Page 1 of 18
PH2.{1,3} | PH2.{1,3} | Adrenergic Drugs and Emergency Sympathomimetic Use — SDL Guide — SDL Guide
Learning Objectives
- Describe the types, pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of adrenergic and antiadrenergic drugs (PH2.1)
- Explain the rationale for and demonstrate the emergency use of sympathomimetic and parasympatholytic drug agonists/antagonists (adrenaline, noradrenaline, dopamine, dobutamine, atropine) in case-based scenarios (PH2.3)
INSTRUCTIONS
The adrenergic nervous system is the pharmacological substrate for managing life-threatening emergencies: anaphylaxis, cardiac arrest, septic shock, and acute heart failure all require you to select the correct catecholamine or adrenergic agent, dial in the right dose and route, and understand why it works. This guide takes you from receptor physiology through drug classification to bedside decision-making, giving you the pharmacological framework that underpins ACLS, ICU vasopressor protocols, and anaesthetic emergency drills.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed., Ch 9-10 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 12-13 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman develops urticaria, throat tightness, and hypotension (BP 70/40 mmHg) within minutes of her first dose of amoxicillin in the outpatient clinic. The nurse hands you a vial labelled 'Adrenaline 1 mg/mL (1:1000).' You need to act in the next 90 seconds. What dose? Which route? Which muscle? And why does getting this pharmacology right mean the difference between a full recovery and a preventable death?
WHY THIS MATTERS
Adrenergic pharmacology is not a topic you learn once and forget — it is the engine driving emergency medicine, intensive care, and perioperative practice. Adrenaline reverses anaphylaxis by simultaneously dilating airways, constricting skin vasculature, and supporting cardiac output. Noradrenaline keeps perfusion pressure in septic shock when the vasculature has collapsed. Dopamine and dobutamine calibrate cardiac output in cardiogenic states. Beta-blockers dominate the management of hypertension, angina, and post-MI care. Understanding these drugs at the receptor level lets you predict effects, anticipate adverse reactions, and adapt doses to clinical reality — skills the OSCE examiners and ICU attendings will test directly.
RECALL
Before we classify adrenergic drugs, ground yourself in the Year-1 physiology you already know. The sympathetic nervous system releases noradrenaline (norepinephrine) at postganglionic synapses and adrenaline (epinephrine) from the adrenal medulla. These catecholamines bind to four main receptor families: α1 (Gq-coupled; vascular smooth muscle contraction, mydriasis, urethral sphincter tone), α2 (Gi-coupled; presynaptic inhibition of NA release, platelet aggregation, reduced insulin secretion), β1 (Gs-coupled; cardiac chronotropy and inotropy, renin release), and β2 (Gs-coupled; bronchodilation, uterine relaxation, glycogenolysis). β3 receptors mediate lipolysis in adipose tissue and bladder relaxation. Dopamine receptors (D1/D2) are present in renal, mesenteric, and splanchnic vasculature, mediating vasodilation at low concentrations. This receptor map is the Rosetta Stone for predicting what every adrenergic drug will do.
Pathophysiology of Sympathetic Activation and Adrenergic Receptors
The adrenergic system is activated by stress, haemorrhage, hypoglycaemia, or threat — the classic 'fight-or-flight' response. Catecholamines are synthesised from tyrosine via a four-step pathway: tyrosine → DOPA (tyrosine hydroxylase, rate-limiting) → dopamine → noradrenaline → adrenaline (phenylethanolamine N-methyltransferase, in adrenal medulla only). Released catecholamines interact with adrenoceptors on target cells, producing effects that are entirely predictable once you know which receptor family is engaged.
The receptor landscape in clinical practice:
- α1 receptors: smooth muscle of blood vessels (vasoconstriction → ↑BP), iris dilator, sphincters. Gq → IP3/DAG → intracellular Ca²⁺ → contraction.
- α2 receptors: presynaptic nerve terminals (autoreceptors: ↓NA release = negative feedback); postsynaptic in CNS and platelets.
- β1 receptors: heart (↑HR, ↑force), kidney juxtaglomerular cells (↑renin). Gs → adenylyl cyclase → ↑cAMP → PKA.
- β2 receptors: bronchial smooth muscle (relaxation → bronchodilation), uterus (relaxation), vascular smooth muscle of skeletal muscle (vasodilation), liver (glycogenolysis).
- β3 receptors: adipose tissue (lipolysis), detrusor muscle (relaxation).
