Page 24 of 33
PH4.1-4 | PH4.1-4 | Drugs Affecting Blood and Coagulation — SDL Guide (Part 2)
Haematinics and Anti-Thrombocytopenia Drugs
Iron therapy — iron deficiency anaemia: Iron is absorbed as ferrous (Fe2+) from the duodenum and upper jejunum. Ferrous salts (ferrous sulphate, ferrous fumarate, ferrous gluconate) are the first-line oral treatment. Ferrous sulphate 200 mg TDS is the standard prescription — each tablet contains ~65 mg elemental iron; 3 tablets/day provides ~195 mg elemental iron, sufficient for haemoglobin restoration (~0.1 g/dL per day) with adequate absorption (~10–20% of ingested iron).
Oral iron pharmacokinetics and ADRs: absorption enhanced by vitamin C (ascorbate reduces Fe3+ to Fe2+, and acidic environment aids dissolution); inhibited by food, antacids, calcium, tetracyclines, PPIs. ADRs: constipation, nausea, dark stools, abdominal discomfort — dose-related. If intolerant: reduce dose, take with food (reduces absorption ~30%), or switch to ferrous gluconate (better tolerated).
IV iron (ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran): indicated for: (1) oral iron intolerance or non-compliance; (2) malabsorption (coeliac, post-gastrectomy); (3) iron deficiency in CKD (impaired absorption + needs of EPO therapy); (4) pregnancy with severe/late iron deficiency; (5) inflammatory bowel disease (oral iron worsens mucosal inflammation). IV iron provides complete replacement in fewer doses — ferric carboxymaltose can replace the entire iron deficit in 1–2 IV infusions.
Vitamin B12 and folate — megaloblastic anaemia:
- B12 (cobalamin): found in animal products; dietary deficiency in strict vegans; malabsorption in pernicious anaemia (absent IF), gastrectomy, and terminal ileal disease. Hydroxocobalamin IM: standard treatment for all causes where absorption is impaired (pernicious anaemia, gastrectomy, ileal disease). Cyanocobalamin (oral or IM): oral form appropriate only when IF is present (dietary B12 deficiency). The 'nerve damage' of B12 deficiency (subacute combined degeneration of the spinal cord — posterior and lateral column demyelination) is irreversible if untreated for months; B12 must be started promptly.
- Folic acid: derived from green vegetables, legumes; essential for DNA synthesis (one-carbon transfer reactions). Deficiency → megaloblastic anaemia (indistinguishable from B12 deficiency on blood film). Treatment: oral folic acid 5 mg daily. CRITICAL WARNING: Never give folic acid alone in mixed B12+folate deficiency without first ensuring B12 is also being treated — folic acid corrects the anaemia but does not protect the nervous system → the subacute combined degeneration progresses, the anaemia resolves, and the neurological damage is masked until severe.
Erythropoietin (EPO) and G-CSF:
- Epoetin alfa/beta, darbepoetin alfa (ESAs): recombinant EPO stimulates erythroid progenitors (CFU-E) in bone marrow → increased RBC production. Indicated for: renal anaemia of CKD (most important), chemotherapy-induced anaemia. ADRs: hypertension (↑blood viscosity + direct vascular effect — monitor BP), thrombosis (increased haematocrit → higher blood viscosity), antibody-mediated pure red cell aplasia (rare but serious — due to anti-EPO antibodies).
- G-CSF (filgrastim, pegfilgrastim): stimulates granulocyte colony-forming units → ↑neutrophil production. Used for: chemotherapy-induced neutropenia (prophylaxis and treatment), febrile neutropenia, stem cell mobilisation before harvest. ADRs: bone pain (medullary expansion), splenic rupture (rare — related to splenic enlargement from stem cell mobilisation).
