Page 4 of 18
PH2.2 | PH2.2 | Cholinergic Drugs and Organophosphate Poisoning Management — SDL Guide — SDL Guide
Learning Objectives
- Describe the types, pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of cholinergic and anticholinergic drugs (PH2.2)
- Demonstrate organophosphate compound (OPC) poisoning management including recognition of the cholinergic toxidrome and the rationale for atropine and pralidoxime therapy (PH2.2)
INSTRUCTIONS
Cholinergic pharmacology governs a remarkably diverse therapeutic landscape — from the eye drops that lower intraocular pressure in glaucoma, to the drug that reverses neuromuscular blockade in the operating theatre, to the lifesaving protocol that keeps a pesticide-poisoned farmer alive in a rural emergency department. This guide builds from the receptor physiology you learned in Year 1, adds a drug-by-drug pharmacological profile for both agonists and antagonists, and culminates in a structured management protocol for organophosphate poisoning — one of the most common and preventable toxicological emergencies in South Asia.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed., Ch 7-8 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 10-11 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old male farmer from a rural taluk is brought to the emergency department by his family. He is unconscious, with pinpoint pupils, profuse salivation soaking his collar, generalised muscle fasciculations, and a HR of 36 bpm. His family says he was spraying insecticide when he suddenly collapsed. The nurse hands you a vial of atropine. How much do you give, and how do you know when to stop? In the next 20 minutes, the correct pharmacological decision will determine whether this man survives.
WHY THIS MATTERS
Organophosphate poisoning is not an exotic toxicology curiosity — in India it accounts for tens of thousands of emergency admissions annually, with agricultural workers and those in suicide attempts being the most common victims. Understanding cholinergic pharmacology is also central to everyday clinical practice: you will use neostigmine at the end of every general anaesthetic that uses neuromuscular blockade; you will prescribe ipratropium in COPD exacerbations; and you will encounter donepezil in every geriatric medicine ward. The anticholinergic toxidrome — dry skin, confusion, urinary retention, tachycardia — is a presentation you must be able to recognise in seconds to prevent treatment with the wrong drug class.
RECALL
The cholinergic system uses acetylcholine (ACh) as its neurotransmitter at multiple sites: all preganglionic autonomic synapses (sympathetic and parasympathetic), all postganglionic parasympathetic synapses, the neuromuscular junction (NMJ), and CNS synapses. ACh is synthesised in the nerve terminal from choline + acetyl-CoA (enzyme: choline acetyltransferase), stored in vesicles, released by exocytosis on nerve firing, and rapidly hydrolysed by acetylcholinesterase (AChE) in the synaptic cleft.
From Year-1 physiology, recall the two receptor families:
- Muscarinic receptors (M1–M5): activated by ACh and mimicked by muscarine (a mushroom alkaloid). Located at postganglionic parasympathetic end-organs: M1 (gastric glands, CNS — Gq), M2 (heart — Gi → ↓HR, ↓AV conduction), M3 (smooth muscle, glands — Gq → contraction + secretion), M4/M5 (CNS). Effects: SLUD — Salivation, Lacrimation, Urination, Defaecation (also bronchospasm and miosis).
- Nicotinic receptors (N_M, N_N): ligand-gated ion channels. N_M at the NMJ mediates skeletal muscle contraction; N_N at autonomic ganglia mediates ganglionic transmission. Nicotine activates both — this is why high-dose nicotine/organophosphate produces both secretory (muscarinic) and motor (nicotinic: fasciculations → paralysis) effects.
Pathophysiology of Cholinergic Transmission and ACh Receptor Subtypes
Cholinergic transmission begins with ACh synthesis. Choline acetyltransferase (ChAT) in the nerve terminal catalyses acetyl-CoA + choline → ACh. Choline is transported back into the terminal after hydrolysis by a high-affinity choline transporter — this reuptake is the rate-limiting factor for sustained cholinergic activity and is the molecular target of hemicholinium-3 (experimental, not clinical). ACh is stored in synaptic vesicles and released by calcium-dependent exocytosis.
