Page 4 of 33
PH4.5 | PH4.5 | Diuretics and Antidiuretic Drugs — SDL Guide
Learning Objectives
- Classify diuretics by site of action in the nephron and explain the mechanism of each class.
- Describe the pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of diuretics and antidiuretic drugs.
- Explain the mechanism of action of vasopressin (ADH) analogues and antagonists (vaptans), and their indications.
- Select the appropriate diuretic for a patient based on indication, renal function, and electrolyte profile.
INSTRUCTIONS
Diuretics are among the most frequently prescribed drugs in clinical medicine — used in hypertension, heart failure, oedema, acute pulmonary oedema, and liver disease. The flip side of their fluid-removing power is a predictable disruption of electrolyte balance: hypokalaemia, hyponatraemia, and metabolic alkalosis are everyday ward issues you will manage. Understanding the nephron-site-specific mechanisms and their electrolyte consequences will make you a safer, more precise prescriber across a wide range of clinical settings.
References
- Tripathi KD. Essentials of Medical Pharmacology, 9th ed., Ch. 40 (Diuretics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed., Ch. 25 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old man with known ischaemic cardiomyopathy (ejection fraction 30%) is admitted with acute breathlessness and bilateral crackles to the lung bases. Chest X-ray shows bilateral pulmonary oedema with cardiomegaly. His serum potassium is 3.2 mEq/L. He is already on furosemide 40 mg orally at home, along with carvedilol and enalapril. The registrar orders IV furosemide 80 mg stat. Thirty minutes later, the patient is passing large volumes of pale urine and his breathlessness improves. Two hours later, his potassium drops to 2.9 mEq/L. Which drug caused this? How do you manage it, and why did the oral dose fail while the IV dose worked?
WHY THIS MATTERS
Diuretics are the workhorses of fluid management across virtually every specialty in medicine. Cardiologists use them in heart failure and hypertension; hepatologists titrate them carefully in cirrhotic ascites; nephrologists use them in nephrotic syndrome; intensivists use mannitol for brain oedema. The antidiuretic arm — vasopressin analogues — is indispensable in managing diabetes insipidus, variceal bleeding (terlipressin), and nocturnal enuresis (desmopressin). Understanding which diuretic to use, at what dose, in which patient, and how to prevent and manage its electrolyte consequences is a core prescribing competency for any practising clinician.
RECALL
Recall from physiology (PY) and biochemistry (BI) the following:
- Nephron anatomy: Glomerulus → proximal convoluted tubule (PCT) → loop of Henle (thin descending, thin ascending, thick ascending limb, TAL) → distal convoluted tubule (DCT) → collecting duct. The TAL and DCT are the primary diuretic targets.
- Key transporters: NKCC2 (Na-K-2Cl cotransporter) in the TAL; NCC (Na-Cl cotransporter) in the early DCT; ENaC (epithelial Na channel) in the cortical collecting duct; carbonic anhydrase (CA) in the PCT.
- Aldosterone mechanism (BI/PY): mineralocorticoid receptor (MR) activation in principal cells → upregulates ENaC (apical) and Na-K-ATPase (basolateral) → sodium retention + potassium secretion + water retention. Spironolactone blocks this MR.
- ADH (vasopressin): released from posterior pituitary in response to hyperosmolality or hypovolaemia; acts on V2 receptors in collecting duct principal cells → adenylyl cyclase → cAMP → aquaporin-2 insertion → water reabsorption. Vasopressin also acts on V1a receptors in vascular smooth muscle → vasoconstriction.
Renal Handling of Sodium and Water: Pathophysiological Basis
The kidneys filter approximately 180 litres of water and 25,000 mmol of sodium daily; less than 1% of each is excreted in urine under normal conditions, reflecting an extraordinarily efficient tubular reabsorption system. Understanding which segment handles what proportion of the filtered load explains why diuretics acting at different nephron sites differ so dramatically in potency.
The proximal convoluted tubule reabsorbs approximately 65–70% of filtered sodium (predominantly via the Na-H antiporter, fuelled by carbonic anhydrase activity) and water isosmotically. The thick ascending limb (TAL) of the loop of Henle reabsorbs about 25% of filtered NaCl via NKCC2, but is impermeable to water — this is where the hyperosmotic medullary gradient is generated. The distal convoluted tubule reabsorbs a further 5–10% via NCC. The collecting duct (~2–5% of Na) is regulated by aldosterone (Na reabsorption via ENaC) and ADH (water reabsorption via aquaporin-2).