Thrombocytopenia — immune thrombocytopenic purpura (ITP) pharmacotherapy:
ITP requires pharmacological intervention when platelets <30,000/μL (or <50,000 with bleeding):
1. Corticosteroids (prednisolone 1 mg/kg/day oral or IV dexamethasone) — first-line; suppress autoantibody production; increase platelet survival; onset 3–7 days. Response in ~70% but relapse common after steroid taper.
2. IVIg (IV immunoglobulin) (1 g/kg × 2 doses): rapidly raises platelet count within 24–48h by blocking Fc receptors on splenic macrophages (prevents opsonised platelet destruction) + anti-idiotype effects. Used for acute severe ITP, pre-surgery, pregnancy-associated ITP. Effect is temporary (1–3 weeks).
3. TPO receptor agonists — eltrombopag (oral), romiplostim (SC weekly): stimulate thrombopoietin receptors (c-Mpl) on megakaryocytes → increased platelet production. Used for chronic/refractory ITP after steroids + IVIg have failed or in patients unsuitable for splenectomy. Eltrombopag must be taken on an empty stomach (chelates polyvalent cations — no milk/antacids within 4h).
4. Anti-D immunoglobulin (in Rh-positive splenectomy-intact patients): binds to D antigen on RBCs → FcγR blockade → platelet sparing. Limited use; requires Rh-positive and intact spleen.
5. Splenectomy: removes the primary site of platelet destruction and anti-platelet antibody production; durable remission in ~70%.
Anticoagulants: Heparin, LMWH, Warfarin, and DOACs
Anticoagulants prevent the formation of fibrin by interfering with the coagulation cascade at different points. Choosing the appropriate agent requires matching the clinical indication, renal function, need for monitoring, reversal options, and patient adherence profile.
Unfractionated heparin (UFH): A heterogeneous mixture of glycosaminoglycans that binds and activates antithrombin III (ATIII) → ATIII inhibits thrombin (IIa), Factor Xa, IXa, XIa (thrombin inhibition is the dominant anticoagulant effect at therapeutic doses). UFH: IV infusion (standard for VTE treatment, ACS, cardiac surgery) or SC injection (prophylaxis). Monitoring: aPTT (target 60–100 seconds, or 1.5–2.5× normal control), checked every 6h until therapeutic, then daily. Reversal: protamine sulphate (positively charged; binds negatively charged heparin; 1 mg protamine neutralises 100 units UFH; give slowly — can cause bradycardia, hypotension).
Low-molecular-weight heparin (LMWH — enoxaparin, dalteparin): Derived from UFH by depolymerisation; predominantly inhibit factor Xa (anti-Xa:anti-IIa ratio ~3:1 for enoxaparin). SC injection, predictable pharmacokinetics, no routine aPTT monitoring required (anti-Xa assay if monitoring needed — e.g., pregnancy, extremes of weight, renal impairment). Bioavailability ~90% SC (vs 30% for UFH SC). Preferred over UFH for VTE treatment and prevention in most clinical settings. Enoxaparin: therapeutic dose 1 mg/kg SC BD (treatment) or 40 mg SC OD (prophylaxis). Reduce dose in severe CKD (renally excreted); avoid if eGFR <30 (use UFH). Reversal: protamine sulphate (partial — ~60% anti-Xa reversal, complete anti-IIa reversal).
Fondaparinux: Synthetic pentasaccharide; selectively inhibits Factor Xa only (no direct anti-IIa); once-daily SC injection; predictable; no HIT risk (does not bind PF4-heparin complex — no antibody formation). Eliminated renally — contraindicated eGFR <20.
Warfarin (vitamin K antagonist): Inhibits vitamin K epoxide reductase complex (VKORC) → prevents regeneration of reduced vitamin K → cannot carboxylate the vitamin K-dependent clotting factors (II, VII, IX, X) and anticoagulant proteins (C, S, Z). Takes 3–5 days to achieve full anticoagulant effect (half-lives of factors must fall — Factor VII shortest t½ ~6h causes initial PT/INR rise; Factor II longest ~60h causes the therapeutic anticoagulant effect). Monitoring: INR (normal 1.0; target 2.0–3.0 for AF and VTE; 2.5–3.5 for mechanical heart valves). Bridging with LMWH required at initiation and around procedures.