Once in the synapse, ACh is rapidly degraded by two esterases:
- Acetylcholinesterase (AChE): the primary synapse-clearing enzyme. Located at the post-synaptic membrane and in erythrocytes. Turns over ACh at ~25,000 molecules/second per enzyme molecule — one of the fastest enzyme reactions in biology.
- Butyrylcholinesterase (BChE / pseudocholinesterase): in plasma; degrades succinylcholine and mivacurium. Relevant in anaesthesia — patients with atypical BChE genotype have prolonged succinylcholine block.
Muscarinic receptor subtype effector map:
| Receptor | Coupling | Location | Effect |
|---|---|---|---|
| M1 | Gq | Gastric parietal cells, CNS (cortex, hippocampus) | ↑Gastric acid secretion; cognitive function |
| M2 | Gi | SA node, AV node, atrial myocardium | ↓HR (negative chronotropy), ↓AV conduction |
| M3 | Gq | Smooth muscle (bronchi, GI, bladder detrusor), glands (salivary, lacrimal, sweat) | Bronchoconstriction, ↑GI motility, urination, secretions, miosis |
| M4 | Gi | Striatum, CNS | Modulation of dopamine pathways |
| M5 | Gq | CNS, blood vessels | Vasodilation, CNS effects |
Nicotinic receptor subtypes:
- N_M (muscle-type): at NMJ — pentameric (α₁β₁δε). Activation → Na⁺/K⁺ influx → depolarisation → end-plate potential → muscle contraction. Blocked by competitive (non-depolarising) NMBDs or depolarised by succinylcholine.
- N_N (neuronal-type): at autonomic ganglia — different subunit composition (α3β4 common). Blocked by ganglionic blockers (hexamethonium — historical antihypertensive).
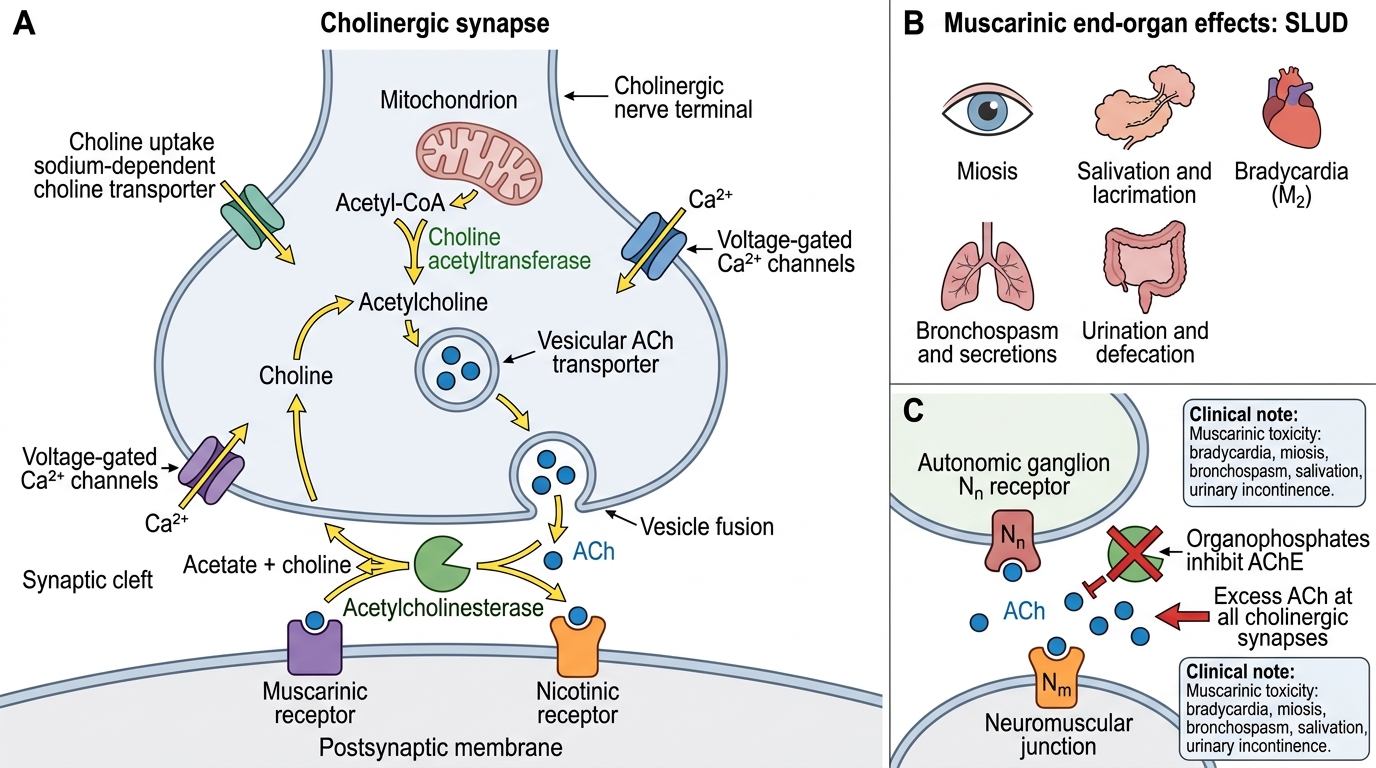
Cholinergic Synapse and Muscarinic SLUD Effects
SELF-CHECK
Organophosphates inhibit acetylcholinesterase at the synapse. Which of the following accurately describes the consequence of excess ACh accumulation at muscarinic receptors?
A. Tachycardia, dry mouth, dilated pupils, urinary retention
B. Bradycardia, miosis, excessive salivation, bronchospasm, urinary incontinence
C. Skeletal muscle paralysis only — muscarinic receptors are not affected by AChE inhibitors
