Page 2 of 18
PH2.{1,3} | PH2.{1,3} | Adrenergic Drugs and Emergency Sympathomimetic Use — SDL Guide — SDL Guide (Part 2)
Adrenergic Agonists — PK, PD, Uses, and Adverse Effects
Adrenergic agonists are among the most pharmacokinetically constrained drugs in the formulary: most catecholamines (adrenaline, noradrenaline, dopamine, dobutamine) are polar, cannot cross the blood-brain barrier, undergo extensive first-pass O-methylation (COMT) and oxidative deamination (MAO), and have plasma half-lives of 1–3 minutes. This mandates IV infusion for systemic emergency use. Exceptions: salbutamol is inhaled for local bronchial effect (oral bioavailability is limited); ephedrine and pseudoephedrine are orally effective (non-catecholamine structure, not MAO/COMT substrates).
| Drug | Receptor profile | Key uses | Major ADRs | Key cautions |
|---|---|---|---|---|
| Adrenaline | α1, α2, β1, β2, β3 (all) | Anaphylaxis (IM), cardiac arrest (IV), severe asthma (IM/SC) | Palpitations, hypertension, arrhythmia, anxiety, tremor, ischaemia | Halothane anaesthesia (sensitises myocardium → VF); narrow-angle glaucoma |
| Noradrenaline | α1, α2, β1 (negligible β2) | Septic shock (IV infusion), vasodilatory shock | Peripheral ischaemia (gangrene at high doses), arrhythmia, reflex bradycardia via α1-mediated BP rise | Extravasation → tissue necrosis (phentolamine antidote); hypertension |
| Dopamine | D1/D2 (low), β1 (mid), α1 (high) | Cardiogenic/distributive shock, acute HF, dopamine renal-dose (historically, now controversial) | Tachyarrhythmias, nausea, vasoconstriction at high doses | Tachycardia limits use in AF; phaeochromocytoma (avoid) |
| Dobutamine | β1 selective | Acute decompensated HF, cardiogenic shock, cardiac stress test | Tachycardia, ectopics, angina (↑O₂ demand), hypotension (β2 at high doses) | Avoid in HOCM (↑outflow tract obstruction) |
| Phenylephrine | α1 selective | Vasopressor (spinal hypotension, adjunct in shock), nasal decongestant, eye drops (mydriasis) | Reflex bradycardia, hypertension, peripheral ischaemia | Low cardiac output states (↑afterload → worse) |
| Salbutamol | β2 selective | Asthma/COPD (inhaled), hyperkalaemia (IV), tocolysis (IV) | Tremor, palpitations, hypokalaemia (β2 → K⁺ into cells), headache | Cardiac disease (tachycardia) |
| Ephedrine | Mixed α + β (indirect + direct) | Spinal anaesthesia hypotension (IV), bronchospasm (oral, now restricted) | Insomnia, hypertension, tachycardia, urinary retention | MAO inhibitors (hypertensive crisis); repeated use → tachyphylaxis |
Key PD principle: receptor selectivity is dose-dependent. Dopamine acts on D1 at 1–3 mcg/kg/min, β1 at 3–10 mcg/kg/min, and α1 at >10 mcg/kg/min. Even 'selective' agents lose selectivity at supratherapeutic doses — salbutamol at very high IV doses activates β1 (tachycardia).
Adrenergic Antagonists — Alpha and Beta Blockers
Adrenergic antagonists block catecholamine access to adrenoceptors. Their clinical utility derives from removing pathological sympathetic tone — in hypertension, ischaemic heart disease, heart failure, and phaeochromocytoma. Pharmacokinetically, beta-blockers as a class are well-absorbed orally, but vary in lipophilicity: lipophilic agents (propranolol, metoprolol) cross the blood-brain barrier (CNS effects — dreams, depression); hydrophilic agents (atenolol) do not. Beta-blockers are largely renally or hepatically cleared; dose adjustment is needed in renal failure for atenolol.