Warfarin has an extremely narrow therapeutic index and is affected by: (1) Genetic factors: VKORC1 polymorphisms (higher sensitivity → lower dose needed); CYP2C9 polymorphisms (slower warfarin metabolism → higher levels → higher INR). (2) Drug interactions: enzyme inducers reduce warfarin effect (rifampicin, carbamazepine, phenytoin → ↑CYP2C9 → faster warfarin metabolism → ↓INR); enzyme inhibitors increase warfarin effect (amiodarone, fluconazole, metronidazole → ↓CYP2C9 → slower metabolism → ↑INR → bleeding). (3) Dietary vitamin K: large fluctuations in green leafy vegetable consumption affect INR (vitamin K is warfarin's antagonist — more vitamin K → ↑factor synthesis → ↓INR).
Warfarin reversal: Minor bleeding → withhold warfarin, check INR; major bleeding → vitamin K 5–10 mg IV (onset 6–24h for factor synthesis) + prothrombin complex concentrate (PCC) (4-factor PCC: factors II, VII, IX, X — immediate INR correction); life-threatening bleeding → PCC + FFP if PCC unavailable.
Direct oral anticoagulants (DOACs): Act directly on thrombin (dabigatran) or Factor Xa (rivaroxaban, apixaban, edoxaban) without requiring antithrombin III as cofactor. Advantages over warfarin: (1) no routine monitoring; (2) predictable pharmacokinetics; (3) fewer drug interactions; (4) fixed dosing; (5) faster onset (2–4h) and offset (12–24h); (6) non-inferior to warfarin for stroke prevention in AF with better bleeding profiles (ARISTOTLE: apixaban superior to warfarin — less stroke/SE AND less major bleeding).
- Dabigatran (Pradaxa): direct thrombin inhibitor; oral pro-drug dabigatran etexilate → dabigatran (active); predominantly renally excreted (>80% — dose-reduce in CKD, avoid if eGFR <30); reversal agent: idarucizumab (specific humanised monoclonal Ab antidote, Praxbind).
- Rivaroxaban, apixaban, edoxaban: direct Factor Xa inhibitors; hepatic metabolism ± renal excretion; reversal: andexanet alfa (recombinant modified Xa mimic that sequesters Xa inhibitors — expensive, not universally available) or PCC (non-specific; used for life-threatening bleeding when andexanet unavailable).
Heparin-induced thrombocytopenia (HIT type II): Immune complication of heparin therapy. Anti-PF4-heparin complex antibodies activate platelets → platelet consumption (thrombocytopenia) AND pro-thrombotic state (paradoxical thrombosis despite low platelets). Diagnosis: platelet fall >50% from baseline, occurring 5–10 days after heparin initiation (or faster if prior heparin exposure); 4T score + anti-PF4-heparin antibody ELISA. Management: stop ALL heparin immediately (including heparin flushes, LMWH, heparin-coated catheters); switch to a NON-heparin anticoagulant (argatroban IV — direct thrombin inhibitor; fondaparinux; bivalirudin). Do NOT give warfarin alone (protein C falls faster → initial hypercoagulable state; warfarin may worsen HIT-associated thrombosis initially). Monitor platelets daily until recovery.
