Page 5 of 13
PH5.2 | PH5.2 | Cough Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Distinguish dry (non-productive) from productive cough and explain why this distinction determines pharmacotherapy choice
- Describe the mechanism of action, pharmacokinetics, adverse drug reactions, and contraindications of major antitussives (opioid and non-opioid, central and peripheral)
- Describe the mechanism of action, uses, and adverse effects of expectorants and mucolytics
- Apply a rational prescribing algorithm for cough management in common clinical scenarios, including special populations
- Identify clinically important drug interactions involving antitussives (particularly dextromethorphan)
INSTRUCTIONS
Cough is the most common presenting complaint in primary care, and choosing between an antitussive and an expectorant — or recognising that the underlying cause needs treatment — is one of the most frequent rational-pharmacotherapy decisions a practitioner makes. This module builds on your understanding of respiratory physiology and the opioid pharmacology you encountered in earlier PH modules. By the end, you will be able to apply a drug-class taxonomy confidently, avoid high-stakes contraindications, and counsel patients in the outpatient setting.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed. Jaypee Brothers; 2019. Ch 16 (Drugs acting on respiratory tract). (textbook)
- Brunton LL, Knollmann BC (eds). Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. McGraw-Hill; 2018. Ch 36 (Pulmonary pharmacology). (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 34-year-old teacher presents with a 5-day history of dry, non-productive cough that is disrupting her sleep and her classroom voice. She has no fever, no sputum, and her chest is clear. Her partner bought her an over-the-counter 'cough syrup' that contains guaifenesin — but her cough has not improved. She now asks whether she should also take the codeine-containing linctus her neighbour recommended. What is the pharmacological basis for choosing between these agents, and what safety concern do you need to address before prescribing?
WHY THIS MATTERS
Cough accounts for more primary-care consultations than any other single symptom. The rational prescriber must answer two questions before reaching for a drug: Is this cough dry or productive? and Is there a treatable underlying cause? These two questions determine whether a drug that suppresses the cough reflex (an antitussive) is appropriate, or whether a drug that facilitates secretion clearance (an expectorant or mucolytic) is needed instead. Prescribing an antitussive for a productive cough actively suppresses the clearance of infective or inflammatory secretions — a potentially harmful choice. This module gives you the pharmacological framework to answer both questions and to avoid the most common — and potentially dangerous — prescribing errors.
RECALL
Before exploring cough pharmacotherapy, recall these foundations:
- Cough reflex arc (from respiratory physiology): Sensory limb — vagal afferents (rapidly adapting receptors in the larynx and large airways; C-fibres in smaller airways) → medullary cough centre → motor limb (expiratory muscles + glottic closure for the explosive expulsion phase). Understanding where each drug acts requires knowing this arc.
- Opioid receptors and respiratory depression (from PH opioid module): μ-opioid receptors in the medulla mediate both analgesia and respiratory depression; cough suppression occurs at a distinct medullary site at sub-analgesic doses for some opioids. Codeine's opioid effects depend on CYP2D6-mediated conversion to morphine — a critical pharmacogenomics point.
- Mucus composition (from Biochemistry): Respiratory mucus is a viscoelastic gel of glycoproteins (mucins) cross-linked by disulfide bonds. Mucolytics break these bonds to reduce viscosity. Water is the most important 'expectorant' — adequate hydration is always co-prescribed.
- First-generation antihistamines (from PH5.1 / autonomic pharmacology): Older antihistamines (chlorphenamine, diphenhydramine) cross the blood-brain barrier, causing sedation and anticholinergic effects. They also reduce mucus production — useful in post-nasal drip cough, but not in productive lower-airway cough.
Pathophysiology of Cough: The Reflex Arc and Its Triggers
Cough is a protective airway reflex that expels foreign material, pathogens, and accumulated secretions from the tracheobronchial tree. Understanding its neural substrate is the key to understanding why different drugs work at different points in the reflex arc.
The sensory limb originates at rapidly adapting receptors (RARs) in the larynx, trachea, and major bronchi, and C-fibre nociceptors distributed throughout the smaller airways and alveoli. These are innervated by the vagus nerve (predominantly) and, at the laryngeal level, the superior laryngeal nerve. Physical stimuli (foreign bodies, cold air) preferentially activate RARs; chemical stimuli (capsaicin, acid, inflammatory mediators such as bradykinin and prostaglandins) activate C-fibres. Both converge on the nucleus tractus solitarius (NTS) and are then integrated in the cough centre — a distributed medullary network also involving the periaqueductal grey. The motor limb involves co-ordinated activity of the diaphragm, intercostal muscles, and glottic closure to generate the explosive expiratory pressure that clears the airway.
