Page 19 of 34
PH3.7 | PH3.7 | Antiparkinsonian and Neurodegenerative Disorder Drugs — SDL Guide — SDL Guide
Learning Objectives
- Explain the pathophysiology of Parkinson's disease and the pharmacological rationale for dopaminergic and anticholinergic treatments
- Describe the pharmacokinetics, pharmacodynamics, uses, and adverse drug reactions of levodopa/carbidopa, dopamine agonists, MAO-B inhibitors, and anticholinergics
- Write a prescription to manage a case of drug-induced parkinsonism, including the rationale for choosing anticholinergics over levodopa
- Identify the pharmacological management of common neurodegenerative disorders (Alzheimer's dementia)
INSTRUCTIONS
Parkinson's disease affects approximately 1% of people over 60, and drug-induced parkinsonism (from antipsychotics and antiemetics) is encountered at any age. The pharmacological management of parkinsonism requires understanding the dopamine-acetylcholine imbalance model — and critically, recognising that the treatment of drug-induced parkinsonism (anticholinergics) differs fundamentally from idiopathic PD management (dopaminergic agents).
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 33 (Drugs for Parkinsonism and Alzheimer's Disease) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 22 (Treatment of Central Nervous System Degenerative Disorders) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman is admitted to the psychiatric ward with acute psychosis and started on haloperidol. Two days later the nursing staff report that she cannot stop shaking — she has a coarse resting tremor in both hands, walks with a shuffling gait, and her face is expressionless. Her relatives are concerned she has developed Parkinson's disease. The psychiatrist correctly identifies this as drug-induced parkinsonism (DIP) — haloperidol's D2-blockade in the nigrostriatal pathway has mimicked the dopamine deficiency of Parkinson's disease. He writes a prescription for trihexyphenidyl (an anticholinergic), not levodopa. Understanding why this is the correct choice — and not levodopa — requires understanding the pharmacology of the dopamine-acetylcholine balance in the striatum.
WHY THIS MATTERS
You will encounter patients with Parkinson's disease in neurology, geriatrics, and general practice. You will also see drug-induced parkinsonism (from antipsychotics and metoclopramide) in psychiatry and emergency settings. The competency explicitly requires you to write a prescription for drug-induced parkinsonism — this is an OSCE skill and a day-to-day clinical need. Understanding why levodopa should NOT be used in DIP (it does not address D2 receptor blockade by the offending drug, and if the cause is an antipsychotic, increasing dopaminergic tone would worsen psychosis) prevents a clinical error.
RECALL
Recall from Year-1 neuroscience: the nigrostriatal pathway runs from the substantia nigra pars compacta (SNpc) to the striatum (caudate + putamen). Dopamine release from SNpc neurons inhibits the indirect pathway (via D2 receptors) and activates the direct pathway (via D1 receptors) — net effect: facilitation of voluntary movement and suppression of competing motor programmes. Recall that the striatum also receives cholinergic input from local interneurons. The balance between dopaminergic (inhibitory) and cholinergic (excitatory) tone in the striatum is essential for smooth motor control. Loss of dopaminergic neurons (as in PD) tips this balance towards cholinergic excess — producing the characteristic triad of tremor, rigidity, and bradykinesia.
Pathophysiology of Parkinson's Disease — Dopamine-Acetylcholine Imbalance
Parkinson's disease (PD) is a progressive neurodegenerative disorder characterised by the selective loss of dopaminergic neurons in the substantia nigra pars compacta (SNpc). The pathological hallmark is the accumulation of Lewy bodies (intraneuronal aggregates of α-synuclein protein). Symptoms appear when approximately 70-80% of nigrostriatal dopaminergic neurons are lost — the remaining neurons compensate until this threshold is crossed, explaining the asymptomatic preclinical phase.