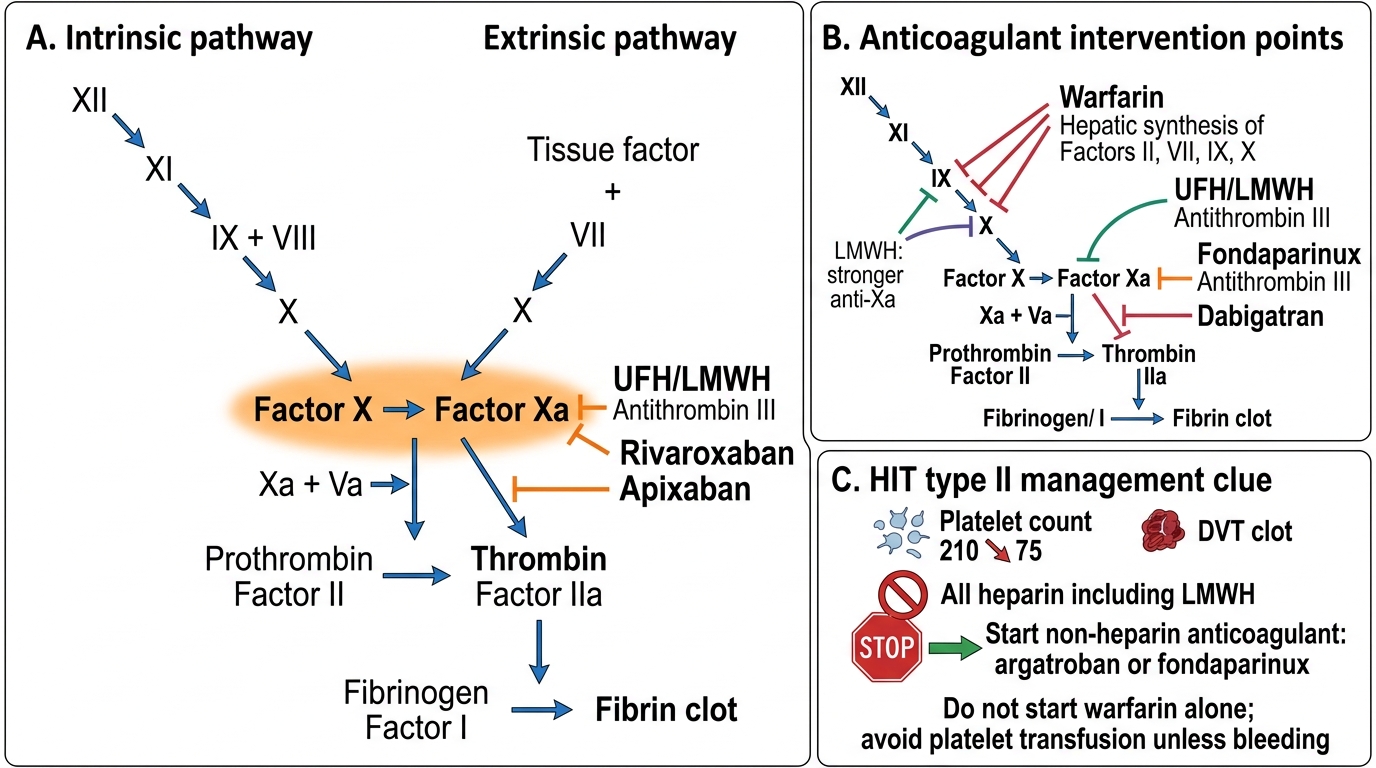
Coagulation Cascade and Anticoagulant Targets
SELF-CHECK
A patient develops a platelet count fall from 210 to 75 (>50% fall) 7 days after starting UFH for DVT treatment. New right arm DVT noted despite anticoagulation. What is the immediate management?
