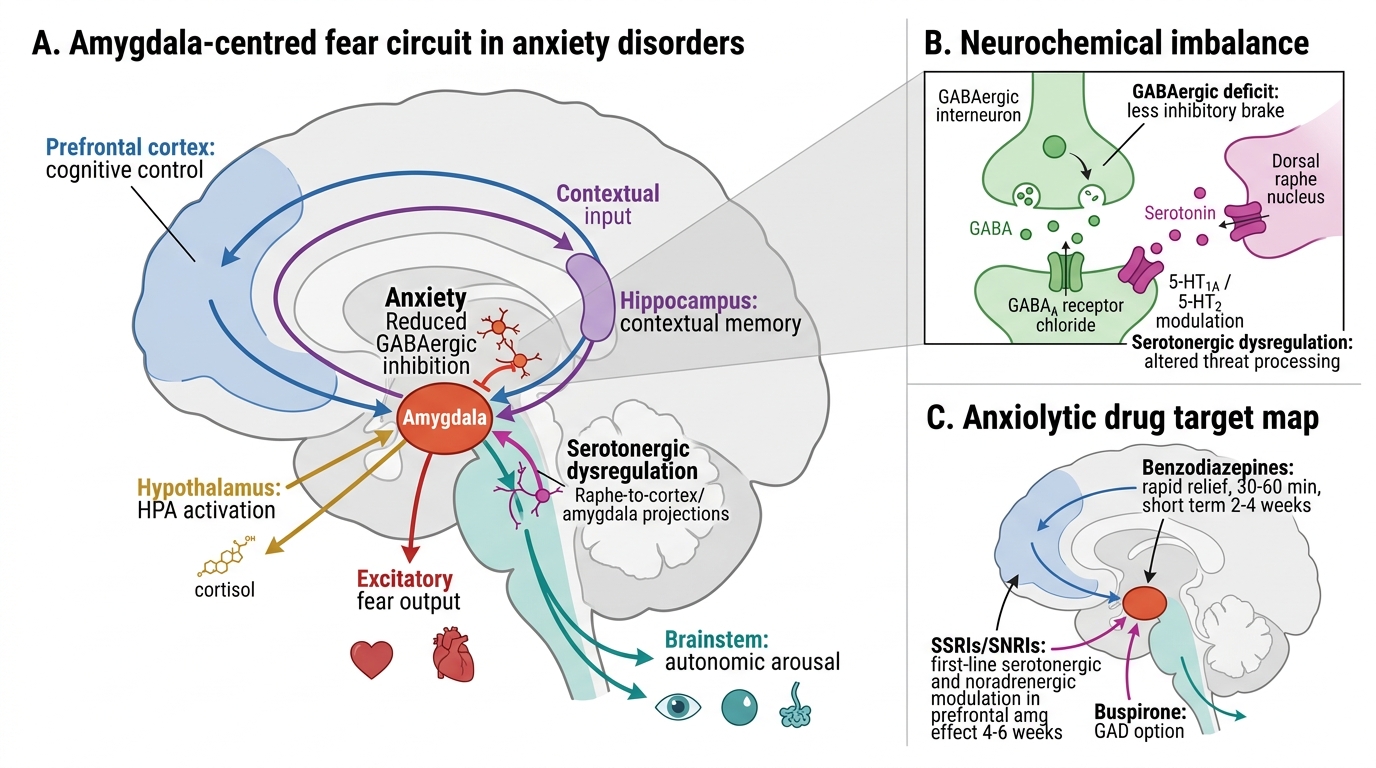
Fear Circuit and Anxiolytic Drug Targets
Goals of Anxiety Pharmacotherapy
The pharmacological goals of anxiety treatment must be matched to the time horizon and disorder type:
Short-term goals (acute anxiety, procedural anxiety, or adjunct at onset): rapid reduction of distressing symptoms — palpitations, tremor, insomnia, somatic arousal. For this purpose, benzodiazepines are rapidly effective (onset within 30-60 minutes). They are appropriate for: pre-procedural anxiety, acute severe anxiety episodes, initiation of SSRI therapy (where SSRI-emergent anxiety during the first 1-2 weeks can be managed with a short BZD course), and alcohol withdrawal. Duration: maximum 2-4 weeks (dependence risk beyond this).
Long-term goals (chronic anxiety disorders — GAD, panic disorder, PTSD, OCD, social anxiety): sustained reduction of anxiety severity, prevention of relapse, and restoration of daily function. For this purpose, SSRIs/SNRIs are the pharmacological first-line (supported by multiple RCTs). They require 4-6 weeks for full anxiolytic effect and should be continued for ≥12 months after remission. Buspirone is an evidence-based alternative for generalised anxiety disorder (GAD) specifically — with no dependence liability and no sedation. Non-pharmacological treatment (cognitive-behavioural therapy, CBT-I) is additive and preferred over long-term pharmacotherapy alone.
