Page 8 of 18
PH2.4 | PH2.4 | Skeletal Muscle Relaxants — SDL Guide — SDL Guide (Part 2)
Neuromuscular Blocking Drugs — PK, PD, Uses, and Adverse Effects
Neuromuscular blocking drugs are among the most precisely titrated drugs in clinical medicine. Their pharmacokinetics — especially onset, duration, and metabolic pathway — directly determine which agent is chosen for a given clinical scenario. Understanding the distinction between depolarising and non-depolarising mechanisms is the key to safe NMB management.
Succinylcholine (suxamethonium) — the depolarising NMBD:
Succinylcholine is two molecules of ACh joined at their acetyl groups. It binds N_M receptors and causes persistent end-plate depolarisation (Phase 1 block — fasciculations are visible within 10–15 seconds as the muscle responds to sustained depolarisation before becoming inexcitable). Onset: ~60 seconds (fastest of any NMBD). Duration: 10–15 minutes (hydrolysed by plasma BChE/pseudocholinesterase). Route: IV only.
Critical adverse effects of succinylcholine:
1. Hyperkalaemia: the persistent depolarisation causes K⁺ efflux from all depolarised muscle fibres. In normal patients, K⁺ rises ~0.5–1 mEq/L (tolerated). In patients with burns (>24h old), prolonged immobilisation, spinal cord injury (>24h), crush injuries, or denervation injuries — upregulation of extrajunctional ACh receptors (spread beyond NMJ) causes massive K⁺ release → potentially fatal hyperkalaemia and cardiac arrest.
2. Malignant hyperthermia trigger: succinylcholine, together with volatile anaesthetics (halothane, sevoflurane), can trigger MH in genetically susceptible individuals.
3. Fasciculations → post-operative myalgia (muscle pain from uncoordinated contraction — can be reduced by prior small non-depolarising NMBD dose 'defasciculation').
4. Bradycardia: repeated or high doses → direct M2 receptor stimulation (ACh-like structure).
5. Prolonged block (succinylcholine apnoea): in patients with atypical BChE (pseudocholinesterase deficiency) — inherited or acquired — block lasts hours instead of minutes.
6. Raised intraocular and intragastric pressure (fasciculations + succinylcholine effect): caution in open eye injuries and gastric reflux.
Non-depolarising NMBDs:
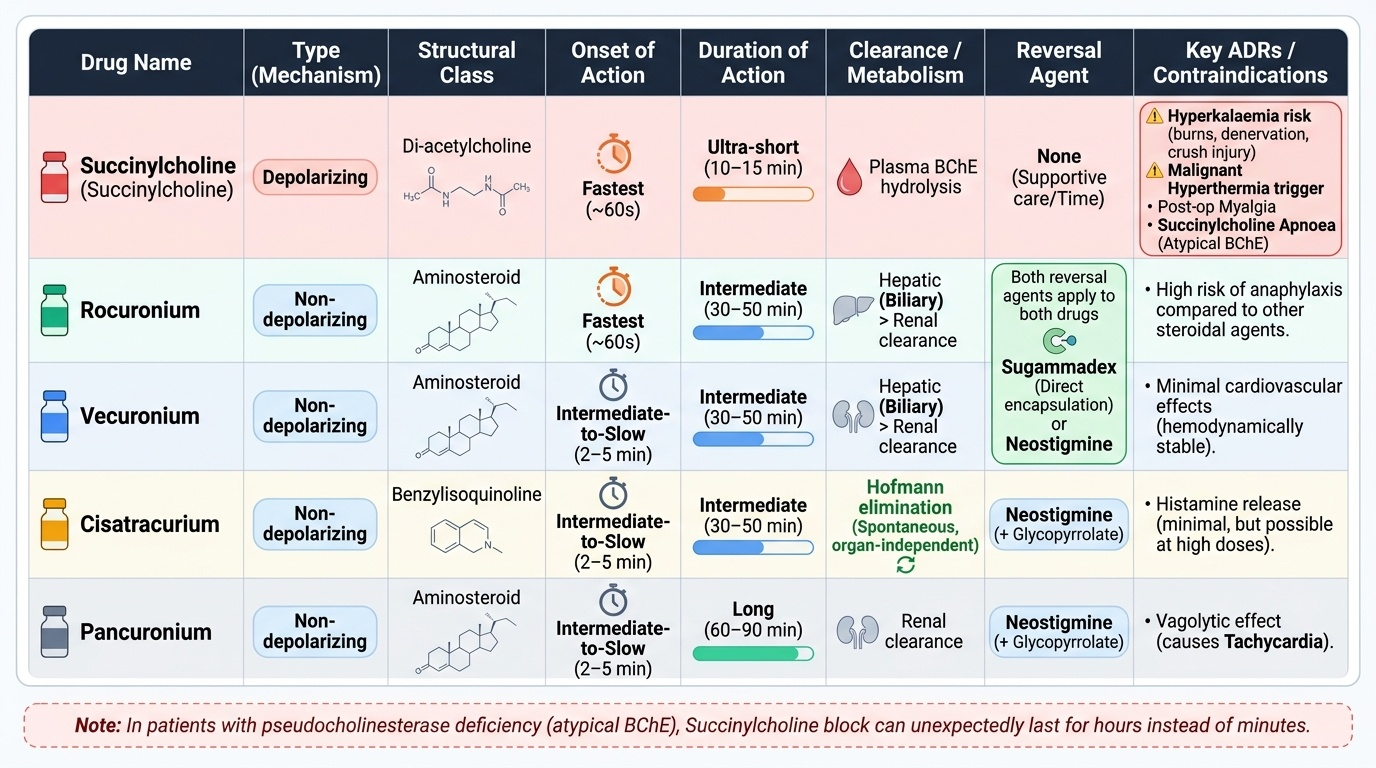
Provided image
Key agents:
- Rocuronium: steroidal, intermediate onset (~60–90 sec at 0.6 mg/kg; ~60 sec at RSI dose 1.2 mg/kg), intermediate duration (~30–60 min). Hepatic clearance. Reversed by neostigmine (standard) or sugammadex (rapid, complete reversal even from deep block). Contraindicated in patients allergic to rocuronium. RSI alternative to succinylcholine when succinylcholine is contraindicated.