A. Increase UFH dose — the DVT extension means inadequate anticoagulation
B. Switch to LMWH (enoxaparin) — it has less HIT risk than UFH
C. Stop all heparin immediately and start argatroban (or fondaparinux); do NOT start warfarin alone
D. Transfuse platelets to restore platelet count before switching anticoagulant
Reveal Answer
Answer: C. Stop all heparin immediately and start argatroban (or fondaparinux); do NOT start warfarin alone
This presentation is consistent with HIT type II: platelet fall >50% from baseline at 5–10 days post-heparin + new thrombosis (paradoxical thrombosis despite anticoagulation). The immediate management is to STOP all heparin — including LMWH (cross-reactive antibodies) — and substitute a non-heparin anticoagulant (argatroban, fondaparinux, or bivalirudin). LMWH is not safe — HIT antibodies cross-react with LMWH. Platelet transfusion is contraindicated (adds substrate for thrombosis in the pro-thrombotic HIT milieu —'fuel to the fire'). Warfarin should NOT be started alone initially — protein C (an anticoagulant) has a short half-life and falls rapidly on warfarin initiation → initial hypercoagulable state worsens HIT thrombosis.
Fibrinolytics, Antifibrinolytics, and Antiplatelets
Fibrinolytic therapy (thrombolysis): Fibrinolytics convert plasminogen → plasmin, which dissolves fibrin. They are indicated for life-threatening thromboembolic emergencies where rapid clot lysis is essential.
Streptokinase: bacterial protein (from β-haemolytic Streptococcus); forms a complex with plasminogen → activates free plasminogen in plasma AND on fibrin → non-fibrin-specific systemic fibrinolytic state (haemorrhagic risk). 1.5 million IU IV over 60 minutes. Allergic reactions (urticaria, anaphylaxis) occur in ~5%. Antibodies form after first use → re-administration is ineffective and dangerous (neutralised by antibodies; risk of anaphylaxis); can only be used once. Cheapest fibrinolytic; widely used in resource-limited settings for STEMI.
Alteplase (tPA) and tenecteplase: recombinant tissue plasminogen activators; fibrin-specific (bind fibrin-bound plasminogen preferentially → localised fibrinolysis with less systemic plasminogen depletion). Do not form antibodies → can be used multiple times; no allergic reactions. Alteplase: accelerated IV regimen (15 mg IV bolus + 0.75 mg/kg over 30 min + 0.5 mg/kg over 60 min, max 100 mg); used for STEMI, massive PE, ischaemic stroke. Tenecteplase: single IV weight-based bolus — simplest to administer (important in STEMI when speed is critical).
Fibrinolytic contraindications — mandatory to screen before giving fibrinolytics:
Absolute: prior intracranial haemorrhage; ischaemic stroke <3 months; known intracranial structural lesion; active significant bleeding; suspected aortic dissection; closed head trauma <3 months.
Relative: uncontrolled hypertension (SBP >180 mmHg); current anticoagulation; traumatic CPR; pregnancy (thrombolytics cross placenta; relative contraindication); recent major surgery (<3 weeks).
Antifibrinolytic agents:
Tranexamic acid (TXA) and aminocaproic acid (ε-ACA): synthetic lysine analogues that competitively bind lysine-binding sites on plasminogen, preventing its activation to plasmin and preventing plasmin from binding fibrin. Result: fibrinolysis is inhibited → clot stabilisation. Uses: (1) trauma haemorrhage — CRASH-2 trial: IV TXA within 3 hours of injury significantly reduced mortality from bleeding in adult trauma patients (1g IV over 10 min, then 1g over 8h); (2) surgical bleeding (cardiac bypass, orthopaedic surgery); (3) heavy menstrual bleeding (oral TXA 1g TDS); (4) epistaxis and dental extraction in haemophilia; (5) postpartum haemorrhage (WHO recommends TXA as adjunct). Aprotinin: serine protease inhibitor (also blocks plasmin + kallikrein); use restricted due to renal toxicity concerns (BART trial); reserved for cardiac surgery.
Antiplatelet drugs (PH4.4):
Aspirin (acetylsalicylic acid): irreversibly acetylates COX-1 in platelets → permanent inhibition of TXA2 synthesis for platelet lifetime (~7–10 days). Loading dose 300 mg (chewed) for ACS; maintenance 75–100 mg/day. Also blocks COX-2 at higher doses → anti-inflammatory, antipyretic. Key cardiovascular indication: ACS (ISIS-2: 25% mortality reduction), secondary prevention post-MI, ischaemic stroke prevention.