D. Hypertension and diaphoresis — consistent with sympathetic activation
Reveal Answer
Answer: B. Bradycardia, miosis, excessive salivation, bronchospasm, urinary incontinence
AChE inhibition prevents ACh breakdown, causing its accumulation at all cholinergic synapses. At muscarinic receptors, this produces the SLUDGE/DUMBELS toxidrome: Bradycardia (M2), bronchospasm (M3), miosis (M3 — ciliary muscle + sphincter pupillae), salivation/lacrimation/urinary incontinence (M3), and GI hypermotility. Tachycardia, dry mouth, dilated pupils, and urinary retention are the opposite — features of anticholinergic (muscarinic antagonist) excess.
Therapeutic Rationale for Cholinergic Drug Therapy
The therapeutic goals of cholinergic drug manipulation fall into two broad categories: stimulating a deficient cholinergic state (agonists/AChE inhibitors) or blocking an excess cholinergic state (antagonists). The specific receptor subtype targeted determines which organ system is affected and which indication is appropriate.
Key therapeutic goals mapped to cholinergic pharmacology:
- Restore smooth muscle tone (post-operative urinary retention, paralytic ileus, atonic bladder): bethanechol (direct M3 agonist, oral/SC) — increases bladder detrusor and GI smooth muscle tone.
- Lower intraocular pressure (glaucoma): pilocarpine eye drops (M3 → ciliary muscle contraction → ↑trabecular outflow drainage; also miosis → relieves angle closure).
- Manage myasthenia gravis (autoimmune NMJ disorder): neostigmine or pyridostigmine (reversible AChE inhibitors → prolong ACh at NMJ → overcome receptor depletion).
- Reverse neuromuscular blockade (post-anaesthetic): neostigmine + glycopyrrolate/atropine — AChE inhibition at NMJ reverses non-depolarising blockade; antisecretory drug prevents systemic muscarinic excess from neostigmine.
- Symptomatic treatment of Alzheimer's dementia: donepezil, rivastigmine, galantamine (reversible, CNS-penetrant AChE inhibitors → slow decline; do not modify the disease course).