The cardinal motor features of PD — the triad of tremor (resting), rigidity, and bradykinesia (slowed movements), with postural instability as a fourth feature — arise directly from the dopamine-acetylcholine imbalance in the striatum:
- Normal state: dopamine (inhibitory, via D2 on indirect pathway neurons; excitatory via D1 on direct pathway neurons) and acetylcholine (from striatal interneurons, excitatory) are in dynamic balance — smooth motor control results.
- PD state: dopamine deficiency → loss of D2-mediated inhibition of the indirect pathway → overactivity of the indirect pathway (→ reduced thalamic output to cortex) AND loss of D1-mediated facilitation of the direct pathway → net reduction in thalamo-cortical activation of motor cortex. Result: slowed, rigid movements with resting tremor (the tremor is partly generated by an oscillating basal ganglia-thalamo-cortical loop).
- Relative cholinergic excess: the loss of dopamine removes its inhibitory counterbalance to striatal cholinergic interneurons — muscarinic receptor stimulation in the striatum increases, contributing especially to tremor and rigidity.
This model predicts two pharmacological strategies: increase dopaminergic tone (levodopa, dopamine agonists, MAO-B inhibitors) OR reduce cholinergic tone (anticholinergics). Both approaches restore the balance, though by different mechanisms.
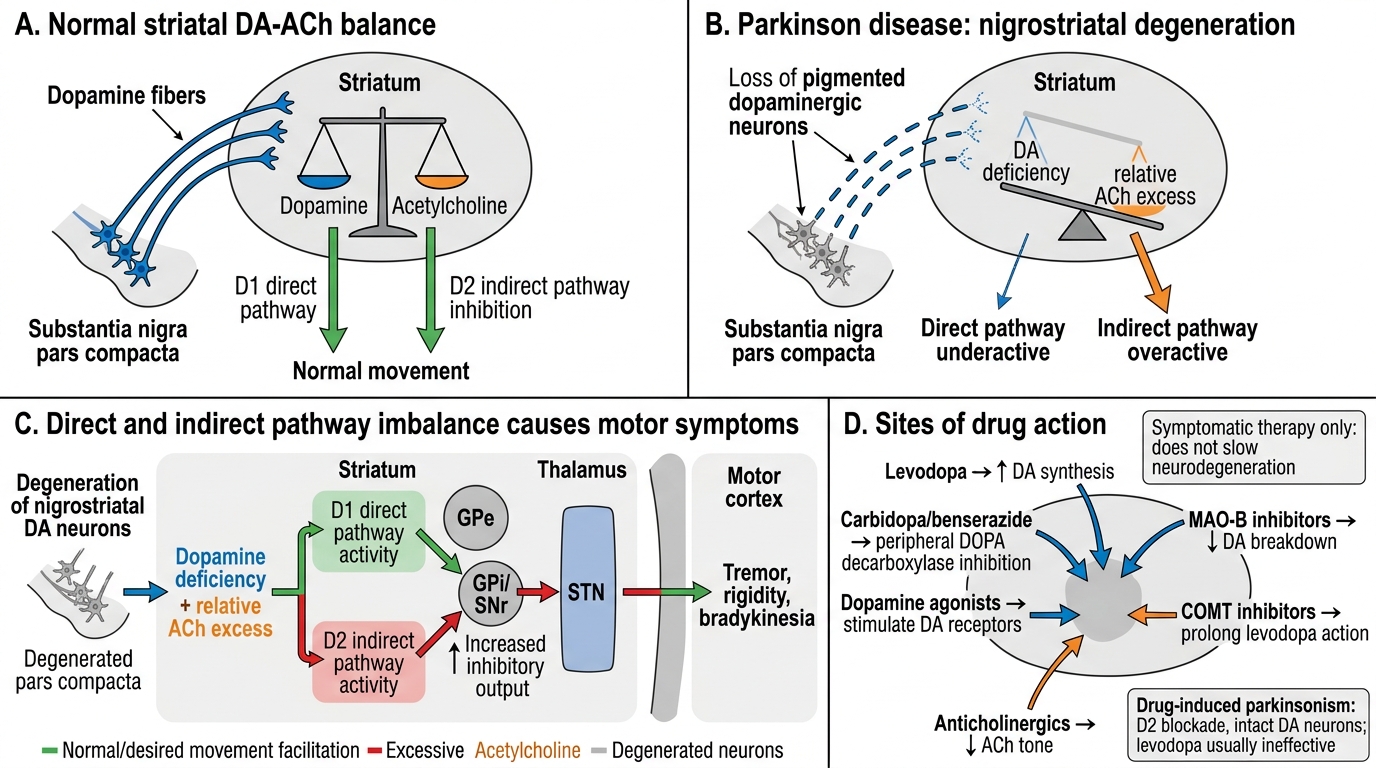
Dopamine-Acetylcholine Imbalance in Parkinson Disease
Therapeutic Goals in Parkinson's Disease Management
