Page 25 of 34
PH3.9 | PH3.9 | Dependence-Producing Drugs and De-Addiction Management — SDL Guide — SDL Guide
Learning Objectives
- Classify dependence-producing drugs into stimulants, depressants, psychedelics, and drugs used for criminal offences, with key agents and mechanisms in each category
- Explain the neurobiological basis of drug dependence (mesolimbic reward pathway) and the concepts of tolerance, physical and psychological dependence, and withdrawal
- Describe the pharmacotherapy of opioid use disorder (buprenorphine/naloxone, methadone, naltrexone) and tobacco use disorder (NRT, varenicline)
- Identify drugs used for drug-facilitated sexual assault and describe the forensic implications
INSTRUCTIONS
Substance use disorders are among the most prevalent and burdensome health problems globally. As a future clinician you will encounter patients with dependence disorders in every setting — wards, emergency departments, and community clinics. Equally important, you may encounter cases of drug-facilitated sexual assault involving pharmacological agents you must recognise. This module provides the pharmacological foundation for recognising, understanding, and managing drug dependence across its spectrum.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 34 (Drug Addiction, Dependence and Drug Abuse) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 24 (Drug Addiction) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man presents to the addiction medicine clinic requesting help to stop injecting heroin. He has been using for four years, currently injecting 2-3 times daily. He has tried to stop three times on his own but each time by the 12-hour mark he develops unbearable muscle cramps, diarrhoea, and sweating; by 24 hours he cannot function. He says he is 'not trying to get high anymore — I just can't face the withdrawal.' This man has severe opioid use disorder. The pharmacological basis of his dependence — mesolimbic dopamine reward circuit adaptation, physical opioid dependence, and withdrawal — and the evidence-based de-addiction pharmacotherapy (buprenorphine/naloxone) that can give him a safe path to abstinence — are what this module is about.
WHY THIS MATTERS
Drug dependence disorders will be among the most common conditions you encounter in clinical practice. Globally, opioid, alcohol, cannabis, tobacco, and stimulant use disorders account for enormous morbidity and mortality. You will be expected to recognise drug-seeking behaviour, manage withdrawal safely, prescribe appropriate de-addiction pharmacotherapy, and — increasingly — recognise presentations consistent with drug-facilitated sexual assault (DFSA) involving pharmacological agents with amnesia properties. The pharmacological knowledge in this module is directly applicable to these scenarios.
RECALL
Recall from earlier in this cluster: the mesolimbic dopamine pathway (VTA → nucleus accumbens) mediates reward and motivation — it is the circuit activated by food, sex, social interaction, and — aberrantly — by all dependence-producing drugs. Recall from PH3.4: opioids act via μ-receptors on GABAergic interneurons in the VTA, disinhibiting dopamine neurons and increasing DA in the nucleus accumbens (indirect reward mechanism). Recall from PH3.2: benzodiazepines enhance GABA-A inhibitory tone; physical dependence develops with daily use beyond 4 weeks; withdrawal resembles alcohol withdrawal. Recall from PH3.8: disulfiram (ALDH inhibitor — aversive deterrent) and naltrexone (μ-opioid antagonist — reduces alcohol reward) are used in alcohol use disorder.
Pathophysiology of Drug Dependence — Reward Circuitry
All dependence-producing drugs, despite their pharmacological diversity, converge on the mesolimbic dopamine reward pathway — specifically, on increasing dopamine release in the nucleus accumbens (NAc) from dopaminergic neurons originating in the ventral tegmental area (VTA). This convergence explains why drugs as structurally different as heroin, cocaine, alcohol, and nicotine all produce subjectively similar reinforcement and why they share a common neurobiological substrate for addiction.