- D1/D2 receptors: renal + splanchnic vasculature (vasodilation at low dopamine concentrations).
The baroreceptor reflex is a critical modulator: when a drug raises BP via α1 stimulation (e.g. phenylephrine), baroreceptors fire → parasympathetic surge → reflex bradycardia. This predictable reflex is why phenylephrine must be given with awareness of its heart-rate lowering effect.
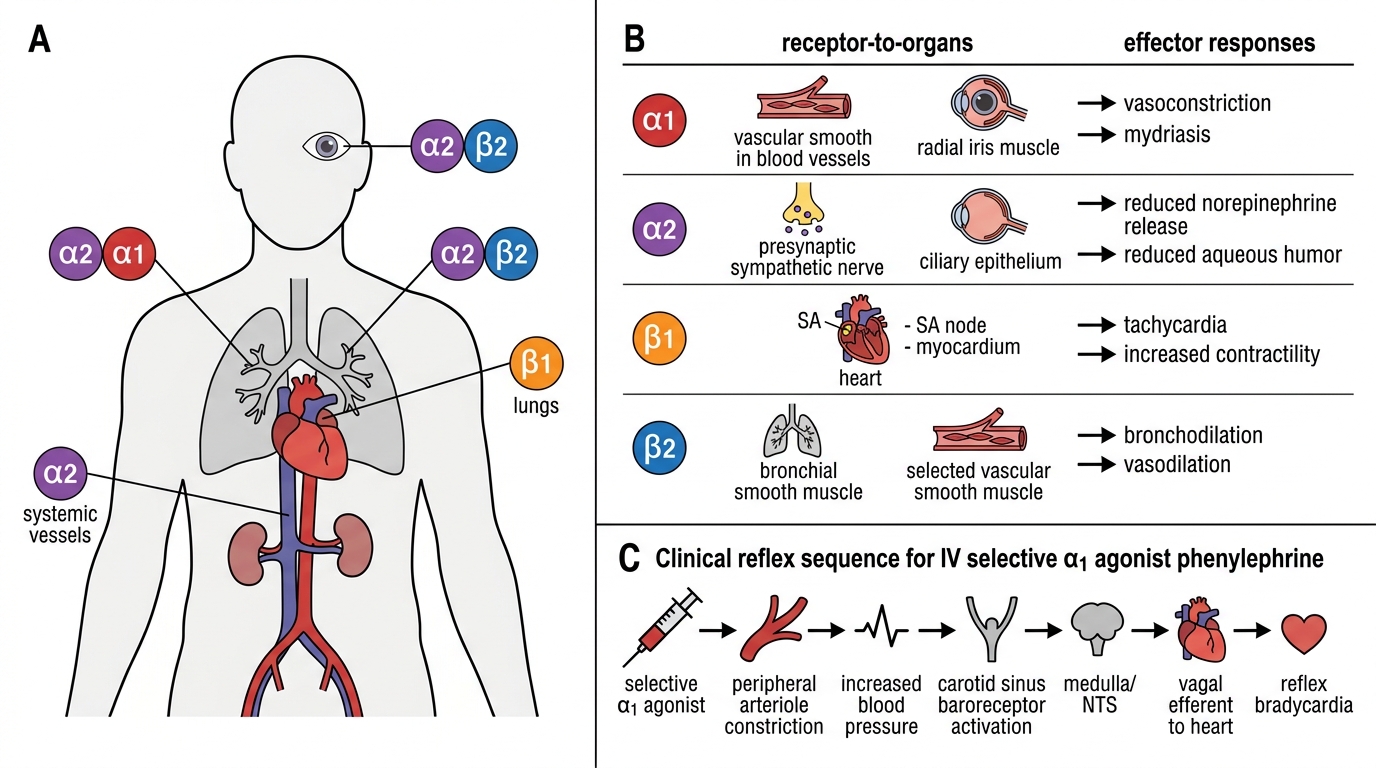
Adrenergic Receptor Subtypes: Locations and Effector Responses
SELF-CHECK
A selective α1 agonist is administered intravenously. Which reflex cardiovascular response do you expect, and via which receptor?
A. Tachycardia via β1 receptor stimulation
B. Bradycardia via baroreceptor-mediated vagal surge
C. No heart rate change; α1 is cardiac-only
D. Tachycardia via α2 presynaptic disinhibition
Reveal Answer
Answer: B. Bradycardia via baroreceptor-mediated vagal surge
A selective α1 agonist (e.g. phenylephrine) causes peripheral vasoconstriction → ↑BP → baroreceptors detect the rise → afferent signals to NTS → parasympathetic (vagal) efferents → ↓HR. This reflex bradycardia is a vasovagal response, not a direct drug effect on cardiac β1 receptors.