The most clinically important distinction is between dry (non-productive) cough and productive (moist) cough:
- Dry cough arises from irritation of the upper or lower airway without excess secretion — common causes include post-viral irritation, ACE-inhibitor-induced bradykinin accumulation (a Class-effect of all ACE inhibitors; occurs in up to 20% of patients), post-nasal drip (rhinitis, sinusitis), gastro-oesophageal reflux disease (GERD — acid reaching the larynx activates C-fibres), and early asthma (cough-variant asthma). In dry cough, the reflex is not clearing secretions — it is a maladaptive irritant response. Suppression is appropriate.
- Productive cough arises when excess secretions accumulate in the airways (infection, bronchiectasis, COPD exacerbation, pulmonary oedema). Here the cough reflex is performing its protective function. Suppressing it with an antitussive would prevent secretion clearance and risk mucus plugging, secondary infection, and worsening hypoxaemia. Suppression is contraindicated; facilitating clearance is the goal.
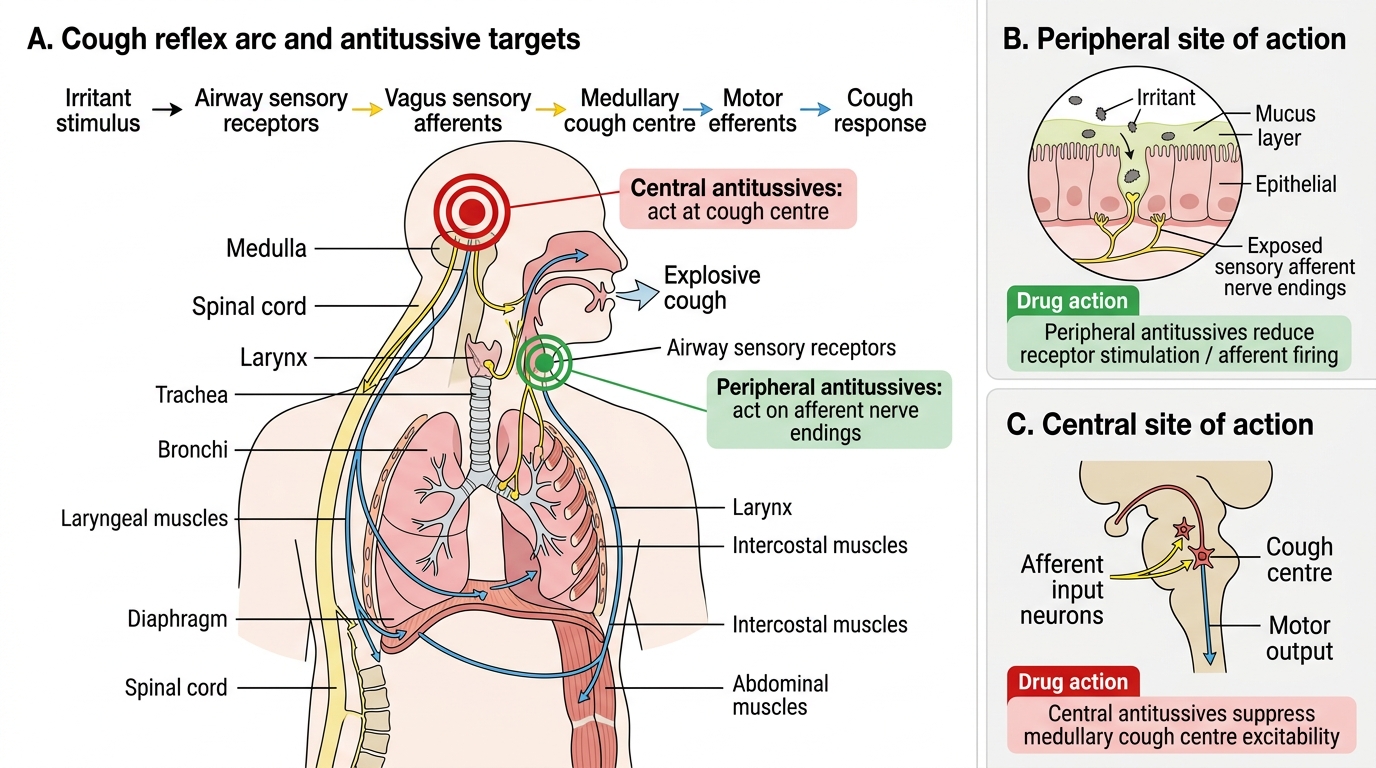
Cough Reflex Arc and Sites of Antitussive Action
A third category, chronic cough (duration >8 weeks), almost always has an identifiable cause (the 'three common causes' triad: post-nasal drip, GERD, and cough-variant asthma account for over 90% of cases in non-smokers without abnormal chest X-ray). Treating the underlying cause is always preferable to indefinite symptom suppression.