Oedema forms when total body sodium is expanded beyond the capacity of the interstitium to maintain the oncotic–hydrostatic balance — most commonly in heart failure (low cardiac output → neurohormonal activation → RAAS + ADH stimulation → sodium and water retention), cirrhosis (splanchnic vasodilation → same neurohormonal cascade), and nephrotic syndrome (hypoalbuminaemia → ↓oncotic pressure). In hypertension, increased extracellular volume expansion contributes to sustained elevated blood pressure. Diuretics correct these states by blocking the Na-transport proteins that maintain abnormal retention.
The degree of diuresis depends on the fraction of filtered sodium delivered to the drug's target segment: loop diuretics act on the TAL (which handles 25% of filtrate) and are therefore far more potent than thiazides (DCT, 5–10%) — which explains why loop diuretics are preferred in severe oedema and cardiac emergencies.
Diuretic Sites of Action in the Nephron
Therapeutic Goals: When and Why We Use Diuretics
The therapeutic goal of diuretics varies by indication. In oedematous states (heart failure, cirrhosis, nephrotic syndrome), the goal is to reduce extracellular fluid volume, relieving dyspnoea, ascites, or peripheral oedema, while avoiding excessive volume depletion or electrolyte disturbances. In hypertension, thiazide diuretics act initially by reducing plasma volume (short-term) and subsequently by reducing peripheral vascular resistance (long-term mechanism); the goal is sustained blood pressure control below target with minimal metabolic impact. In acute pulmonary oedema, loop diuretics delivered IV provide both venodilatation (vasodilator effect within 5 minutes) and subsequently diuresis — relieving dangerous hypoxaemia. In raised intracranial pressure (cerebral oedema), osmotic diuretics (mannitol) create an osmotic gradient that draws water from brain tissue to plasma.
Indication-to-class matching:
- Acute pulmonary oedema, severe cardiac failure → IV loop diuretic (furosemide)