Therapeutic Rationale for Adrenergic Drug Therapy
The fundamental rationale for manipulating the adrenergic system is to restore or re-calibrate the physiological variables that sustain tissue perfusion and organ function. In critical illness, the normal sympathetic compensatory response is either inadequate (septic shock — vasodilation overwhelms the reflex) or pathologically excessive (hypertensive crisis — sympathetic hyperactivation). Understanding which physiological defect is present determines which receptor targets are engaged and which drugs are chosen.
Key therapeutic goals mapped to receptor targets:
- Restore perfusion pressure (septic/distributive shock): noradrenaline (α1 + β1) is first-line — raises SVR and provides modest inotropy without the excessive chronotropy of adrenaline.
- Treat anaphylaxis (bronchospasm + vasodilation + urticaria): adrenaline is uniquely indicated — β2 dilates bronchi, α1 constricts cutaneous vasculature, β1 supports cardiac output. No other drug addresses all three pathways simultaneously.
- Support cardiac output (acute decompensated heart failure): dobutamine (selective β1) increases contractility without major vasoconstriction; dopamine at low doses adds D1-mediated renal vasodilation.
- Control bronchospasm (asthma/COPD): salbutamol (β2 agonist) relaxes bronchial smooth muscle with minimal β1 cardiac effects (at therapeutic doses).
- Lower BP (hypertension, angina, post-MI): beta-blockers (β1 blockade → ↓HR, ↓CO, ↓renin) and alpha-blockers (α1 blockade → ↓SVR).
- Manage phaeochromocytoma (catecholamine excess): phenoxybenzamine (irreversible α-blocker) pre-operatively, then beta-blockers only after alpha-blockade (beta first → unopposed α1 → hypertensive crisis).
The key discipline: always match the receptor to the physiological defect. Using a non-selective agonist when a selective one would suffice risks unwanted receptor activation and predictable adverse effects.
Classification of Adrenergic Drugs
Adrenergic drugs are classified at two levels: first by their primary action (agonist vs antagonist), then by their receptor selectivity and mechanism. Understanding this taxonomy is essential for predicting the pharmacological profile of any agent in the class.
Class 1: Adrenergic Agonists (Sympathomimetics)
Agonists mimic or enhance sympathetic activity. They are further divided by mechanism:
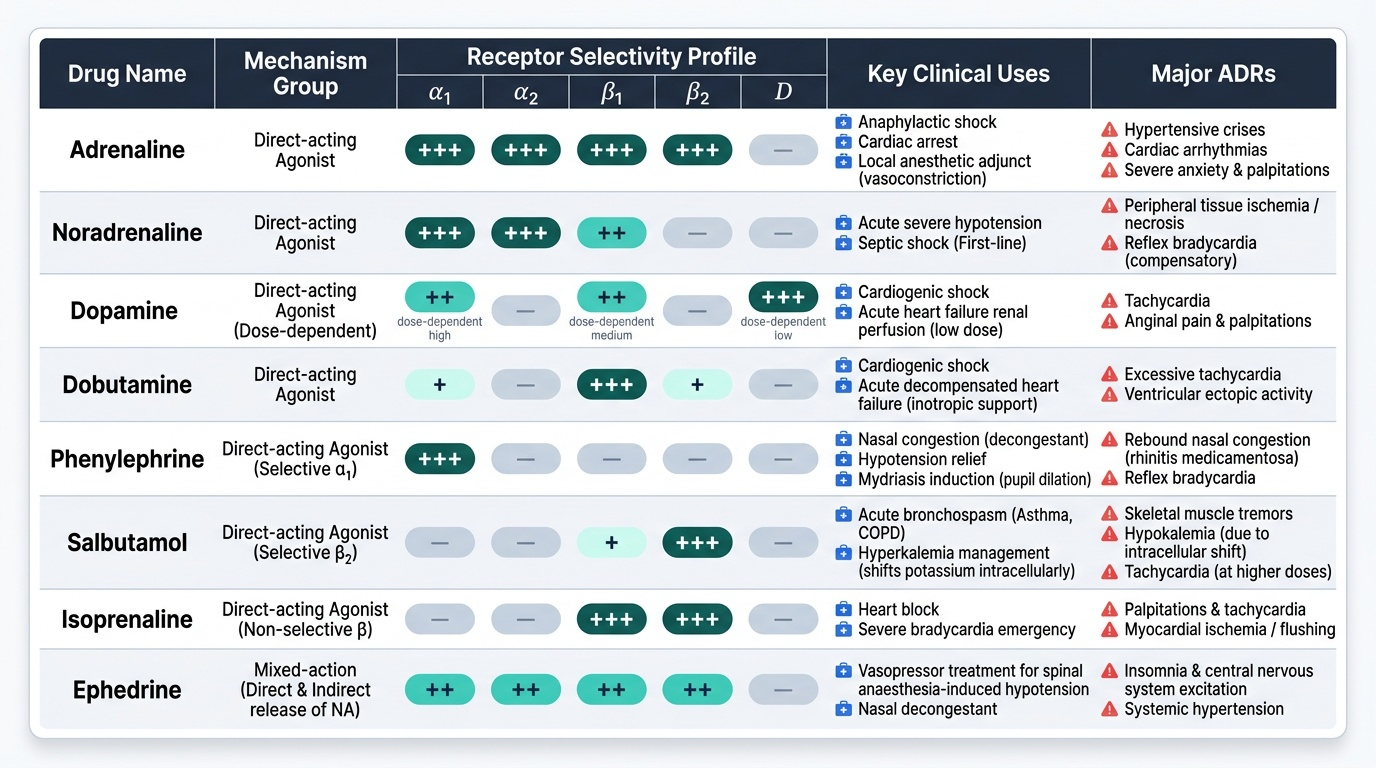
