Page 7 of 18
PH2.4 | PH2.4 | Skeletal Muscle Relaxants — SDL Guide — SDL Guide
Learning Objectives
- Explain the salient pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of skeletal muscle relaxants (PH2.4)
- Distinguish depolarising from non-depolarising neuromuscular blocking drugs (NMBDs) and explain their reversal strategies
- Describe centrally acting muscle relaxants and their role in spasticity management and malignant hyperthermia
INSTRUCTIONS
Skeletal muscle relaxants are indispensable in modern anaesthesia and critical care: without them, endotracheal intubation and abdominal surgery would not be possible in their current form. The neuromuscular junction (NMJ) is the precise anatomical target — understanding how ACh binds the N_M receptor and generates the end-plate potential is the foundation for understanding why succinylcholine causes fasciculations before paralysis, why rocuronium can be reversed in seconds by sugammadex, and why a patient with a spinal cord injury develops spasticity rather than flaccidity. This guide covers the full spectrum from the operating theatre to the neurology ward.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed., Ch 24-25 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 11 and Ch 19 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 02:00 at night. A 35-year-old patient is rushed into the operating theatre for emergency laparotomy after blunt abdominal trauma. The patient has a full stomach (ate 3 hours ago), making aspiration risk very high. The anaesthesiologist calls for rapid sequence induction (RSI). You are the intern on call. She asks: 'Succinylcholine or rocuronium?' Both are on the drug cart. You have 30 seconds to answer — and if you say succinylcholine for a patient with crush injuries and hyperkalaemia, you may cause a fatal cardiac arrest.
WHY THIS MATTERS
Muscle relaxant pharmacology is tested in every MBBS final practical and USMLE-style examination because errors in this domain directly cause patient harm in the operating theatre. Selecting succinylcholine in a patient with burns, spinal cord injury, or hyperkalaemia can kill within minutes by releasing intracellular potassium. Failing to reverse neuromuscular blockade before extubation is a cause of post-operative respiratory failure. Misdiagnosing malignant hyperthermia as fever delays dantrolene and results in preventable death. But these drugs are also powerful allies: rocuronium-sugammadex allows you to establish an airway in 60 seconds and fully reverse it in under 3 minutes — a combination that has saved thousands of 'can't intubate, can't oxygenate' scenarios. Understanding the pharmacology is what makes you safe.
RECALL
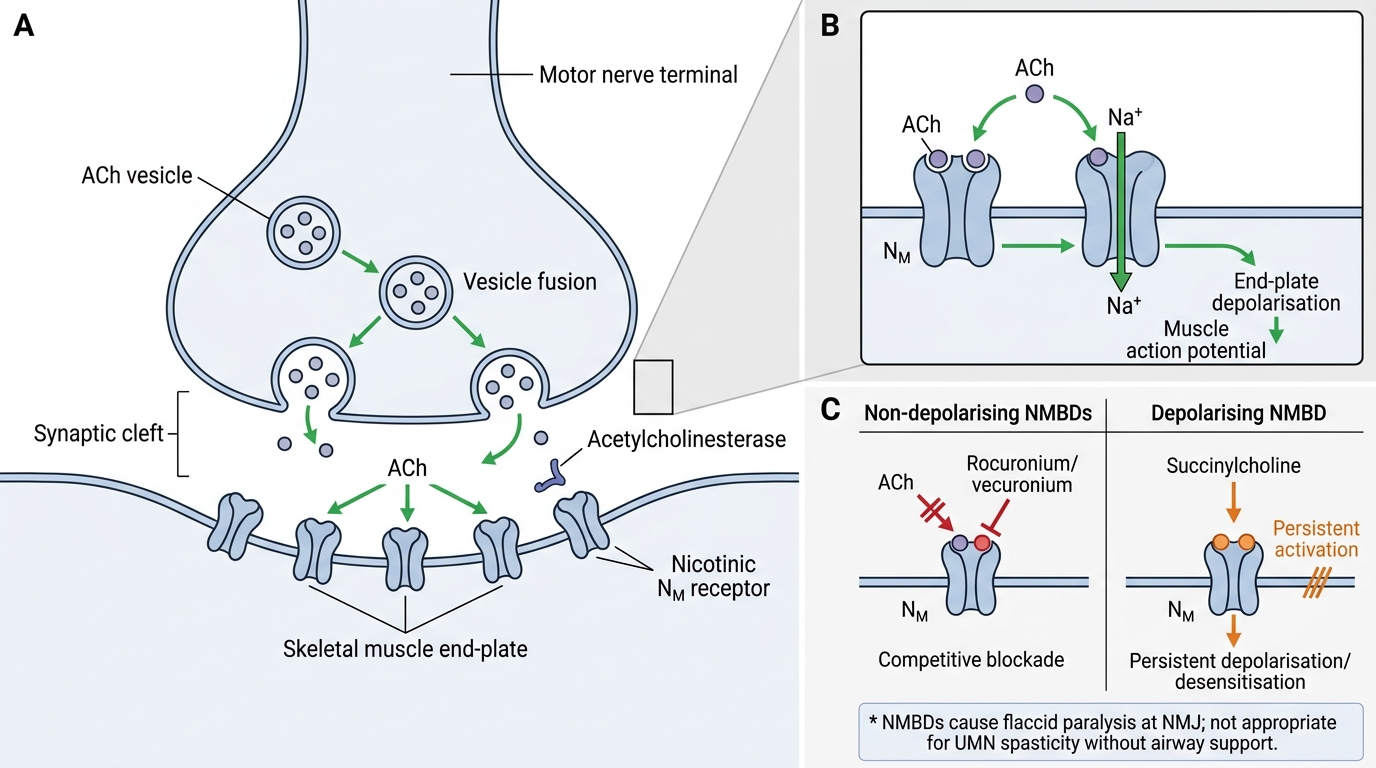
From your cholinergic pharmacology, recall the neuromuscular junction (NMJ): the motor nerve terminal releases acetylcholine (ACh) from vesicles in response to a nerve action potential. ACh crosses the synaptic cleft and binds nicotinic N_M receptors on the motor end-plate — these are pentameric ligand-gated ion channels (α₁β₁δε subunit composition at adult NMJ) that, when activated, allow Na⁺ influx and K⁺ efflux, generating an end-plate potential (EPP). If the EPP reaches threshold, a muscle action potential propagates → sarcoplasmic reticulum releases Ca²⁺ via ryanodine receptors (RyR1) → troponin-tropomyosin complex releases → actin-myosin cross-bridge cycling → contraction. ACh is hydrolysed by acetylcholinesterase in the synaptic cleft and butyrylcholinesterase (BChE) in plasma. This pathway is the target for both NMBDs (blocking the receptor or the depolarisation) and dantrolene (blocking the RyR1 Ca²⁺ release step).
