Page 5 of 18
PH2.2 | PH2.2 | Cholinergic Drugs and Organophosphate Poisoning Management — SDL Guide — SDL Guide (Part 2)
Cholinergic Agonists and AChE Inhibitors — PK, PD, Uses, and Adverse Effects
The pharmacokinetic profile of a cholinergic agonist or AChE inhibitor is critically determined by its molecular structure — specifically, whether it is a quaternary amine (permanently charged, poor GI absorption, does NOT cross BBB) or a tertiary amine (uncharged, better oral bioavailability, CROSSES BBB). This structural distinction governs both the clinical utility and the adverse-effect profile of each agent.
| Drug | Class | BBB | Route | Key uses | Major ADRs |
|---|---|---|---|---|---|
| Pilocarpine | Direct muscarinic agonist | Limited (high conc.) | Eye drops, oral | Glaucoma (open-angle + angle-closure), Sjögren's (↑salivation) | Miosis, brow ache, blurred vision, systemic SLUD if absorbed |
| Bethanechol | Direct M agonist (selectively GI/bladder) | No | Oral, SC | Post-op urinary retention, neurogenic bladder, reflux oesophagitis (historical) | Salivation, sweating, GI cramps, bronchospasm (contraindicated in asthma) |
| Neostigmine | Reversible AChE inhibitor (quaternary) | No | IV, IM, oral | Myasthenia gravis, reversal of non-depolarising NMB, post-op ileus | SLUDGE, bradycardia, bronchospasm (give with atropine/glycopyrrolate for NMB reversal) |
| Pyridostigmine | Reversible AChE inhibitor (quaternary) | No | Oral, IV | Myasthenia gravis (preferred over neostigmine — longer action) | Similar to neostigmine |
| Physostigmine | Reversible AChE inhibitor (tertiary) | YES | IV, IM | Antidote for anticholinergic toxidrome (e.g. atropine overdose, tricyclic poisoning) | SLUDGE, seizures, bradycardia (must give carefully) |
| Donepezil | Reversible AChE inhibitor (tertiary) | YES | Oral | Alzheimer's dementia (mild–moderate → severe) | Nausea, diarrhoea, insomnia, bradycardia, syncope; does NOT modify disease |
| Rivastigmine | Pseudo-irreversible AChE inhibitor | YES | Oral, patch | Alzheimer's + Parkinson's dementia | Nausea (patch reduces GI ADRs), weight loss |
| Galantamine | Reversible AChE + nicotinic allosteric modulator | YES | Oral | Alzheimer's dementia | GI effects; less commonly bradycardia |
Key principle: the AChE inhibitors for dementia (donepezil/rivastigmine/galantamine) must penetrate the CNS to be effective — all are tertiary amines or lipophilic. They provide symptomatic benefit (modest improvement or slowing of cognitive decline) but do NOT reverse neurodegeneration. Adverse effects in the elderly (bradycardia, syncope, GI upset) require careful monitoring.
Anticholinergic Drugs — PK, PD, Uses, and Adverse Effects
Muscarinic antagonists compete with ACh for M receptors, reducing parasympathetic tone at end-organs. Their pharmacokinetics, like the agonists, depend critically on whether the drug is a quaternary (no BBB, no oral CNS effects) or tertiary amine (crosses BBB, has CNS effects). This structural distinction is the key to choosing between atropine and glycopyrrolate in clinical practice.
Atropine (prototype muscarinic antagonist)
Atropine is a tertiary amine alkaloid from Atropa belladonna. It is non-selective for M1–M3 receptors and crosses the blood-brain barrier, producing CNS effects. Dose-dependent organ effects:
- Low dose (0.1–0.2 mg): paradoxical bradycardia (block of presynaptic M1 inhibiting vagal inhibitory interneurons — vagal tone actually increases briefly)
- Moderate dose (0.5–1 mg): tachycardia (M2 block at SA node), dry mouth (M3 salivary glands)
- High dose (1–2+ mg): mydriasis (M3 — sphincter pupillae), cycloplegia, urinary retention (M3 — detrusor inhibition), decreased bowel sounds
- Very high dose (>5 mg): CNS effects — excitement, restlessness, hallucinations, delirium ('mad as a hatter'); hyperthermia ('hot as a hare'); flushed dry skin ('red as a beet').