Therapeutic Goals in Cough Management
The therapeutic goal in cough management is not reflexive suppression — it is rational, context-matched intervention. The prescriber must identify which of three goals is primary before selecting a drug.
Goal 1: Suppress an unproductive cough (dry cough — where the reflex is maladaptive). The aim is to reduce cough frequency and severity enough to allow sleep, prevent glottic trauma, and restore quality of life, without suppressing normal mucociliary clearance. This is the appropriate use-case for antitussives.
Goal 2: Facilitate secretion clearance (productive cough — where the reflex is protective). The aim is to reduce mucus viscosity and/or increase ciliary transport to make expectoration easier and to support the cough reflex, not abolish it. Antitussives are actively harmful here. Expectorants, mucolytics, adequate hydration, and physiotherapy (chest percussion) serve this goal.
Goal 3: Treat the underlying cause. This is always the most important goal and often renders symptomatic therapy unnecessary:
- ACE-inhibitor cough → switch to an angiotensin receptor blocker (ARB, e.g. losartan); the ARB class does not cause bradykinin accumulation. No cough suppressant is needed — cough resolves within 1-4 weeks of stopping the ACE inhibitor.
- GERD-induced cough → proton-pump inhibitor (PPI) or H₂-blocker; the cough resolves as reflux is controlled (over weeks to months).
- Post-nasal drip / allergic rhinitis → intranasal corticosteroid (INCS) ± first-generation antihistamine (anticholinergic effect reduces secretions); first-generation agents preferred over non-sedating antihistamines for this indication because the anticholinergic and mild drying effect is therapeutic here.
- Cough-variant asthma → inhaled corticosteroid ± short-acting β₂ agonist; cough is the sole or dominant asthma symptom and does not respond to antitussives.
- Infective bronchitis / URTI → supportive care; antibiotics rarely indicated; cough typically resolves within 3 weeks.
Recognising cause-directed therapy prevents the common error of prescribing indefinite antitussive treatment for a cough that has a simple, reversible cause.
Drug Classification for Cough Management
The pharmacotherapy of cough is organised around two primary treatment branches, determined by the type of cough, plus a set of supporting agents used for specific causes.
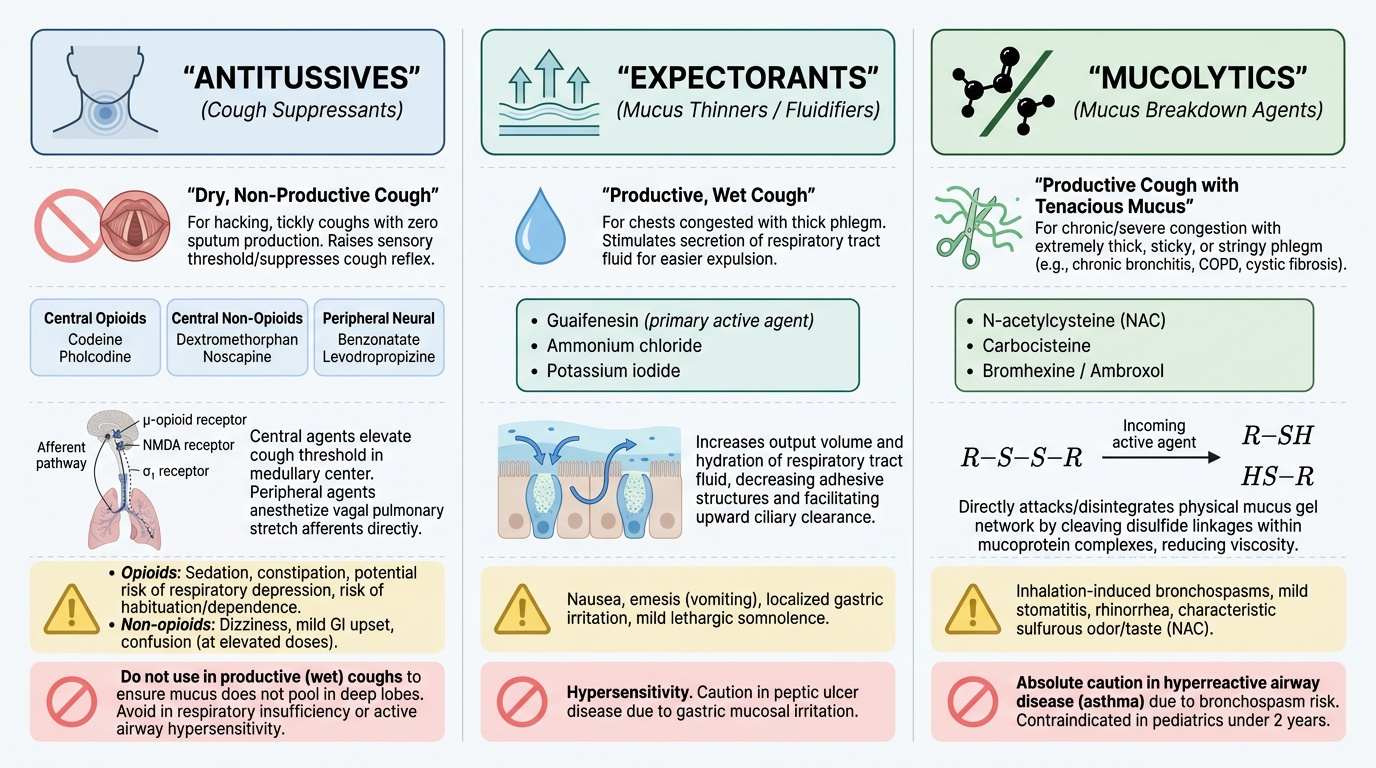
Branch 1: Antitussives — for dry (non-productive) cough only. These agents suppress the cough reflex at either the central cough centre in the medulla or the peripheral sensory afferents. They are subdivided into:
- Central antitussives — opioid: codeine, pholcodine (act at μ-opioid receptors in the medullary cough centre)