The therapeutic goals of PD pharmacotherapy are: (1) restore functional dopamine-acetylcholine balance in the striatum to reduce motor disability; (2) maintain quality of life and independence for as long as possible; (3) minimise the long-term motor complications of dopaminergic therapy (on-off fluctuations, peak-dose dyskinesias). Critically, current drugs are symptomatic, not neuroprotective — they compensate for lost dopamine but do not slow disease progression.
For drug-induced parkinsonism (DIP) — caused by D2 receptor blockade by antipsychotics (haloperidol, chlorpromazine, risperidone) or antiemetics (metoclopramide) — the therapeutic goal is to restore striatal dopamine-acetylcholine balance by reducing cholinergic excess with anticholinergic drugs. DIP differs from idiopathic PD in that: (a) it is potentially reversible on stopping or reducing the offending drug, and (b) the dopamine pathway is intact — the problem is functional blockade of D2 receptors, not loss of dopaminergic neurons. Therefore, levodopa does not help DIP — it cannot overcome receptor blockade by the antipsychotic. If haloperidol is the cause, increasing levodopa would also worsen the psychosis being treated.
The three-priority sequencing in clinical management:
- Early PD (young patient, mild symptoms): dopamine agonist monotherapy (pramipexole, ropinirole) first — delays levodopa exposure and its long-term complications
- Established PD with significant disability: levodopa/carbidopa (gold standard) with titration to effect
- Drug-induced parkinsonism: anticholinergic (trihexyphenidyl, benztropine) + review offending drug
Classification of Antiparkinsonian Drugs
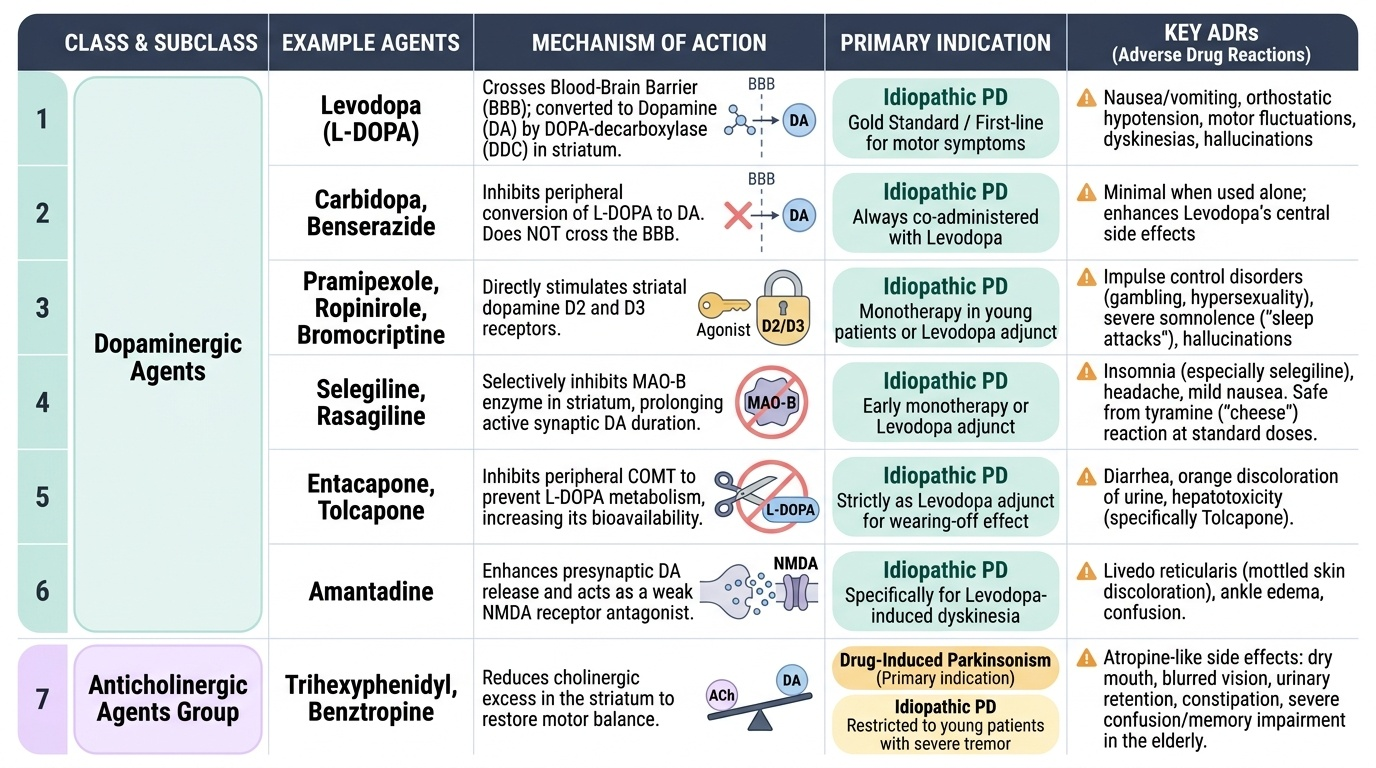
Antiparkinsonian drugs are classified into two mechanistic groups — dopaminergic (restore dopaminergic tone by various means) and anticholinergic (reduce cholinergic excess).