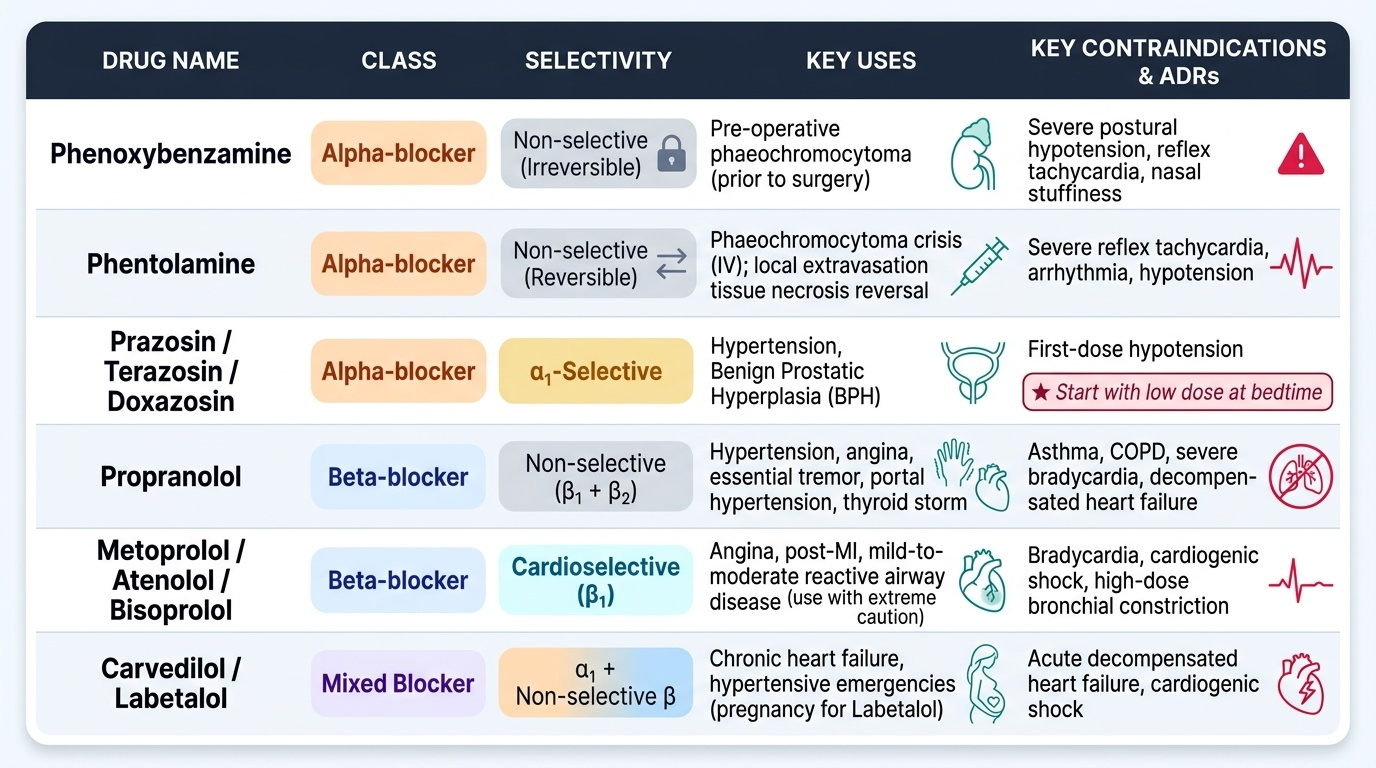
Provided image
Alpha-blockers in detail:
- Phenoxybenzamine: irreversible, non-competitive α-block (covalent alkylation). Duration 24–48 hours (requires new receptor synthesis to reverse). Used for pre-operative α-blockade in phaeochromocytoma (started 10–14 days before surgery). Major ADRs: postural hypotension (especially on first standing), reflex tachycardia, nasal stuffiness, miosis.
- Phentolamine: competitive, reversible, non-selective α-blocker. Short-acting IV drug used for phaeochromocytoma crisis (hypertensive emergency) and to reverse noradrenaline extravasation tissue necrosis (local injection). Causes reflex tachycardia (block α2 presynaptic → ↑NA release + direct β stimulation).
- Prazosin / terazosin / doxazosin: selective α1 blockade. No presynaptic α2 block → less reflex tachycardia. Uses: hypertension, benign prostatic hyperplasia (α1A in bladder neck/prostate). First-dose hypotension is a well-known class effect — always start with a low dose at bedtime.
Beta-blockers in detail:
- Propranolol: prototype non-selective β-blocker (β1 + β2). Uses: hypertension, angina, arrhythmias (supraventricular), essential tremor, portal hypertension (↓splanchnic flow), thyroid storm. Contraindicated in asthma/COPD (β2 blockade → bronchoconstriction). Also contraindicated in significant bradycardia, heart block, and decompensated HF (acute).