Therapeutic uses: emergency bradycardia (0.5–1 mg IV), OPC poisoning (large IV doses), pre-anaesthetic medication (reduce secretions), ophthalmic (mydriasis/cycloplegia), antispasmodic (GI colic).
Anticholinergic toxidrome (recognised from atropine overdose or other anticholinergic agents — tricyclics, antihistamines, antipsychotics): dry as a bone (dry skin, no sweating), blind as a bat (mydriasis), red as a beet (flushed skin — cutaneous vasodilation), hot as a hare (hyperthermia — no sweating), mad as a hatter (confusion, hallucinations), full as a flask (urinary retention), heart racing like a rabbit (tachycardia).
Antidote for anticholinergic toxidrome: physostigmine 1–2 mg IV slowly (crosses BBB → reverses CNS + peripheral effects).
| Drug | BBB | Key use | Key distinguishing feature |
|---|---|---|---|
| Atropine | YES (tertiary) | Bradycardia, OPC poisoning, pre-anaesthetic | Prototype; full organ effects; CNS stimulation at high dose |
| Hyoscine (scopolamine) | YES (tertiary) | Motion sickness (transdermal patch), pre-med (sedation + antisecretory) | More CNS sedation and antiemetic effect than atropine |
| Ipratropium | NO (quaternary) | COPD, asthma (inhaled) | No systemic absorption → no CNS or cardiac effects; also minimal effect on sputum viscosity |
| Glycopyrrolate | NO (quaternary) | Perioperative (with neostigmine), sialorrhoea | No CNS sedation/confusion — preferred in elderly and in NMB reversal |
| Oxybutynin | YES (partial) | Overactive bladder | CNS effects (confusion in elderly); transdermal patch reduces CNS ADRs |
| Solifenacin / tolterodine | Minimal | Overactive bladder | More bladder-selective; fewer CNS and dry-mouth ADRs than oxybutynin |
SELF-CHECK
An elderly patient with moderate COPD and mild cognitive impairment is prescribed a muscarinic antagonist for bronchospasm. Which agent is most appropriate and why?
A. Atropine tablets — non-selective, most effective bronchodilation
B. Ipratropium inhaled — quaternary amine, does not cross BBB, no systemic or CNS effects, acts locally on airway M3 receptors
C. Oxybutynin oral — bladder-selective so does not affect the airways
D. Glycopyrrolate IV — parenteral route ensures highest bioavailability in COPD
Reveal Answer
Answer: B. Ipratropium inhaled — quaternary amine, does not cross BBB, no systemic or CNS effects, acts locally on airway M3 receptors
Ipratropium is the correct choice: it is a quaternary amine administered by inhalation, acting locally on M3 receptors in the bronchial smooth muscle to produce bronchodilation. It does not cross the BBB (no worsening of cognitive impairment), does not cause tachycardia or systemic muscarinic blockade at inhaled doses, and does not thicken secretions significantly (an old concern). Atropine orally would cause systemic adverse effects (tachycardia, confusion) unacceptable in this patient. Oxybutynin is bladder-selective, not airway-specific.
Organophosphate Poisoning — Pathophysiology and Management
Organophosphate compounds (OPC) — widely used as agricultural insecticides (malathion, parathion, chlorpyrifos) and as chemical warfare nerve agents (sarin, VX, novichok) — cause poisoning by irreversible covalent phosphorylation of the serine hydroxyl group at the active site of AChE. With the enzyme inactivated, ACh accumulates at all cholinergic synapses, producing a combined toxidrome.
Toxidrome features — remember DUMBELS (or SLUDGE + nicotinic + CNS):
Muscarinic effects (SLUDGE):
- Salivation, Lacrimation, Urination, Defaecation, GI cramps/vomiting, Emesis
- Also: Bradycardia, Bronchospasm, Bronchorrhoea (the 3Bs — most lethal)
- Miosis (M3 — characteristic early sign)
Nicotinic effects (NMJ excess):
- Muscle fasciculations, cramps, weakness → flaccid paralysis (end-plate depolarisation block)
- Sweating (though sweat glands are muscarinic, excess stimulation presents with diaphoresis)
CNS effects (central ACh excess):
- Anxiety, restlessness, seizures, loss of consciousness, central respiratory depression
AChE ageing: after organophosphate phosphorylation, the bond undergoes dealkylation ('ageing'), making reactivation by oximes impossible. The time to ageing is agent-specific: tabun/soman age within minutes to hours; parathion/malathion (agricultural OPCs) age over 24–48 hours, providing a longer window for pralidoxime.