Provided image
Dopaminergic agents:
1. Levodopa (L-DOPA) — precursor to dopamine, crosses the BBB and is converted to DA by DOPA-decarboxylase (DDC) in the striatum. Always combined with a peripheral DDC inhibitor.
2. Peripheral DDC inhibitors — carbidopa (North America, global), benserazide (Europe): block peripheral conversion of L-DOPA to DA, reducing nausea/vomiting and allowing lower levodopa doses. Do NOT cross BBB.
3. Dopamine receptor agonists — pramipexole, ropinirole (non-ergot D2/D3 agonists); bromocriptine (ergot D2 agonist, less used now). Act directly on striatal dopamine receptors.
4. MAO-B inhibitors — selegiline, rasagiline: selectively inhibit MAO-B (which metabolises dopamine in the striatum) — increase synaptic DA duration. At standard doses, MAO-A is preserved → no tyramine reaction (distinguishes selegiline from phenelzine/non-selective MAOIs).
5. COMT inhibitors — entacapone, tolcapone: block catechol-O-methyl transferase, reducing peripheral L-DOPA metabolism → increases L-DOPA bioavailability and duration. Used as levodopa adjuncts.
6. Amantadine — antiviral that releases presynaptic dopamine + weak NMDA antagonist; mild antiparkinsonian effect; particularly useful for levodopa-induced dyskinesias (NMDA antagonism is the proposed mechanism for this indication).
Anticholinergic agents:
- Trihexyphenidyl (benzhexol), benztropine — block muscarinic receptors in the striatum (and elsewhere in CNS), reducing the relative cholinergic excess. Particularly effective for tremor and for drug-induced parkinsonism. ADRs: anticholinergic effects (dry mouth, constipation, urinary retention, blurred vision, memory impairment — particularly problematic in elderly).