- Atenolol / metoprolol / bisoprolol: cardioselective β1-blockers (ISA absent in most). Preferred when beta-blockade is needed in patients with mild-to-moderate reactive airway disease (still use with caution — selectivity is relative, lost at high doses). Uses: hypertension, stable angina, post-MI, HF (bisoprolol — mortality benefit in HFrEF).
- Carvedilol: non-selective β + α1 blocker. Used in HFrEF (evidence-based: reduces all-cause mortality and hospitalisation in systolic HF — targets both β1-mediated adverse remodelling and α1-mediated vasoconstriction). Additional anti-oxidant properties. Dose must be titrated up slowly in HF (start low, go slow).
- Labetalol: α1 + β1 + β2 blocker (α:β ratio ~1:7 IV, ~1:3 oral). Used in hypertensive emergencies, particularly in pregnancy (safe profile; does not cause foetal bradycardia at standard doses unlike other beta-blockers).
Critical class effect: rebound hypertension on abrupt beta-blocker withdrawal — receptor upregulation during chronic blockade means sudden cessation causes exaggerated sympathetic response. Always taper.
SELF-CHECK
A 62-year-old with HFrEF (LVEF 30%), controlled hypertension, and mild COPD is being optimised. Which beta-blocker is most appropriate and why?
A. Propranolol — non-selective blockade achieves better BP reduction
B. Carvedilol — has evidence-based mortality benefit in HFrEF plus α1 blockade reduces afterload; use with caution given COPD (monitor airway symptoms)
C. Atenolol — cardioselective, avoids bronchoconstriction, and is first-line in HFrEF
D. No beta-blocker — beta-blockade is absolutely contraindicated in HF
Reveal Answer
Answer: B. Carvedilol — has evidence-based mortality benefit in HFrEF plus α1 blockade reduces afterload; use with caution given COPD (monitor airway symptoms)
Carvedilol (and bisoprolol, and metoprolol succinate) has Level A evidence for mortality reduction in HFrEF. Carvedilol's combined β + α1 blockade is particularly useful as it reduces both adverse remodelling and afterload. Atenolol lacks HFrEF mortality evidence (trials used carvedilol, bisoprolol, metoprolol succinate). Propranolol is non-selective — its β2 blockade is risky in COPD. Beta-blockers are NOT contraindicated in stable HF — they are guideline-mandatory in HFrEF (start at very low dose, titrate up when fluid-overload resolved).
Emergency Use of Sympathomimetic and Parasympatholytic Drugs: Case-Based Decision Making
Emergency pharmacology demands rapid, protocol-driven decision-making grounded in receptor pharmacology. The five high-yield emergency scenarios below each follow a structured decision logic: identify the physiological defect → match the receptor target → select the drug → specify dose/route/monitoring.
Scenario 1 — Anaphylaxis
Physiology: IgE-mediated mast-cell degranulation → histamine + prostaglandins → vasodilation (↓SVR → hypotension) + bronchoconstriction + urticaria/angioedema.
Drug of choice: Adrenaline (epinephrine).
- Route: intramuscular (IM), lateral thigh (vastus lateralis). IM provides faster, more reliable absorption than SC; IV only in cardiac arrest or unresponsive to IM.
- Dose: 0.5 mg (500 mcg) IM of 1:1000 solution (1 mg/mL) for adults. Children: 0.01 mg/kg IM (max 0.5 mg).
- Rationale: α1 → vasoconstriction → restores BP + reduces urticaria/angioedema; β2 → bronchodilation; β1 → ↑HR and inotropy.
- Repeat in 5–15 min if no improvement. Adjuncts: IV fluid, antihistamine, corticosteroid (slower onset, prevent biphasic).
Scenario 2 — Septic Shock
Physiology: cytokine-driven vasodilation → ↓SVR → distributive hypotension, often with preserved/elevated CO early.
First-line vasopressor: Noradrenaline (norepinephrine).
- Dose: 0.01–3 mcg/kg/min IV infusion (central line preferred; titrate to MAP ≥65 mmHg).
- Rationale: strong α1 (vasoconstriction → ↑SVR → ↑MAP) + β1 (maintains CO) with less tachyarrhythmia than adrenaline.
- Dopamine is an alternative (especially with bradycardia) but meta-analyses (SOAP-II trial) show higher arrhythmia rates; guideline recommendation is noradrenaline as first-line.