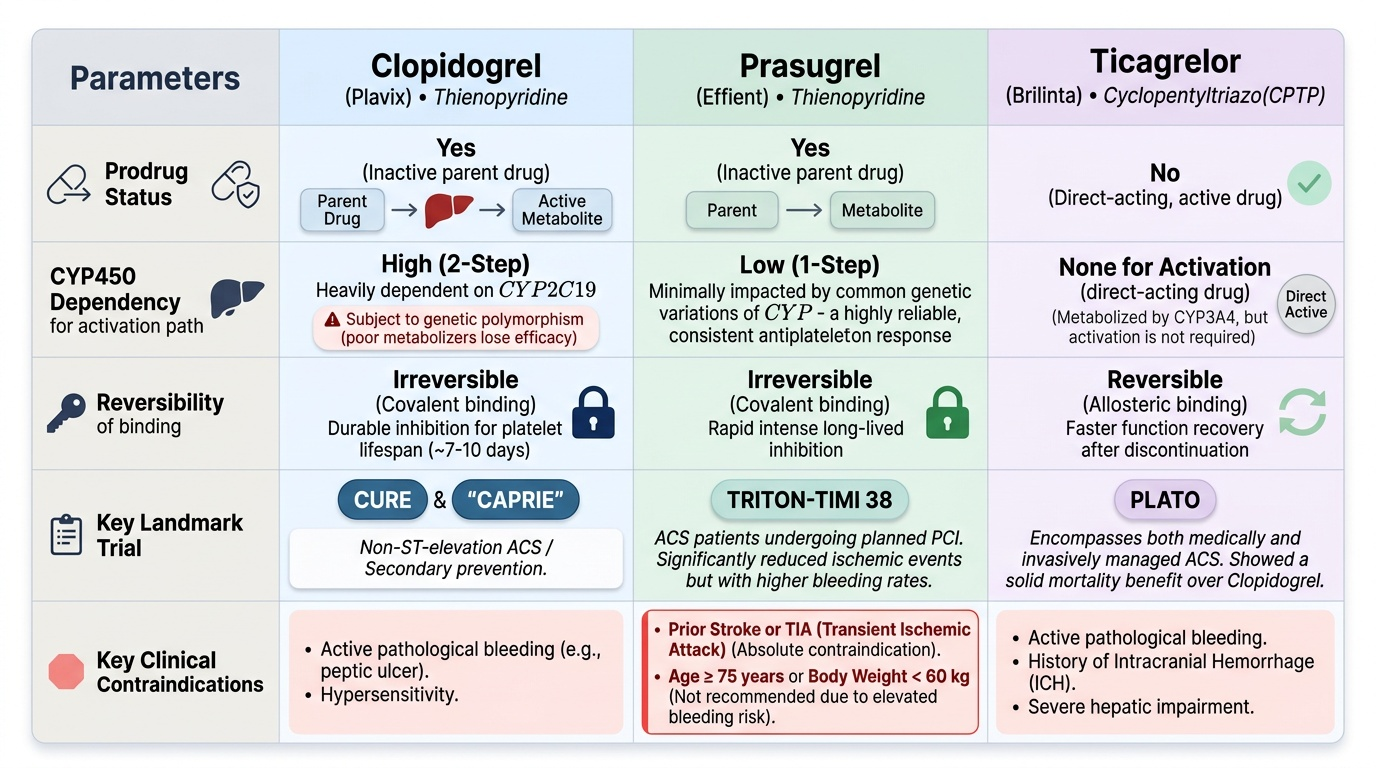
P2Y12 inhibitors: Block ADP-mediated platelet activation at the P2Y12 receptor:
- Clopidogrel (Plavix): thienopyridine prodrug → CYP2C19 in liver → active thiol metabolite; irreversible P2Y12 blockade; CYP2C19 loss-of-function polymorphisms → reduced efficacy (clopidogrel 'non-responders').