- Atracurium/Cisatracurium: benzylisoquinoline — Hofmann elimination (spontaneous chemical degradation at physiological temperature and pH) + ester hydrolysis. Organ-independent clearance → drug of choice in severe hepatic or renal failure. Cisatracurium: less histamine release than atracurium, preferred in ICU.
- Vecuronium: steroidal, intermediate duration, hepatic clearance. No vagolytic or histamine effects — haemodynamically neutral.
- Pancuronium: steroidal, long duration (~90–120 min), vagolytic (blocks cardiac M2 → tachycardia — limits use in ischaemic heart disease). Renal + hepatic clearance.
Reversal of non-depolarising NMBDs:
- Neostigmine (AChE inhibitor): works by increasing ACh at NMJ to compete off the NMBD. Requires some residual neuromuscular function (TOF ratio >0.2 for adequate reversal). Must give with glycopyrrolate or atropine to prevent muscarinic adverse effects.
- Sugammadex: a modified gamma-cyclodextrin that encapsulates rocuronium or vecuronium molecules in a 1:1 ratio, rapidly removing them from the NMJ and plasma. Reversal is independent of neuromuscular function — can reverse from deep block. Dose: 2 mg/kg (routine), 4 mg/kg (deep block, TOF=0), 16 mg/kg (immediate emergency reversal of RSI dose 1.2 mg/kg rocuronium within 3 minutes of dose).
Monitoring: Train-of-four (TOF) stimulation — 4 electrical stimuli applied to peripheral nerve (usually ulnar). Count of twitches (0–4) and fade ratio guides reversal timing. TOF ratio ≥0.9 = adequate recovery.
SELF-CHECK
A 40-year-old with crush injuries from a road traffic accident requires emergency intubation 36 hours after the incident. Pre-operative potassium is 5.2 mEq/L. Which NMBD is appropriate for RSI and why?
A. Succinylcholine 1.5 mg/kg — fastest onset, best RSI conditions
B. Rocuronium 1.2 mg/kg IV — avoids succinylcholine's K⁺ release risk in a patient with crush injury and borderline hyperkalaemia; reversed by sugammadex 16 mg/kg if needed
C. Atracurium 0.5 mg/kg — Hofmann elimination safest in trauma
D. Pancuronium 0.1 mg/kg — long duration ensures no awareness during emergency surgery
Reveal Answer
Answer: B. Rocuronium 1.2 mg/kg IV — avoids succinylcholine's K⁺ release risk in a patient with crush injury and borderline hyperkalaemia; reversed by sugammadex 16 mg/kg if needed
Succinylcholine is contraindicated in crush injuries (>24h) because upregulated extrajunctional ACh receptors across denervated and injured muscle lead to massive K⁺ efflux on succinylcholine administration — potentially precipitating fatal hyperkalaemia (K⁺ can rise 2–5 mEq/L, causing cardiac arrest). Rocuronium 1.2 mg/kg provides RSI-equivalent conditions (onset ~60 sec) without the K⁺ risk. Crucially, sugammadex 16 mg/kg can immediately reverse this high dose of rocuronium if the airway fails — providing a 'can't intubate, can ventilate' escape. Atracurium and pancuronium have slower onsets and are not appropriate for RSI.