- Direct-acting: bind adrenoceptors directly. Examples: adrenaline (non-selective), noradrenaline (α1/α2/β1), dopamine (dose-dependent), dobutamine (selective β1), phenylephrine (selective α1), salbutamol (selective β2), isoprenaline (non-selective β).
- Indirect-acting: promote NA release from nerve terminals or inhibit NA reuptake (no direct receptor binding). Examples: amphetamine, tyramine.
- Mixed action: both direct receptor binding and NA release. Example: ephedrine — clinically relevant as a vasopressor in spinal anaesthesia-induced hypotension.
Class 2: Adrenergic Antagonists (Sympatholytics)
Antagonists block adrenoceptors. Classified by receptor subtype:
- Alpha-blockers:
- Non-selective irreversible: phenoxybenzamine (covalent bond → 24h block → used in phaeochromocytoma prep)
- Non-selective reversible: phentolamine (used in phaeochromocytoma crisis, IV)
- Selective α1: prazosin, terazosin, doxazosin (used in hypertension, BPH — first-dose hypotension is a key adverse effect)
- Beta-blockers:
- Non-selective (β1+β2): propranolol — avoid in asthma (β2 blockade → bronchoconstriction)
- Selective β1 (cardioselective): atenolol, metoprolol, bisoprolol — preferred in patients with reactive airway disease
- Mixed α + β blocker: carvedilol, labetalol — carvedilol used in HFrEF (reduces mortality); labetalol preferred in hypertensive emergencies in pregnancy
Provided image
SELF-CHECK
A patient with phaeochromocytoma requires surgical resection. The pre-operative preparation begins with phenoxybenzamine. Why must alpha-blockade be established BEFORE any beta-blocker is given?
A. Beta-blockers increase catecholamine secretion from the tumour
B. Without alpha-blockade, beta-blockade removes the vasodilatory β2 check and leaves α1-mediated vasoconstriction unopposed, precipitating a hypertensive crisis
C. Phenoxybenzamine is a beta-blocker itself and must load the receptors first
D. Alpha-blockade prevents reflex tachycardia that would be exacerbated by beta-blockers
Reveal Answer
Answer: B. Without alpha-blockade, beta-blockade removes the vasodilatory β2 check and leaves α1-mediated vasoconstriction unopposed, precipitating a hypertensive crisis
In phaeochromocytoma, tumour catecholamines activate both α (vasoconstriction) and β2 (vasodilation, as well as β1 tachycardia) receptors. If a beta-blocker is given first, β2-mediated vasodilation is lost while α1 remains fully active — the result is severe unopposed vasoconstriction and a dangerous hypertensive crisis. Alpha-blockade first neutralises the α1 vasoconstriction; beta-blockers are then added to control tachycardia safely.