Mechanisms of convergence on the reward pathway:
- Direct DA release enhancers: cocaine and amphetamines directly increase DA concentration in the NAc by blocking the dopamine transporter (DAT) [cocaine] or reversing DAT/NET to release catecholamines [amphetamines]
- Indirect DA disinhibition: opioids activate μ-receptors on GABAergic interneurons in the VTA, inhibiting GABA release and thereby removing the tonic inhibition of dopamine neurons — net: increased DA release in NAc
- GABA-A potentiation (alcohol, BZDs): indirectly affect the reward circuit; GABA enhancers in the NAc suppress the aversive/withdrawal-related neurotransmission
- Nicotine: activates α₄β₂ nicotinic ACh receptors on VTA dopamine neurons → direct dopamine neuron stimulation → DA release in NAc
- Cannabis (THC): CB₁ receptor activation on GABAergic interneurons in VTA (disinhibition) and directly on NAc neurons
Neuroadaptation — the basis of tolerance and withdrawal:
Chronic drug exposure causes compensatory neuroplastic changes: down-regulation of reward circuit sensitivity (tolerance), up-regulation of opposing stress/anti-reward circuits. When the drug is withdrawn, the sensitised stress circuits dominate — producing the withdrawal syndrome (anxiety, dysphoria, craving, physiological symptoms). Physical dependence (measurable physiological withdrawal) is most pronounced with opioids, alcohol, and BZDs. Psychological dependence (craving, compulsive drug-seeking despite adverse consequences) is the hallmark of all addictions.
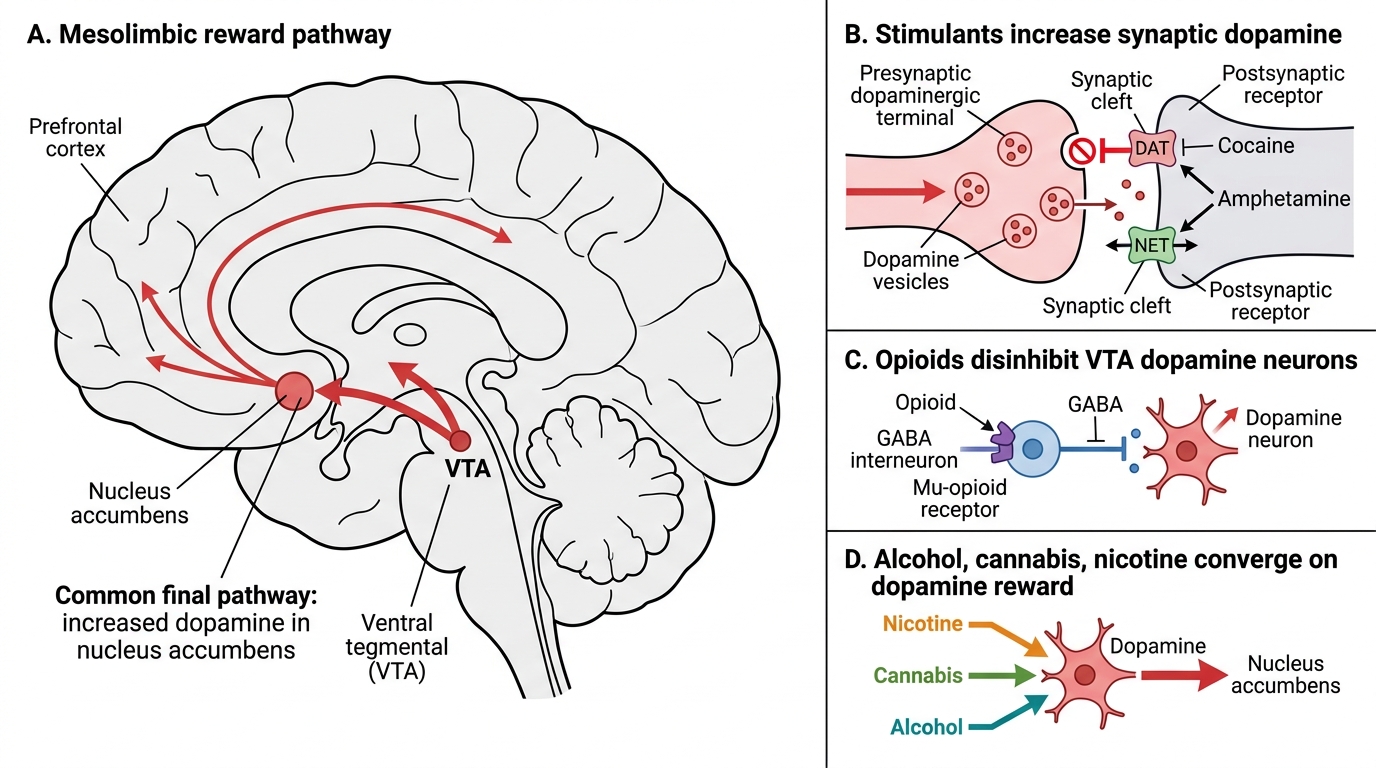
Mesolimbic Dopamine Reward Pathway and Drugs of Addiction
Goals of De-Addiction Management
The pharmacological goals of de-addiction management follow a three-phase model:
Phase 1 — Detoxification (safe withdrawal): manage the acute physiological withdrawal syndrome safely, preventing life-threatening complications (withdrawal seizures in opioid/alcohol dependence, respiratory depression if precipitated abruptly). This is a purely medical intervention — it is NOT treatment of the dependence itself.