- Treat OPC/nerve agent poisoning: atropine (reverses muscarinic excess) + pralidoxime (reactivates AChE before irreversible ageing).
- Manage COPD/asthma bronchospasm: ipratropium (quaternary M3 antagonist, inhaled → blocks bronchoconstriction without CNS effects).
- Reduce secretions / prevent bradycardia perioperatively: glycopyrrolate (quaternary, does not cross BBB → no sedation/confusion — preferred over atropine in the elderly).
- Treat overactive bladder: oxybutynin, solifenacin (selective M3 antagonists → reduce detrusor overactivity).
Classification of Cholinergic Drugs
Cholinergic drugs are classified by primary action (agonist vs antagonist) and then by mechanism and receptor subtype. This two-level taxonomy is the foundation for predicting any agent's organ effects and adverse reactions.
Class 1: Cholinergic Agonists
Agonists enhance cholinergic activity via two mechanisms:
- Direct-acting muscarinic agonists (bind M receptors directly): pilocarpine (glaucoma, Sjögren's), bethanechol (urinary/GI tone), carbachol (eye surgery miosis), arecoline (betel nut — M + N). These agents are resistant to AChE hydrolysis (except ACh itself) because they lack or modify the ester hydrolysis site.
- Direct-acting nicotinic agonists: nicotine (ganglion + NMJ — complex dose-dependent effects), lobeline (historical nicotine substitute).
- Indirect-acting: AChE inhibitors — prevent ACh breakdown, effective at ALL ACh synapses:
- Reversible: neostigmine and pyridostigmine (quaternary amines — do NOT cross BBB; NMJ reversal + myasthenia); physostigmine (tertiary amine — CROSSES BBB; antidote for anticholinergic toxidrome); edrophonium (ultra-short, IV — historical myasthenia diagnosis); donepezil, rivastigmine, galantamine (CNS-penetrant, Alzheimer's).
- Irreversible: organophosphates (diisopropyl fluorophosphate [DFP], echothiophate, malathion, parathion, sarin, VX) and carbamates — covalent phosphorylation or carbamylation of AChE serine residue; persistent enzyme inhibition until new enzyme synthesised or oxime reactivation.
Class 2: Cholinergic Antagonists
Antagonists block ACh receptors:
- Muscarinic antagonists: atropine (non-selective M1–M3 prototype; tertiary amine, crosses BBB), hyoscine/scopolamine (more CNS penetration — motion sickness, pre-med), ipratropium (quaternary — no BBB — inhaled COPD), glycopyrrolate (quaternary — no BBB — perioperative), oxybutynin / solifenacin (M3-selective — overactive bladder), tropicamide / cyclopentolate (eye drops — mydriasis/cycloplegia).
- Ganglionic blockers: hexamethonium (N_N — historical, no longer used clinically).