Scenario 3 — Cardiac Arrest
Protocol: adrenaline 1 mg IV (1:10,000 solution = 0.1 mg/mL) every 3–5 minutes during CPR.
Rationale: α1-mediated vasoconstriction → ↑coronary + cerebral perfusion pressure during CPR. Note: the PARAMEDIC2 RCT showed adrenaline improved return of spontaneous circulation (ROSC) but NOT survival with favourable neurological outcome at 30 days (the benefit is haemodynamic; neurological outcome depends on CPR quality and time to defibrillation).
Scenario 4 — Acute Decompensated Heart Failure (Cardiogenic Shock)
Physiology: reduced LV contractility → ↓CO → hypotension despite normal/elevated filling pressures.
Drug: Dobutamine 2.5–20 mcg/kg/min IV infusion.
Rationale: selective β1 agonism → ↑contractility → ↑CO. Some β2-mediated vasodilation at higher doses reduces afterload (beneficial). Avoid in hypovolaemia (need adequate preload). Monitor for tachycardia and ventricular ectopy.
Scenario 5 — Bradycardia and Organophosphate (OPC) Poisoning: Atropine
Atropine is a competitive muscarinic antagonist (parasympatholytic, not adrenergic), but PH2.3 explicitly requires its emergency demonstration because it antagonises the excessive cholinergic state seen in OPC poisoning and in vagally mediated bradycardia.
- Bradycardia (symptomatic sinus bradycardia / AV block): atropine 0.5–1 mg IV bolus, repeat up to 3 mg total. Mechanism: blocks M2 receptors at SA node → removes vagal brake → ↑HR.
- OPC/organophosphate poisoning: atropine 2–4 mg IV (repeated large doses — up to 20 mg or more in severe poisoning) to dry secretions and restore HR. Titrate to secretions (salivation, bronchospasm) not to tachycardia. Pair with pralidoxime (oxime to reactivate AChE — give before ageing).
| Emergency | Drug | Dose | Route | Monitoring |
|---|---|---|---|---|
| Anaphylaxis | Adrenaline | 0.5 mg (adult) | IM — lateral thigh | BP, SpO2, HR, symptoms |
| Septic shock | Noradrenaline | 0.01–3 mcg/kg/min | IV infusion (central) | MAP ≥65, urine output, lactate |
| Cardiac arrest | Adrenaline | 1 mg every 3–5 min | IV bolus | ROSC, rhythm |
| Acute HF/cardiogenic shock | Dobutamine | 2.5–20 mcg/kg/min | IV infusion | CO/CI, BP, HR, arrhythmia |
| Bradycardia | Atropine | 0.5–1 mg (up to 3 mg) | IV bolus | HR, AV conduction |
| OPC poisoning | Atropine | 2–4 mg (repeat) | IV bolus | Secretions dry, bronchospasm |
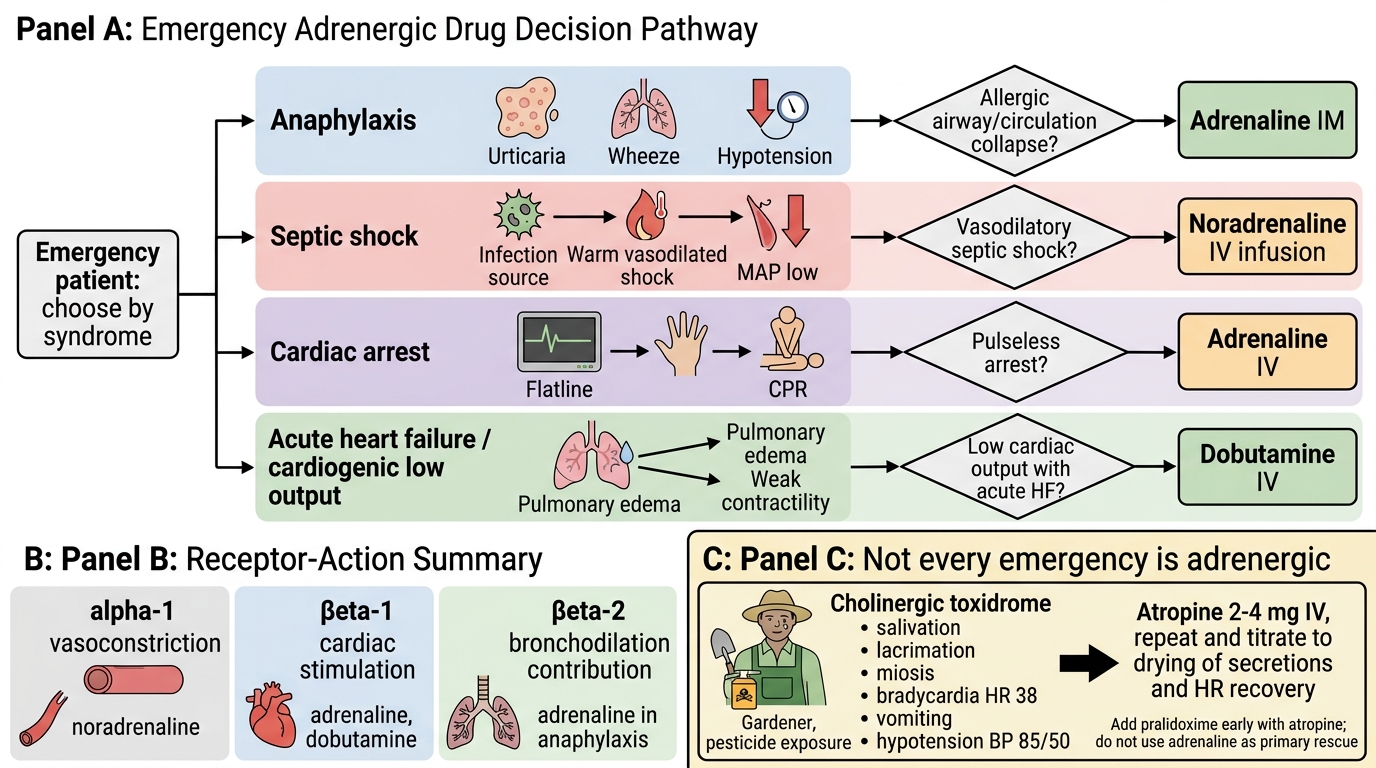
Emergency Adrenergic Drug Selection Flowchart
SELF-CHECK