Pharmacological principles guiding selection:
- Rapid onset needed → BZD (≤4 weeks)
- Chronic disorder → SSRI/SNRI first-line
- GAD without need for sedation, dependence concern → buspirone
- Somatic performance anxiety (exams, public speaking) → propranolol PRN
- Avoid long-term BZD monotherapy for any chronic anxiety disorder
Classification of Anxiolytic Agents
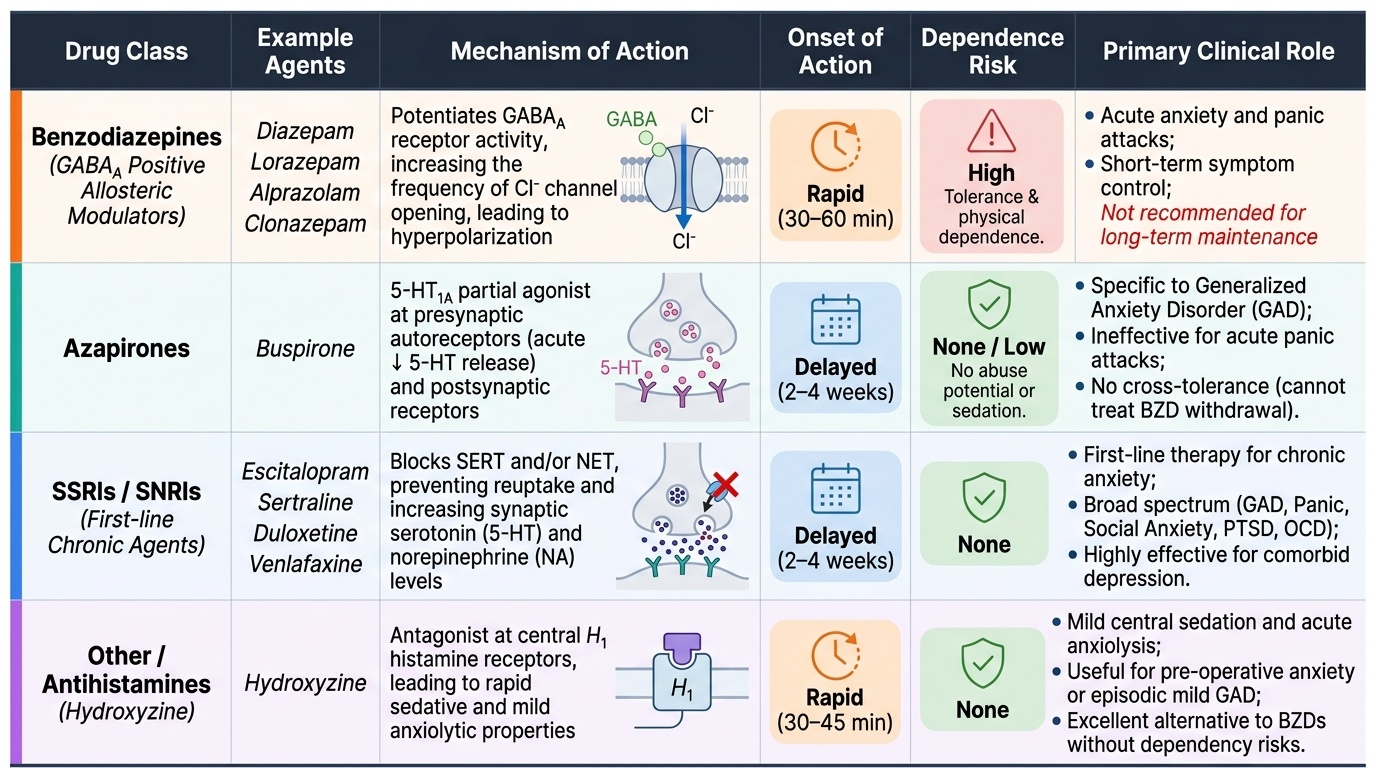
Anxiolytic agents are classified by their pharmacological mechanism, which determines their onset of action, adverse effect profile, dependence liability, and the anxiety disorders they are suitable for.
1. Benzodiazepines (GABA-A positive allosteric modulators): diazepam, lorazepam, alprazolam, clonazepam — potentiate GABA-A by increasing frequency of Cl⁻ channel opening. Rapid onset (30-60 min oral). High efficacy for acute anxiety and panic attacks. Risk of dependence with prolonged use; tolerance to anxiolytic effect develops over weeks.
2. Azapirones — buspirone: 5-HT₁A partial agonist at presynaptic autoreceptors (reduces serotonin release acutely) and postsynaptic receptors (longer-term receptor desensitisation and neuroplastic change). Anxiolytic onset: 2-4 weeks (delayed, like SSRIs). No sedation, no motor impairment, no dependence or abuse potential, no cross-tolerance with BZDs (will not relieve BZD withdrawal). Effective specifically for GAD; NOT for panic disorder or acute anxiety episodes.
3. SSRIs/SNRIs: first-line for all chronic anxiety disorders. Mechanism: SERT blockade (+ NET for SNRIs) → increased synaptic 5-HT (+ NA). Onset: 2-4 weeks. No dependence. The same drugs used for depression are used for anxiety — evidence-based for GAD, panic disorder, social anxiety, PTSD, and OCD.
4. Other agents: (a) Hydroxyzine (H₁ antihistamine) — mild central sedation and anxiolysis; no dependence; useful for pre-operative anxiety or mild GAD; (b) Propranolol (beta-blocker) — blocks peripheral sympathomimetic manifestations of anxiety (tremor, tachycardia, palpitations) — used for performance anxiety (exams, public speaking) — NO central anxiolytic effect; does not reduce worry or fear; (c) Pregabalin — α₂δ-subunit Ca²⁺ channel modulator; evidence for GAD and social anxiety; some dependence potential.
Provided image