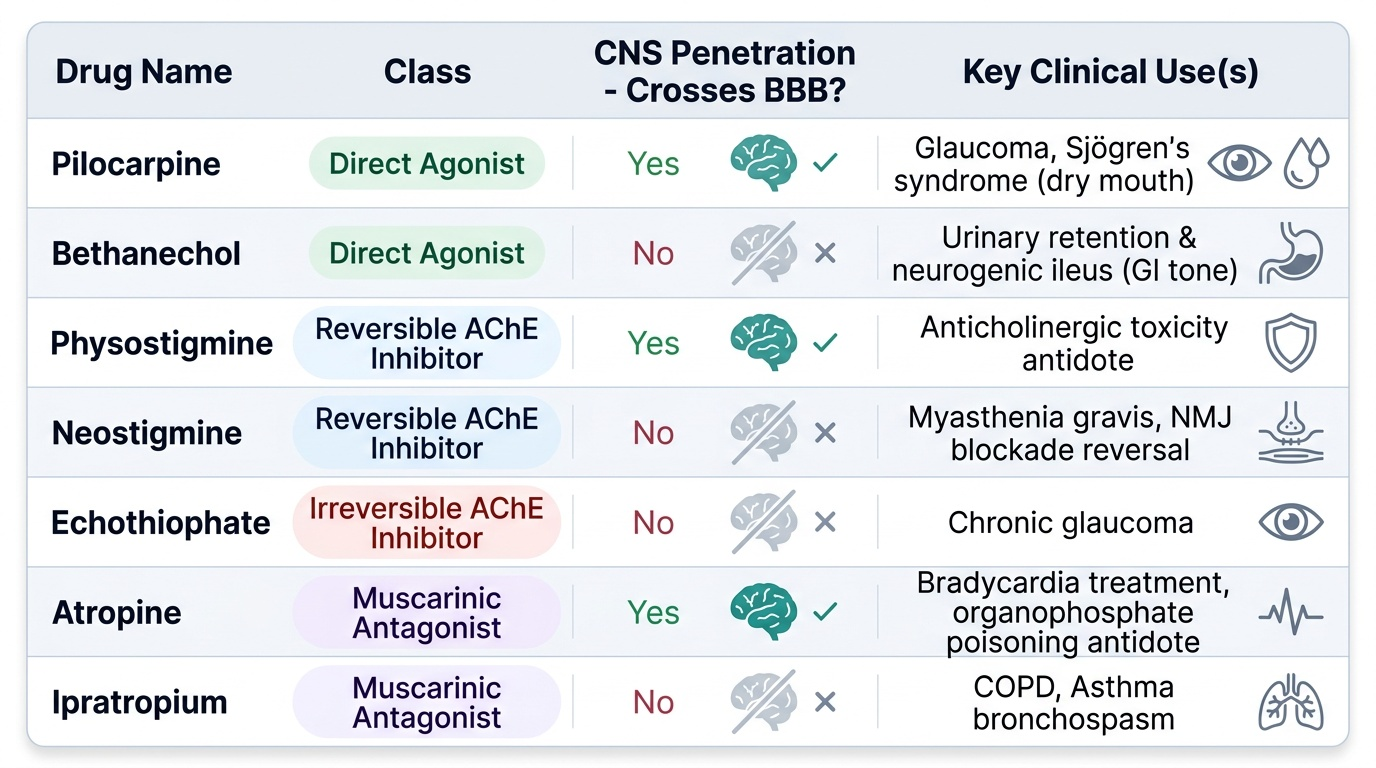
Provided image
SELF-CHECK
A patient recovering from general anaesthesia remains paralysed despite reversal with neostigmine. Neostigmine causes increased secretions and bradycardia. Which drug is given WITH neostigmine to counteract its systemic muscarinic effects, and why is atropine preferred over glycopyrrolate in some situations?
A. Adrenaline — to raise HR and dry secretions via α1 + β1 stimulation
B. Glycopyrrolate or atropine — muscarinic antagonists. Glycopyrrolate is preferred in elderly because it does NOT cross BBB (no confusion); atropine crosses BBB and can cause agitation/sedation
C. Pralidoxime — reactivates AChE so neostigmine effect is reversed directly
D. Propranolol — blocks the cardiac effects of ACh at β1 receptors
Reveal Answer
Answer: B. Glycopyrrolate or atropine — muscarinic antagonists. Glycopyrrolate is preferred in elderly because it does NOT cross BBB (no confusion); atropine crosses BBB and can cause agitation/sedation
Neostigmine's AChE inhibition at the NMJ reverses non-depolarising blockade, but systemic muscarinic effects (bradycardia, bronchospasm, secretions) require co-administration of a muscarinic antagonist. Glycopyrrolate (quaternary, does not cross BBB) is preferred in the elderly and patients at risk of confusion; atropine (tertiary, crosses BBB) works faster for acute bradycardia but can cause CNS stimulation or sedation. Propranolol is a β-blocker and would worsen bradycardia. Pralidoxime reverses organophosphate poisoning, not neostigmine.