- Central antitussives — non-opioid: dextromethorphan (NMDA receptor antagonist + sigma-1 agonist; not an opioid at antitussive doses), noscapine (benzylisoquinoline alkaloid)
- Peripheral antitussives: benzonatate (local anaesthetic action on vagal afferents), levodropropizine (peripheral opioid-like receptor action; no CNS effects)
Branch 2: Expectorants and mucolytics — for productive cough only. These agents reduce the viscosity of airway secretions or stimulate their clearance:
- Expectorants: guaifenesin, ammonium chloride, potassium iodide (increase bronchial secretion volume and reduce apparent viscosity by dilution/reflex secretion)
- Mucolytics (disulfide-bond cleaving): NAC (N-acetylcysteine), carbocisteine (cleave mucin disulfide bonds directly)
- Mucolytics (mucokinetic): bromhexine and its active metabolite ambroxol (stimulate serous gland secretion, reduce goblet-cell mucus viscosity; ambroxol also has surfactant-stimulating properties), erdosteine (inactive prodrug converted to active thiol metabolite)
Supporting/adjunctive agents:
- Demulcents: honey, glycerol, simple linctus — coat and soothe inflamed mucosa; WHO-recommended for children aged 1–5 years with cough from URTI (preferred over pharmacological agents in this age group)
- First-generation antihistamines: useful only in post-nasal drip cough (anticholinergic/drying effect); not for lower-airway productive cough
- Adequate hydration — the single most important measure for productive cough; always advise alongside any mucolytic or expectorant
A critical prescribing rule that cannot be over-emphasised: antitussives are absolutely contraindicated in productive cough — their use suppresses the clearance of potentially infective or inflammatory secretions and can cause mucus plugging, atelectasis, and secondary pneumonia.
Provided image
SELF-CHECK
A 68-year-old patient with COPD presents with increased cough and purulent yellow sputum. Which is the most appropriate pharmacological intervention?
A. Codeine linctus 10 mg three times daily
B. Dextromethorphan 15 mg three times daily
C. Bromhexine 8 mg three times daily plus adequate hydration
D. Benzonatate 100 mg three times daily
Reveal Answer
Answer: C. Bromhexine 8 mg three times daily plus adequate hydration
This patient has a productive cough with purulent sputum — a classic indication for a mucolytic/expectorant approach, not an antitussive. Bromhexine (a mucokinetic mucolytic) reduces mucus viscosity and facilitates expectoration. Codeine, dextromethorphan, and benzonatate are all antitussives, and all are contraindicated in productive cough. Adequate hydration must always accompany mucolytic therapy.