Management Protocol — step by step:
- Remove from exposure / decontamination: remove contaminated clothing, wash skin with soap and water (wear gloves — absorbs through skin). Priority to prevent further absorption and staff contamination.
- Airway and breathing: high-flow oxygen; intubate if respiratory failure. Bronchospasm + bronchorrhoea are the primary causes of death.
3. Atropine — first-line antidote:
- Initial dose: 2–4 mg IV (much higher than typical clinical dose)
- Repeat every 5–10 minutes; titrate to secretions drying and bronchospasm resolving
- Do NOT titrate to tachycardia — the endpoint is resolution of bronchospasm and bronchorrhoea, not HR normalisation (pre-existing tachycardia from nicotinic effects can mislead)
- Total dose can be 20 mg or more in severe poisoning (doses that would be lethal in a normal person are well-tolerated in OPC poisoning because muscarinic receptors are massively over-stimulated)
4. Pralidoxime (2-PAM) — oxime AChE reactivator:
- Dose: 1–2 g IV over 15–30 minutes (WHO recommendation)
- Mechanism: oxime group attacks phosphorus in the phosphorylated AChE complex → displaces the phosphate → restores AChE activity
- Effective only before ageing — must be given within the agent-specific time window (generally <24–48h for agricultural OPCs; within minutes for soman)
- Pralidoxime reverses both nicotinic (fasciculation, weakness) and, to some extent, muscarinic effects — but atropine is still essential for muscarinic control
- Diazepam for seizures: IV benzodiazepine (GABA agonist) for OPC-induced seizures; seizures worsen hypoxia and outcome.
- Supportive care: ICU monitoring, mechanical ventilation if needed, continuous ECG (arrhythmias), glucose monitoring.
| Management Step | Drug | Dose | Endpoint/Rationale |
|---|---|---|---|
| Decontamination | None | — | Remove OPC before further absorption |
| Muscarinic block | Atropine | 2–4 mg IV; repeat q5–10 min | Dry secretions, resolve bronchospasm; titrate to secretions NOT HR |
| AChE reactivation | Pralidoxime | 1–2 g IV over 30 min | Restore AChE before ageing; effective within time window |
| Seizures | Diazepam | 5–10 mg IV | GABA agonist; prevents secondary anoxic injury |
| Airway | Intubation/O2 | — | Bronchorrhoea + respiratory paralysis are primary causes of death |
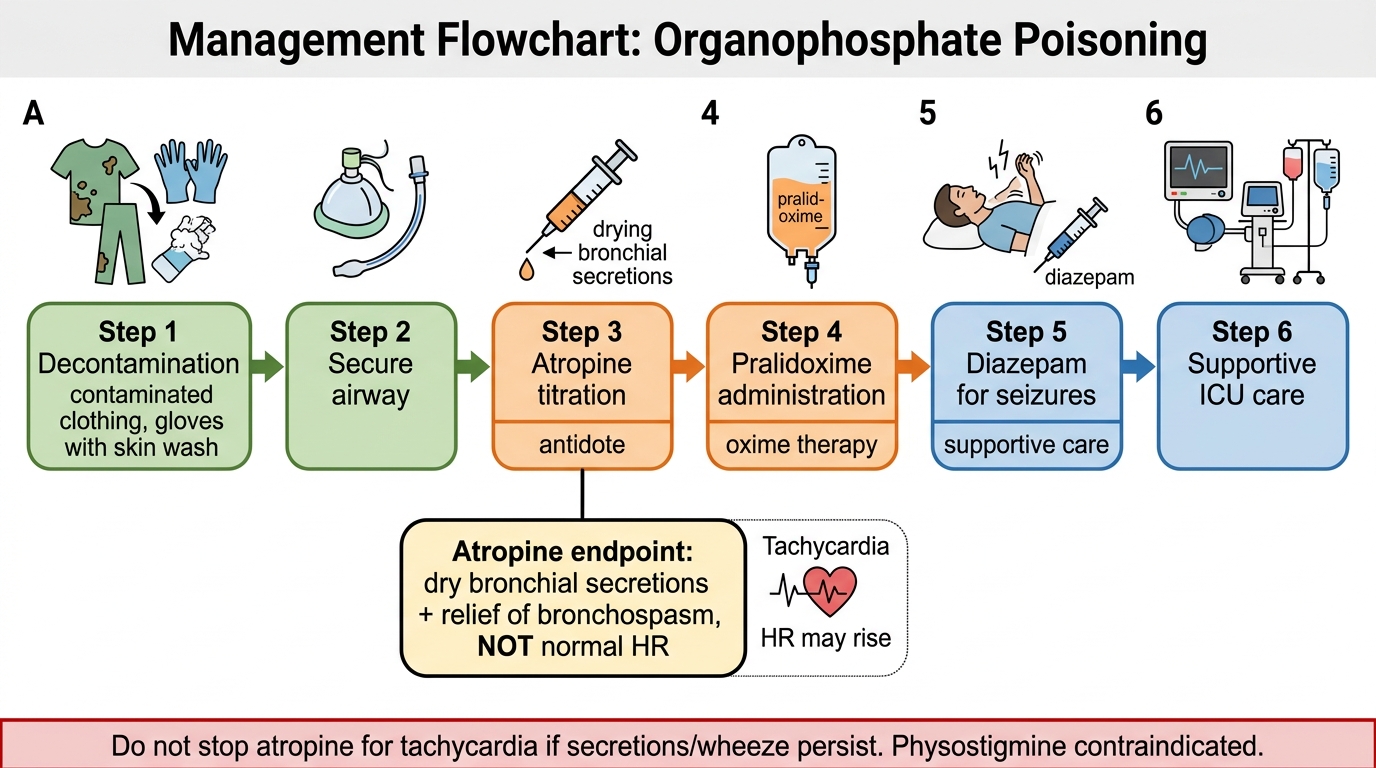
Organophosphate Poisoning Management Flowchart
SELF-CHECK