- Hypertension (without oedema) → thiazide (chlorthalidone, HCTZ, indapamide)
- Chronic heart failure (HFrEF) maintenance → oral loop ± potassium-sparing
- Cirrhotic ascites → spironolactone first-line (aldosterone-driven sodium retention)
- Cerebral/spinal cord oedema → mannitol IV (osmotic)
- Glaucoma → acetazolamide (carbonic anhydrase inhibitor reduces aqueous humour)
- Altitude sickness → acetazolamide (reduces CSF production + metabolic acidosis stimulus to breathe)
- Hypercalcaemia → IV saline + furosemide (loop diuretic increases Ca excretion)
- Calcium-containing renal stones → thiazides (reduce urinary Ca excretion)
- SIADH/hyponatraemia (euvolaemic) → vaptan (tolvaptan) — free water excretion without Na loss
Classification of Diuretics by Site of Action
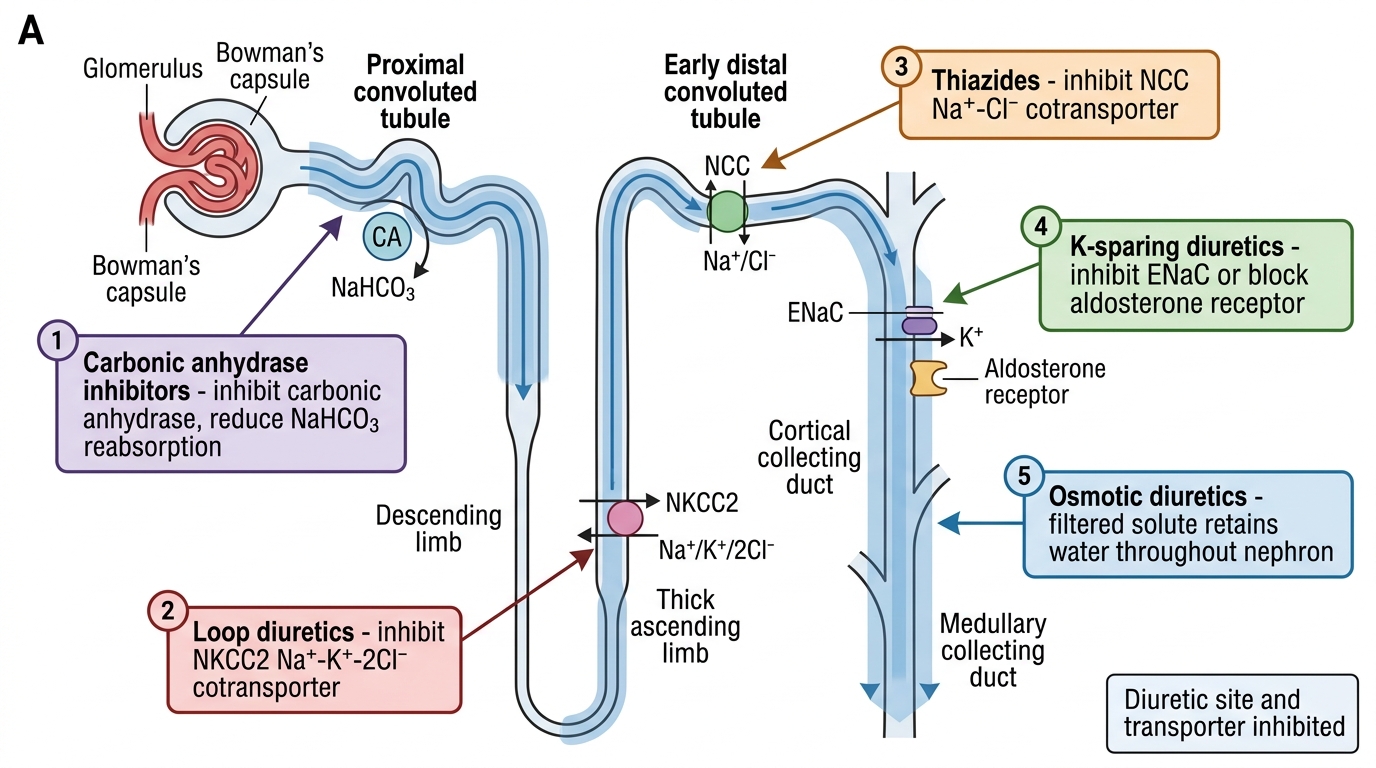
Diuretics are most logically classified by their primary site of action in the nephron, which directly determines their potency and electrolyte profile. The five established classes, in anatomical order from proximal to distal, are:
Provided image
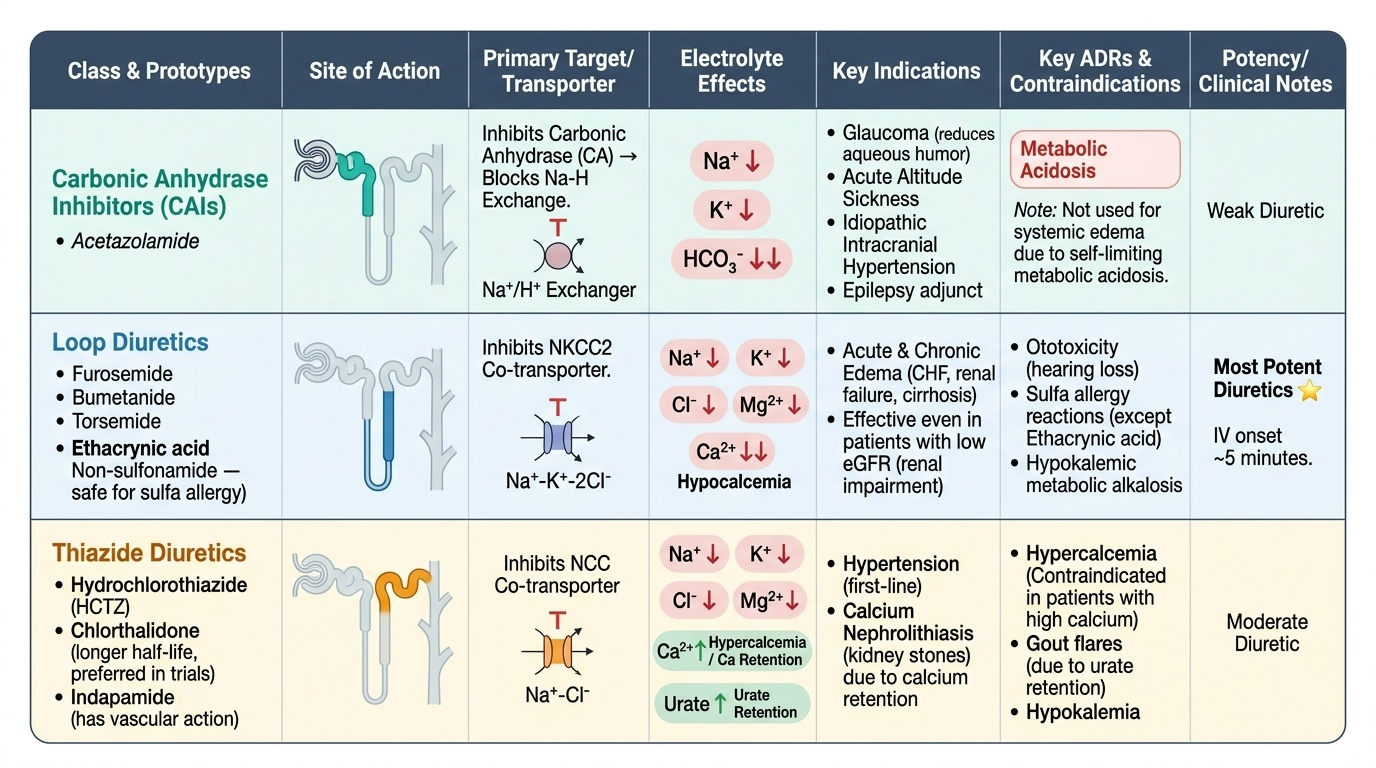
1. Carbonic anhydrase inhibitors (CAIs) — Proximal tubule. Prototype: acetazolamide. Inhibit CA → block Na-H exchange → lose Na, K, bicarbonate in urine → metabolic acidosis → weak diuresis. Used primarily for glaucoma, altitude sickness, idiopathic intracranial hypertension, and epilepsy adjunct. Not used for oedema (metabolic acidosis limits effect).
2. Loop diuretics — Thick ascending limb (TAL). Prototypes: furosemide (most widely used), bumetanide, torsemide, ethacrynic acid (only non-sulfonamide loop, used in sulfa allergy). Inhibit NKCC2 → lose Na, K, Cl, Mg, and Ca (hypocalcaemia). Most potent diuretics. Effective even in low eGFR. IV onset ~5 minutes.