Pathophysiology of Neuromuscular Transmission and Spasticity
Normal neuromuscular transmission requires the precise coordination of ACh synthesis, vesicular release, post-synaptic receptor activation, and enzymatic termination. Diseases and drugs can disrupt this at multiple steps, and the pharmacological consequences depend entirely on which step is affected.
The normal NMJ signal cascade:
1. Action potential arrives at motor nerve terminal → voltage-gated Ca²⁺ channels open → intracellular Ca²⁺ rises.
2. Ca²⁺ triggers SNARE protein-mediated vesicle fusion → ACh released into synaptic cleft (~10,000 molecules per vesicle).
3. ACh binds α-subunits of N_M receptor → channel opens → Na⁺ in/K⁺ out → depolarisation of end-plate region.
4. If sufficient EPPs summate → muscle fibre action potential → T-tubule depolarisation → RyR1 opens → Ca²⁺ from SR → contraction.
5. AChE (concentrated in the synaptic folds) hydrolyses ACh rapidly → channel closes → end-plate repolarises.
Spasticity pathophysiology: In upper motor neuron (UMN) lesions (stroke, spinal cord injury, multiple sclerosis), descending cortical and reticulospinal inhibitory pathways are disrupted. The spinal reflex arc (Ia afferents → alpha motor neuron → muscle) loses its descending inhibitory control, becoming hyperexcitable. Result: increased muscle tone, clonus, and exaggerated deep tendon reflexes. This is why centrally acting spasmolytics (baclofen, diazepam, tizanidine) — which restore inhibitory tone at the spinal cord level — are appropriate for spasticity management, while NMBDs would cause complete flaccid paralysis and are unsuitable.
Key distinction: spasticity (velocity-dependent UMN hypertonia, treated with spasmolytics) vs spasm (acute painful muscle contraction from local injury, treated with shorter-term relaxants like diazepam or cyclobenzaprine).
Neuromuscular Junction and NMBD Targets
SELF-CHECK
A patient with multiple sclerosis develops lower limb spasticity (increased tone, clonus, painful muscle spasms). Which drug class is appropriate for managing this, and why are neuromuscular blocking drugs inappropriate?
A. Non-depolarising NMBDs — they safely relax muscles without CNS effects
B. Centrally acting spasmolytics (baclofen, tizanidine) — they reduce spinal cord hyperexcitability while preserving voluntary motor control and consciousness; NMBDs would abolish all voluntary movement and require ventilatory support
C. Succinylcholine — it is short-acting and easy to reverse
D. Dantrolene — it reliably reverses UMN spasticity by peripheral mechanism
Reveal Answer
Answer: B. Centrally acting spasmolytics (baclofen, tizanidine) — they reduce spinal cord hyperexcitability while preserving voluntary motor control and consciousness; NMBDs would abolish all voluntary movement and require ventilatory support
Spasticity requires restoration of inhibitory control at the spinal cord level without abolishing voluntary motor function. Centrally acting spasmolytics (baclofen — GABA-B agonist; tizanidine — α2 agonist; diazepam — GABA-A) reduce hyperexcitable spinal interneuron firing while leaving consciousness and volitional movement partially intact. NMBDs act at the NMJ and cause complete flaccid paralysis — patients would require mechanical ventilation and ICU care, making them entirely inappropriate for ambulatory spasticity management. Dantrolene acts peripherally on RyR1 and can reduce tone but is reserved for MH and NMS, not chronic spasticity (significant hepatotoxicity with long-term use).