Phase 2 — Maintenance and relapse prevention: pharmacotherapy that reduces craving, blocks the reward of drug use, or provides a safer substitute (substitution therapy). This is the pharmacologically active phase of treatment.
Phase 3 — Rehabilitation and psychosocial support: pharmacotherapy alone has limited long-term efficacy without concurrent psychological (CBT, motivational interviewing) and social support (housing, employment, peer support). The pharmacotherapy creates a window of physiological stability within which these interventions can work.
Harm reduction is an evidence-based framework that accepts that not all patients can achieve immediate abstinence — and that reducing harm (clean needles, naloxone distribution to prevent overdose death, supervised consumption) saves lives even when abstinence is not achieved.
The de-addiction process and steps per the competency:
1. Assessment (severity of dependence, physical/psychiatric comorbidities)
2. Detoxification (medically supervised withdrawal management)
3. Substitution/maintenance pharmacotherapy (where applicable: methadone, buprenorphine for OUD; NRT for tobacco)
4. Relapse prevention pharmacotherapy (naltrexone for opioid/alcohol; varenicline for tobacco)
5. Psychosocial rehabilitation
6. Long-term follow-up and relapse management
Classification of Dependence-Producing Drugs
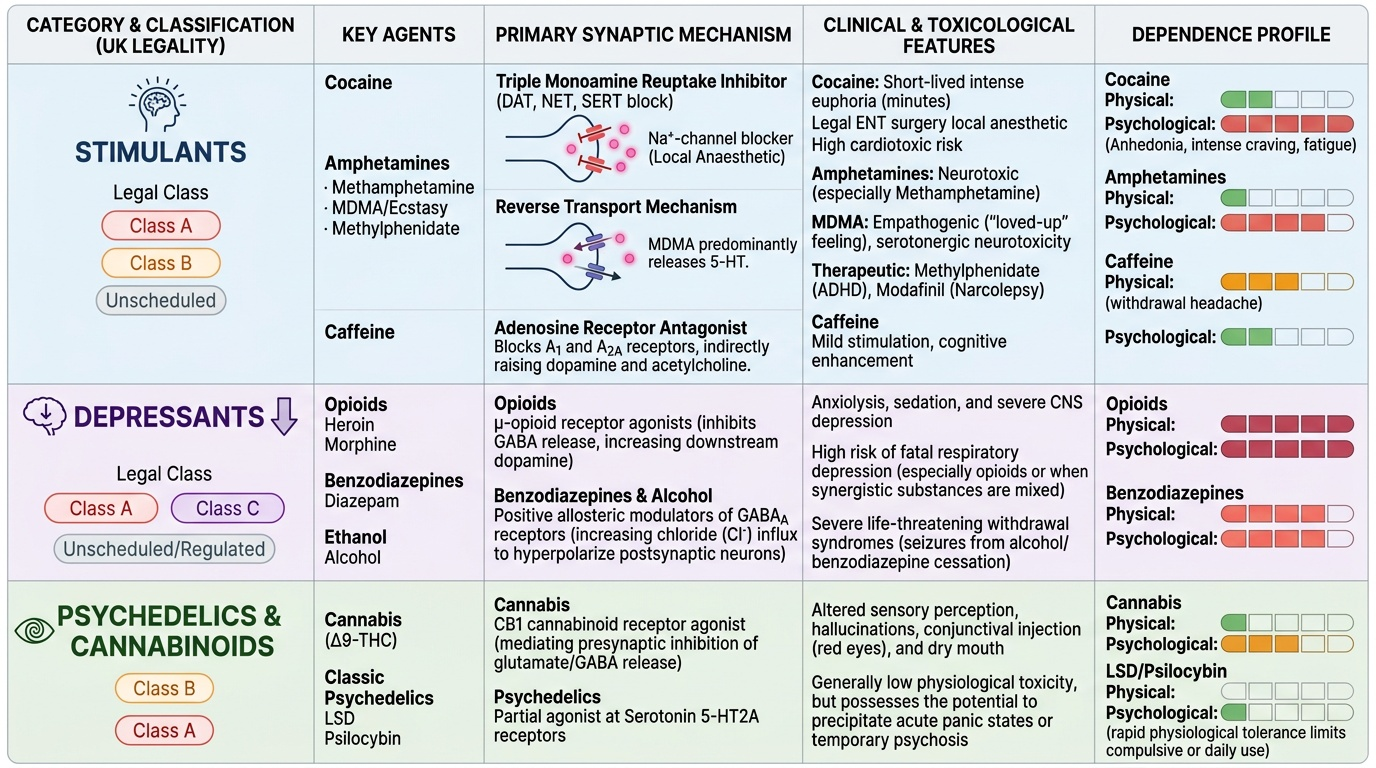
The NMC competency (PH3.9) specifies four categories of dependence-producing drugs, each of which must be covered:
1. Stimulants: drugs that increase CNS activation and catecholaminergic activity.
- Cocaine: blocks DAT, NET, and SERT simultaneously (reuptake inhibitor); massive DA, NA, and 5-HT accumulation in the synapse. Euphoria, intense but short-lived (minutes). Also a local anaesthetic (Na⁺-channel block — legitimately used in ENT surgery). Physical withdrawal is mild but psychological withdrawal (craving, anhedonia, fatigue) is severe.
- Amphetamines (including methamphetamine, MDMA): act as reverse transporters — enter the nerve terminal via DAT/NET, cause reversal of the transporter to actively export DA/NA into the synapse; also block reuptake. Methamphetamine is highly neurotoxic. MDMA ('ecstasy') is amphetamine-related but predominantly a 5-HT releaser (also DA/NA) — produces empathogenic effects ('loved-up' feeling), long-term serotonergic neurotoxicity. Therapeutic use: methylphenidate (more selective DA/NA reuptake inhibitor) for ADHD; modafinil for narcolepsy.
- Caffeine: adenosine receptor antagonist — blocks A₁ and A₂A receptors in basal ganglia and cortex, increasing dopaminergic and cholinergic tone indirectly. Mild stimulant; dependence (mild headache withdrawal) is the most widely experienced drug dependence in the world.
2. Depressants: drugs producing CNS depression.
- Cannabis, opioids, alcohol, benzodiazepines (covered in PH3.4, PH3.8, PH3.2 respectively — brief cross-reference here).
- Cannabis (delta-9-THC): CB₁ agonist (brain: hippocampus, amygdala, basal ganglia, cerebellum → impaired memory, anxiety, altered motor coordination); CB₂ (periphery, immune cells). Amotivational syndrome (chronic heavy use). Psychological dependence; mild physical withdrawal (irritability, insomnia, decreased appetite).
3. Psychedelics/Hallucinogens:
- LSD (lysergic acid diethylamide): partial agonist at 5-HT₂A receptors in the prefrontal cortex and thalamus — disrupts sensory processing, produces vivid visual hallucinations, altered time perception, synesthesia. Tolerance develops rapidly (requires increasingly large doses for effect within days). No physical dependence. No significant withdrawal. Risk of hallucinogen persisting perception disorder (HPPD) (flashbacks).
- Psilocybin (magic mushrooms): also 5-HT₂A agonist — similar to LSD.
- Ketamine (PH3.1 cross-ref): NMDA antagonist — dissociative anaesthetic; at sub-anaesthetic doses, produces euphoria and perceptual distortions; psychological dependence; bladder toxicity with chronic use.
- PCP (phencyclidine): NMDA antagonist; more neurotoxic than ketamine.
4. Drugs used for criminal offences (drug-facilitated sexual assault — DFSA):
- GHB (gamma-hydroxybutyrate): GABA-B receptor agonist + GHB receptor agonist → sedation + anterograde amnesia. Colourless, nearly tasteless, dissolves in drinks. Produces rapid sedation and immobility at high doses. Detection window: only 4-8 hours in urine — forensic specimens must be collected early. Also abused for euphoria (medical grade: sodium oxybate for narcolepsy).
- Flunitrazepam (Rohypnol): potent high-dose BZD — anterograde amnesia, profound sedation. Originally produced tablets that dissolved clearly in liquid; newer formulations dye the drink blue to aid detection.
- Ketamine: used for DFSA in nightclub settings.
- Scopolamine (anticholinergic): causes amnesia and suggestibility — used in some DFSA contexts in South America.
Provided image