3. Thiazide diuretics — Early distal convoluted tubule. Prototypes: hydrochlorothiazide (HCTZ), chlorthalidone (longer half-life, preferred in hypertension trials), indapamide (some vascular action). Inhibit NCC → lose Na, K, Cl, Mg, urate; importantly retain Ca (hypercalcaemia) — useful in Ca-stone disease; contraindicated in hypercalcaemia. Moderate potency. Ineffective when eGFR <30 mL/min/1.73m² (except metolazone, indapamide).
4. Potassium-sparing diuretics — Cortical collecting duct. Two subgroups:
- Aldosterone (MR) antagonists: spironolactone, eplerenone — block MR → ↓ENaC + ↓Na-K-ATPase → retain K, lose Na. ADR: hyperkalaemia; spironolactone also causes gynaecomastia (anti-androgenic) — eplerenone is more selective.
- ENaC blockers: amiloride, triamterene — block ENaC directly, not via MR. Retain K. Used as combination with thiazide/loop to prevent hypokalaemia.
5. Osmotic diuretics — Acts throughout the nephron. Prototype: mannitol. Freely filtered, not reabsorbed, exerts osmotic pressure preventing water reabsorption throughout the nephron. Increases urine volume, Na, and water excretion. Used IV for: raised ICP (cerebral oedema), acute oliguric renal failure (to convert to non-oliguric), haemolysis/myoglobinuria (flush kidneys). Contraindicated in pulmonary oedema (expands plasma volume transiently before diuresis).
SELF-CHECK
A patient with hypertension and recurrent calcium oxalate kidney stones is being started on antihypertensive therapy. Which diuretic class is most appropriate?
A. Loop diuretics (furosemide)
B. Carbonic anhydrase inhibitors (acetazolamide)
C. Thiazide diuretics (hydrochlorothiazide)
D. Osmotic diuretics (mannitol)
Reveal Answer
Answer: C. Thiazide diuretics (hydrochlorothiazide)
Thiazide diuretics reduce urinary calcium excretion (they cause hypercalcaemia by increasing calcium reabsorption in the DCT). This makes them the preferred diuretic for patients with calcium-containing renal stones, as lowering urinary calcium reduces stone formation. They also treat hypertension. Loop diuretics do the opposite — they increase calcium excretion (hypocalcaemia) and are used for hypercalcaemia. Mannitol is an osmotic diuretic not used for hypertension or stones.