A patient with severe OPC poisoning has received 8 mg of atropine IV over 20 minutes. His HR is now 120 bpm, but he still has copious bronchial secretions and audible wheeze. What is the correct next step?
A. Stop atropine — tachycardia indicates atropine toxicity
B. Continue atropine — tachycardia is an acceptable outcome; the endpoint is drying of secretions and resolution of bronchospasm, not HR normalisation
C. Switch to glycopyrrolate — less cardiac stimulation
D. Give physostigmine to reverse the excess atropine
Reveal Answer
Answer: B. Continue atropine — tachycardia is an acceptable outcome; the endpoint is drying of secretions and resolution of bronchospasm, not HR normalisation
The therapeutic endpoint for atropine in OPC poisoning is NOT normalisation of heart rate — it is resolution of bronchospasm and drying of bronchial secretions. In severe OPC poisoning, nicotinic-mediated tachycardia (from NMJ and ganglionic stimulation) may already be present before any atropine. Continuing atropine despite tachycardia is correct practice. Stopping because of tachycardia is a common and dangerous mistake that allows fatal bronchorrhoea to continue. Physostigmine would worsen cholinergic excess and is absolutely contraindicated here.
CLINICAL PEARL
Carbamate vs organophosphate poisoning — the management difference: Both carbamates (e.g. carbaryl, methomyl) and organophosphates inhibit AChE and produce an identical cholinergic toxidrome. However, carbamate inhibition is spontaneously reversible (carbamylation is unstable; enzyme activity recovers in hours without oxime treatment). Pralidoxime is generally not required in carbamate poisoning and may be ineffective or even worsen toxicity (paradoxical ACh release from some preparations). Atropine is still the mainstay. The key clinical implication: when the poisoning agent is unknown, start with atropine (safe for both) while identification proceeds; pralidoxime is added if OPC is confirmed or strongly suspected.
Second pearl — the 'atropine challenge test': In a patient with suspected OPC poisoning but an uncertain diagnosis, give a test dose of atropine 1–2 mg IV. In a healthy person, this would cause tachycardia and dry mouth. In a patient with severe cholinergic excess from OPC, the same dose produces minimal or no tachycardia (and may not even dry secretions) — because the massively stimulated muscarinic receptors 'absorb' the atropine without visible effect. Absence of atropine effect = confirms severe OPC poisoning and signals the need for large atropine dosing.