Therapeutic Rationale for Muscle Relaxant Therapy
Skeletal muscle relaxants serve three distinct therapeutic goals in clinical medicine, each addressed by a different mechanism and drug class. Understanding the rationale prevents the catastrophic error of choosing a drug from the wrong category for the clinical need.
Goal 1: Facilitate endotracheal intubation and surgical relaxation
For general anaesthesia, complete abolition of voluntary and reflex skeletal muscle activity is required for laryngoscopy and intubation (to prevent laryngospasm), abdominal surgery (to allow surgical access without visceral herniation), and mechanical ventilation synchrony. Only NMBDs acting at the NMJ can achieve this reliably and safely. Duration of action is matched to the surgical procedure.
Goal 2: Manage spasticity in chronic neurological disease
In stroke, multiple sclerosis, spinal cord injury, and cerebral palsy, upper motor neuron lesions cause chronic spasticity that impairs function, causes pain, and leads to contractures. The goal is to reduce tone while preserving some voluntary function. Centrally acting agents (baclofen, tizanidine, diazepam) are used — they do not produce the complete paralysis of NMBDs and are suitable for outpatient use.
Goal 3: Treat malignant hyperthermia (MH) and prevent rhabdomyolysis
Malignant hyperthermia is a life-threatening pharmacogenomic crisis triggered by volatile anaesthetics or succinylcholine in genetically susceptible individuals (mutations in RyR1 or CACNA1S genes → uncontrolled Ca²⁺ release from SR). The only specific pharmacological antidote is dantrolene, which acts peripherally by blocking RyR1, reducing the pathological Ca²⁺ cascade. Dantrolene is also used in neuroleptic malignant syndrome (NMS — dopamine antagonist-induced hyperthermia with rigidity — similar peripheral mechanism of action).
Classification of Skeletal Muscle Relaxants
The two-level classification of skeletal muscle relaxants is clinically essential: a drug from the wrong class, given for the wrong indication, can cause fatal complications.
Class 1: Neuromuscular Blocking Drugs (NMBDs) — act at the NMJ
These drugs block neuromuscular transmission and cause complete skeletal muscle paralysis. They do NOT cross the BBB and have no CNS sedative effects — the patient is paralysed but not anaesthetised (anaesthesia requires separate agents). Classified by mechanism:
- 1a. Depolarising NMBDs: succinylcholine (suxamethonium) — only clinical example. Binds N_M receptors like ACh, causing persistent depolarisation (fasciculations → Phase 1 block). The end-plate remains depolarised and refractory. Onset: 60 seconds. Duration: 10–15 minutes (hydrolysed by BChE). Reversed by waiting (no pharmacological antidote; neostigmine worsens Phase 1 block).
- 1b. Non-depolarising NMBDs (competitive antagonists): bind α-subunit of N_M receptor competitively, preventing ACh access. No initial depolarisation — flaccid paralysis from the start. Reversed by neostigmine (AChE inhibition → ↑ACh competes the NMBD off) or sugammadex (for rocuronium/vecuronium). Subclassified by structure:
- Steroidal: rocuronium, vecuronium, pancuronium (vagolytic → tachycardia), pipecuronium.
- Benzylisoquinoline: atracurium, cisatracurium (Hofmann elimination — organ-independent), mivacurium (BChE — prolonged in BChE deficiency), tubocurarine (historical — histamine release → bronchospasm, ↓BP).
Class 2: Centrally Acting Skeletal Muscle Relaxants (Spasmolytics)
Act on spinal interneurons or supraspinal pathways to reduce pathological muscle tone. They do NOT block the NMJ — voluntary motor function is partially preserved.
- Baclofen: GABA-B receptor agonist at spinal cord (inhibits Ia afferent release + postsynaptic hyperpolarisation of alpha motor neurons). Oral or intrathecal (pump) for severe MS/SCI spasticity.
- Diazepam: GABA-A positive allosteric modulator (↑Cl⁻ influx → spinal cord interneuron inhibition). Useful for acute painful muscle spasm and adjunct in chronic spasticity.
- Tizanidine: central α2 agonist (like clonidine) — reduces excitatory interneuron firing at spinal level. Less sedation than diazepam, similar efficacy for spasticity.
- Dantrolene (unique — peripheral mechanism): blocks RyR1 (ryanodine receptor type 1) in skeletal muscle SR → prevents Ca²⁺ release → reduces contractile force. Used for: malignant hyperthermia (IV acute), neuroleptic malignant syndrome, occasionally chronic spasticity (hepatotoxicity limits long-term use).