A 35-year-old gardener presents with excessive salivation, lacrimation, bradycardia (HR 38), miosis, and vomiting after pesticide exposure. BP is 85/50 mmHg. Which drug is immediately indicated and at what dose?
A. Adrenaline 0.5 mg IM — anaphylaxis protocol
B. Atropine 2–4 mg IV — treat cholinergic excess; titrate to drying of secretions and restoration of HR
C. Noradrenaline infusion — correct the hypotension with a vasopressor first
D. Pralidoxime 1 g IV alone — oxime reactivates AChE without need for atropine
Reveal Answer
Answer: B. Atropine 2–4 mg IV — treat cholinergic excess; titrate to drying of secretions and restoration of HR
This is classic organophosphate/carbamate poisoning producing the cholinergic toxidrome (SLUDGE/DUMBELS: Salivation, Lacrimation, Urination, Defaecation, GI upset, Emesis; Bradycardia, Bronchospasm). Atropine blocks M1/M2/M3 muscarinic receptors, drying secretions and increasing HR. Large and repeated doses (2–4 mg IV repeated; up to 20 mg or more in severe cases) are needed — titrate to secretions, not tachycardia. Pralidoxime reactivates AChE but must be given with atropine (atropine is the primary rescue drug); give pralidoxime early, before ageing. Adrenaline is not indicated — the problem is not adrenergic.
CLINICAL PEARL
The 'alpha-first' rule in phaeochromocytoma: Never give a beta-blocker before establishing adequate alpha-blockade in a patient with a known or suspected phaeochromocytoma. Beta-blockade removes the only remaining dilatory (β2) counter-pressure against tumour-released catecholamines, leaving pure α1-mediated vasoconstriction — this can precipitate a life-threatening hypertensive crisis with organ damage. The correct sequence is: phenoxybenzamine orally for 10–14 days pre-op → add propranolol/atenolol after α-blockade is established → liberal IV fluids to expand the contracted intravascular volume. Intraoperatively, phentolamine IV is the agent of choice for acute BP spikes when the tumour is manipulated.
Second pearl — IM beats SC for adrenaline in anaphylaxis: Subcutaneous adrenaline is occasionally still given in error. Multiple pharmacokinetic studies (including the classic Simons 1998 study) show that IM adrenaline in the vastus lateralis achieves higher and faster peak plasma concentrations than SC in the deltoid region. The reason: subcutaneous vasoconstriction (α1 effect of adrenaline itself) limits its own absorption when given SC. IM injection bypasses this self-limiting loop.