- Ticagrelor (Brilinta): cyclopentyl-triazolopyrimidine; NOT a prodrug; reversible P2Y12 blockade; active as ingested; no CYP2C19 dependency; PLATO trial: superior to clopidogrel in ACS (CV death + MI + stroke: 9.8% vs 11.7%); side effects: dyspnoea (adenosine reuptake inhibition), bradycardia, ↑uric acid.
- Prasugrel (Effient): thienopyridine prodrug; single-step hepatic activation (faster than clopidogrel's two-step); irreversible; TRITON-TIMI 38: superior to clopidogrel in ACS/PCI for ischaemic events + more bleeding; absolute contraindications: prior stroke/TIA (increased intracranial bleeding), age >75 years, weight <60 kg (poor net clinical benefit).
GPIIb/IIIa inhibitors (abciximab, eptifibatide, tirofiban): Block the final common pathway of platelet aggregation (GPIIb/IIIa receptor + fibrinogen bridging). IV only; used adjunctively during PCI for high-risk ACS. Very potent platelet inhibition → high bleeding risk.
Dipyridamole: Inhibits phosphodiesterase (↑cAMP in platelets) + blocks adenosine reuptake (→ ↑adenosine → A2 receptor → ↑cAMP). Used in modified-release combination with aspirin (Aggrenox) for secondary stroke prevention (ESPS-2 trial).
Provided image
SELF-CHECK
A patient with AF on warfarin (INR 2.4) presents with acute ischaemic stroke onset 2 hours ago. The neurologist wants to give IV alteplase. What is the most important contraindication to consider?
A. The INR of 2.4 is within the therapeutic range — alteplase can be safely given
B. Current anticoagulation with INR >1.7 is an absolute contraindication to IV alteplase for acute stroke
C. Aspirin should be given instead of alteplase in this situation
D. Warfarin should be reversed first with vitamin K, then alteplase given
Reveal Answer
Answer: B. Current anticoagulation with INR >1.7 is an absolute contraindication to IV alteplase for acute stroke
Current anticoagulation with INR >1.7 is an absolute contraindication to IV alteplase in acute ischaemic stroke per most stroke thrombolysis guidelines (AHA/ASA, ESO). Even though the patient's INR is 2.4 (within the 2.0–3.0 therapeutic range for AF), thrombolysis on top of anticoagulation dramatically increases the risk of haemorrhagic transformation of the infarct → intracranial haemorrhage. Alteplase cannot be safely given. The appropriate approach: admit to stroke unit, withhold anticoagulation acutely, consider aspirin after 24h (and ensure no haemorrhagic transformation on imaging), then restart anticoagulation. Rapid reversal of warfarin + then thrombolysis is not standard practice and would still leave the patient in a high-risk state. Mechanical thrombectomy (endovascular) may be possible within the extended time window.
CLINICAL PEARL
Anticoagulation in pregnancy — only heparin is safe: Every pregnant woman with VTE, mechanical heart valve, AF, or antiphospholipid syndrome requiring anticoagulation must receive heparin (UFH or LMWH). Warfarin crosses the placenta and causes 'warfarin embryopathy' in the first trimester (nasal hypoplasia, stippled epiphyses, limb hypoplasia), fetal intracranial haemorrhage in the second and third trimesters, and stillbirth. DOACs (dabigatran, rivaroxaban, apixaban) also cross the placenta and have insufficient safety data — absolutely contraindicated. LMWH (enoxaparin) is the preferred anticoagulant throughout pregnancy for VTE and prosthetic valve patients — it does NOT cross the placenta (too large for placental transfer) and has an established safety record in pregnancy. The notable exception: LMWH is switched to UFH near term (more predictable reversal with protamine for delivery). This 'heparin only in pregnancy' rule is one of the most important safety principles in obstetric pharmacology.