Centrally Acting Muscle Relaxants — PK, PD, Uses, and Adverse Effects
Centrally acting skeletal muscle relaxants reduce pathological muscle tone by acting on the central nervous system or, in the case of dantrolene, on the peripheral mechanism of contraction. They are pharmacologically distinct from NMBDs and cannot substitute for them — they are the outpatient neurologist's and rehabilitation physician's tools, not the anaesthesiologist's.

Provided image
Baclofen
Baclofen is a GABA-B receptor agonist — it mimics GABA at presynaptic GABA-B receptors on Ia afferent terminals (reducing glutamate release) and at postsynaptic GABA-B receptors on alpha motor neurons (Gi → K⁺ channel opening → hyperpolarisation → reduced motor neuron firing). It does not cross the BBB well at oral doses, but intrathecal delivery (via implanted pump) achieves therapeutic spinal concentrations with minimal systemic effects. Uses: spasticity in multiple sclerosis, spinal cord injury, cerebral palsy. Key ADRs: sedation, dizziness, muscle weakness (dose-related), abrupt withdrawal = severe baclofen withdrawal syndrome (hallucinations, seizures, hyperthermia — taper slowly). Overdose → coma, respiratory depression.
Diazepam
A benzodiazepine that acts as a positive allosteric modulator at GABA-A receptors throughout the CNS, including spinal interneurons involved in the polysynaptic reflex arc that mediates spasm. Effectively reduces both acute spasm (musculoskeletal, after trauma) and contributes to spasticity reduction. The sedation and dependence risks limit its use to short-term and adjunctive roles.
Tizanidine
Tizanidine is a central α2 receptor agonist (related structurally to clonidine) that acts at the spinal cord and supraspinal levels to reduce excitatory interneuron activity, decreasing alpha motor neuron firing. Unlike baclofen, tizanidine produces less weakness relative to tone reduction. ADRs: sedation, dry mouth, hepatotoxicity (monitor LFTs), hypotension, bradycardia. Used as first- or second-line spasmolytic for spasticity.
Dantrolene — peripheral mechanism:
Dantrolene is unique among 'muscle relaxants' — it acts NOT on the CNS or NMJ but on the ryanodine receptor type 1 (RyR1) in the sarcoplasmic reticulum of skeletal muscle, blocking Ca²⁺ release. This reduces the Ca²⁺ available for troponin C, directly impairing the excitation-contraction coupling step. Cardiac and smooth muscle RyR2/RyR3 are less sensitive to dantrolene.
Critical uses:
- Malignant hyperthermia (MH): life-threatening crisis from uncontrolled RyR1-mediated Ca²⁺ release, triggered by volatile anaesthetics or succinylcholine in susceptible individuals (RYR1 or CACNA1S gene mutations). Clinical features: rapidly rising temperature (>40°C), severe rigidity ('masseter spasm' may be the first sign), metabolic acidosis, hyperkalaemia, rising CO₂ → treat with dantrolene 2.5 mg/kg IV bolus, repeated every 5–10 minutes up to 10 mg/kg total, while stopping the triggering agent, cooling the patient, and treating metabolic derangements.
- Neuroleptic malignant syndrome (NMS): antipsychotic-induced dopamine blockade in hypothalamus + peripheral muscle RyR dysregulation → hyperthermia, severe rigidity, altered consciousness. Dantrolene + bromocriptine (D2 agonist) used adjunctively.
Long-term oral dantrolene for chronic spasticity: significant hepatotoxicity risk (up to 1% with prolonged use) — limits use to patients with severe spasticity unresponsive to other agents (cerebral palsy, SCI).
SELF-CHECK
During a laparotomy under halothane anaesthesia, a patient's end-tidal CO₂ begins rising rapidly, HR increases to 140 bpm, and the anaesthesiologist notes the patient's body is becoming rigid despite deepening anaesthesia. Which drug is immediately indicated, and what is its mechanism?
A. Atropine 1 mg IV — treat the tachycardia with a vagal blocker
B. Dantrolene 2.5 mg/kg IV — blocks RyR1 in skeletal muscle SR to halt the uncontrolled Ca²⁺ release causing malignant hyperthermia
C. Succinylcholine 1.5 mg/kg IV — complete muscle paralysis will stop the rigidity
D. Neostigmine — reverse any residual neuromuscular blockade causing the rigidity
Reveal Answer
Answer: B. Dantrolene 2.5 mg/kg IV — blocks RyR1 in skeletal muscle SR to halt the uncontrolled Ca²⁺ release causing malignant hyperthermia
This is a malignant hyperthermia (MH) crisis triggered by halothane (a volatile anaesthetic). MH occurs in genetically susceptible individuals (RYR1 mutation) when volatile anaesthetics/succinylcholine trigger uncontrolled Ca²⁺ release from the SR via RyR1, leading to hypermetabolism, hyperthermia, rigidity, and metabolic acidosis. The specific antidote is dantrolene 2.5 mg/kg IV (repeat up to 10 mg/kg total), which blocks RyR1 and halts the pathological Ca²⁺ cascade. The triggering agent (halothane) must also be immediately discontinued. Succinylcholine is itself a potential MH trigger and is absolutely contraindicated.
Clinical Decision-Making: Choosing and Monitoring Muscle Relaxants
The clinical application of muscle relaxant knowledge requires matching the pharmacological profile of each agent to the clinical scenario — contraindications to succinylcholine, appropriate reversal strategy, and MH recognition and treatment are the three highest-yield areas.
1. RSI (Rapid Sequence Induction) — which NMBD?
RSI is used when rapid loss of consciousness and immediate intubation are required in patients at risk of pulmonary aspiration (full stomach, emergency surgery, trauma). Two options:
| Feature | Succinylcholine | Rocuronium (RSI dose 1.2 mg/kg) |
|---|---|---|
| Onset | ~60 sec | ~60 sec (at 1.2 mg/kg) |
| Duration | 10–15 min | 60–90 min |
| Reversal if airway fails | Wait (no antidote) | Sugammadex 16 mg/kg → reversal in <3 min |
| Contraindications | Burns (>24h), SCI, crush injuries, hyperkalaemia, MH susceptibility, atypical BChE, open eye injury, personal/family history of MH | Allergy to rocuronium/sugammadex |
| Intubating conditions | Excellent | Excellent at 1.2 mg/kg |
Choice principle: if succinylcholine is contraindicated, rocuronium 1.2 mg/kg + sugammadex available is the safe alternative.
2. NMB monitoring — Train-of-Four (TOF)
TOF stimulation delivers four supramaximal nerve stimuli at 2 Hz. In a non-paralysed patient: 4 equal twitches (ratio 1.0). As NMBD depth increases: fewer twitches (0–4 count), with fade (diminishing amplitude). Reversal is adequate when TOF count 4/4 and TOF ratio ≥0.9 (measured by acceleromyography). Neostigmine reversal requires TOF count ≥2 for effectiveness.
3. Reversal strategies:
- Neostigmine + glycopyrrolate: for non-depolarising NMBDs when TOF ≥2. Cannot be used for succinylcholine.
- Sugammadex: for rocuronium or vecuronium, at any depth of block. Dose: 2 mg/kg (routine), 4 mg/kg (deep, TOF=0), 16 mg/kg (emergency reversal of 1.2 mg/kg RSI within 3 min).
- No pharmacological reversal for succinylcholine — Phase 1 block reverses spontaneously as BChE hydrolyses the drug.
4. MH recognition and management — MHAUS protocol:
1. Stop trigger (volatile anaesthetic + succinylcholine) immediately.
2. Dantrolene 2.5 mg/kg IV bolus — repeat every 5–10 min up to 10 mg/kg (each 20 mg vial must be dissolved in 60 mL sterile water — have enough vials).
3. Cooling: ice packs, cold IV fluids, surface cooling.
4. Treat metabolic derangements: bicarbonate for acidosis, calcium/insulin-dextrose for hyperkalaemia, antiarrhythmics (amiodarone — avoid calcium channel blockers, which worsen Ca²⁺ dysregulation).
5. Transfer to ICU. Test for MH susceptibility (caffeine-halothane contracture test or genetic testing — RYR1/CACNA1S).
5. Choosing a spasmolytic:
- Spasticity (chronic UMN, MS, SCI): baclofen (first-line), tizanidine (alternative), diazepam (adjunct or if baclofen fails).
- Acute painful muscle spasm (trauma, back pain): diazepam short-term, or cyclobenzaprine (not on NMC PH2.4 core list).
- Cerebral palsy severe spasticity: intrathecal baclofen pump.
- NMS or MH acute: dantrolene IV.
CLINICAL PEARL
Sugammadex — the game-changer in 'can't intubate, can't oxygenate' (CICO): Before sugammadex, a failed intubation after a large dose of rocuronium meant the patient could be paralysed for 60+ minutes with no pharmacological exit. Sugammadex 16 mg/kg IV reverses 1.2 mg/kg rocuronium in under 3 minutes — restoring breathing and avoiding the need for emergency surgical airway in many CICO scenarios. This has fundamentally changed anaesthetic practice: rocuronium + sugammadex is increasingly chosen over succinylcholine for RSI precisely because of this reversibility safety net. The cost of sugammadex remains a barrier in low-resource settings, which is why knowing succinylcholine's contraindications is still essential.
Second pearl — 'masseter rigidity' is an MH warning sign: Masseter muscle spasm after succinylcholine administration (difficulty opening the jaw for laryngoscopy) is an early warning sign of possible MH in susceptible patients. It is not diagnostic alone (some patients with normal RYR1 develop transient masseter rigidity), but it mandates vigilance — cancel the case if possible, monitor core temperature, and have dantrolene immediately available.