Page 10 of 18
PH2.5 | PH2.5 | Local Anaesthetics and Administration Techniques — SDL Guide — SDL Guide
Learning Objectives
- Explain the types, salient pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of local anaesthetics (PH2.5)
- Demonstrate understanding of the various methods of administration of local anaesthetics including topical, infiltration, nerve block, epidural, and spinal techniques (PH2.5)
INSTRUCTIONS
Local anaesthetics are the most frequently injected drugs in medicine. A dentist uses lignocaine hundreds of times a year; an obstetrician administers epidural bupivacaine for labour analgesia in the delivery suite; an emergency physician blocks the intercostal nerve for a fractured rib. Understanding local anaesthetic pharmacology — from the Na⁺ channel mechanism to the maximum dose calculation and the treatment of systemic toxicity — is a core clinical competency that you will use from your first year of internship. This guide builds from the channel physiology, through drug classification and pharmacokinetics, to the practical techniques and safety boundaries that govern every injection.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed., Ch 26 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 20 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old man undergoing repair of a hand laceration in the emergency department receives lignocaine infiltration. After 3 mL injected, he suddenly says he feels 'ringing in his ears' and then begins to have perioral tingling. Thirty seconds later he has a generalised tonic-clonic seizure. The nurse asks: 'Did you give too much? What do we do now?' The registrar looks at you — you are the one who drew up the drug. You need to know: how much was safe, what happened pharmacologically, and what the antidote is.
WHY THIS MATTERS
Local anaesthetic toxicity — systemic absorption causing CNS excitation, seizures, and cardiac arrhythmia — is a preventable emergency that occurs in emergency departments, operating theatres, and outpatient clinics worldwide. But local anaesthetics are also the pharmacological tools that make pain-free dentistry, painless labour, and awake craniotomy possible. The ability to calculate the maximum safe dose for a patient, choose the right technique for the clinical need, and manage a toxicity event are skills you will exercise every week of your clinical career. The pharmacokinetic principles — pKa, protein binding, lipid solubility — that determine onset, duration, and toxicity are universally applicable and frequently examined.
RECALL
From Year-1 physiology, recall how action potentials propagate along sensory nerves. Voltage-gated sodium channels (Nav) are transmembrane protein complexes with a pore-forming α-subunit consisting of four homologous domains (I–IV), each containing six transmembrane segments (S1–S6). The S4 segment is the voltage sensor; the S6 segments form the inner pore lining. The channel exists in three states: resting (closed but activatable), open (conducting Na⁺), and inactivated (closed, non-conducting, after rapid depolarisation). Local anaesthetics bind to a site on the inner face of S6 segments during the inactivated state — this is the pharmacological basis of use-dependent block: neurons firing at high frequency (many action potentials, spending more time in the inactivated state) are more susceptible to LA block. Pain fibres (Aδ and C fibres), which are small and unmyelinated or lightly myelinated, have shorter internodal distances and are blocked preferentially at lower concentrations than large motor fibres — this is why LAs produce differential block (pain relieved before touch, touch before motor, motor last).
Pathophysiology of Pain Transmission and Na⁺ Channel Physiology
The nociceptive pathway begins at peripheral nociceptors (free nerve endings in skin, muscle, viscera) that transduce thermal, mechanical, or chemical stimuli into electrical signals. These signals travel along Aδ fibres (thinly myelinated, 1–5 μm, 5–30 m/s — fast sharp pain) and C fibres (unmyelinated, <1 μm, 0.5–2 m/s — slow burning aching pain). Both fibre types converge on the dorsal horn of the spinal cord and relay nociceptive signals rostrally via the spinothalamic tract.
At the cellular level, pain transmission depends on the generation and propagation of action potentials, which require functional voltage-gated Na⁺ channels. The three-state model of the channel is critical for understanding LA pharmacology:
- Resting state: channel closed, membrane at −70 mV. Na⁺ cannot flow.
- Open/activated state: membrane depolarises → S4 voltage sensor moves → pore opens → Na⁺ rushes in → depolarisation propagates. Duration: ~1 ms.
- Inactivated state: after rapid depolarisation, the inactivation gate (loop between domains III and IV) occludes the pore. Channel is closed and non-conducting. Returns to resting state on repolarisation.
LA mechanism: state-dependent blockade
Local anaesthetics are weak bases (pKa 7.5–9.5). At physiological pH (7.4), both ionised (BH⁺, quaternary form) and unionised (B, tertiary amine form) fractions exist. The pharmacokinetics at the tissue level follow a two-step model:
1. The unionised (lipophilic) form crosses the axonal membrane (phospholipid bilayer).
2. Once inside, re-ionisation to BH⁺ occurs (intracellular pH ~7.2 → slightly more ionised); this ionised form enters and blocks the open/inactivated Na⁺ channel from the cytoplasmic side (inner vestibule of S6 pore).
LA preferentially stabilises the inactivated state → prevents transition back to resting → channel cannot be reactivated. Use-dependent block: channels that open and inactivate more frequently (high-frequency firing — pain fibres > motor fibres) are more readily blocked. This is why small, high-frequency C fibres lose pain sensation before large, low-frequency motor fibres lose motor function.
Differential nerve block order (from most to least sensitive at equimolar LA concentration):
Small unmyelinated C fibres (pain, temperature, autonomic) → small myelinated Aδ fibres (fast pain, cold) → medium Aβ fibres (touch, pressure) → large Aα motor fibres (proprioception, motor) — LAST.
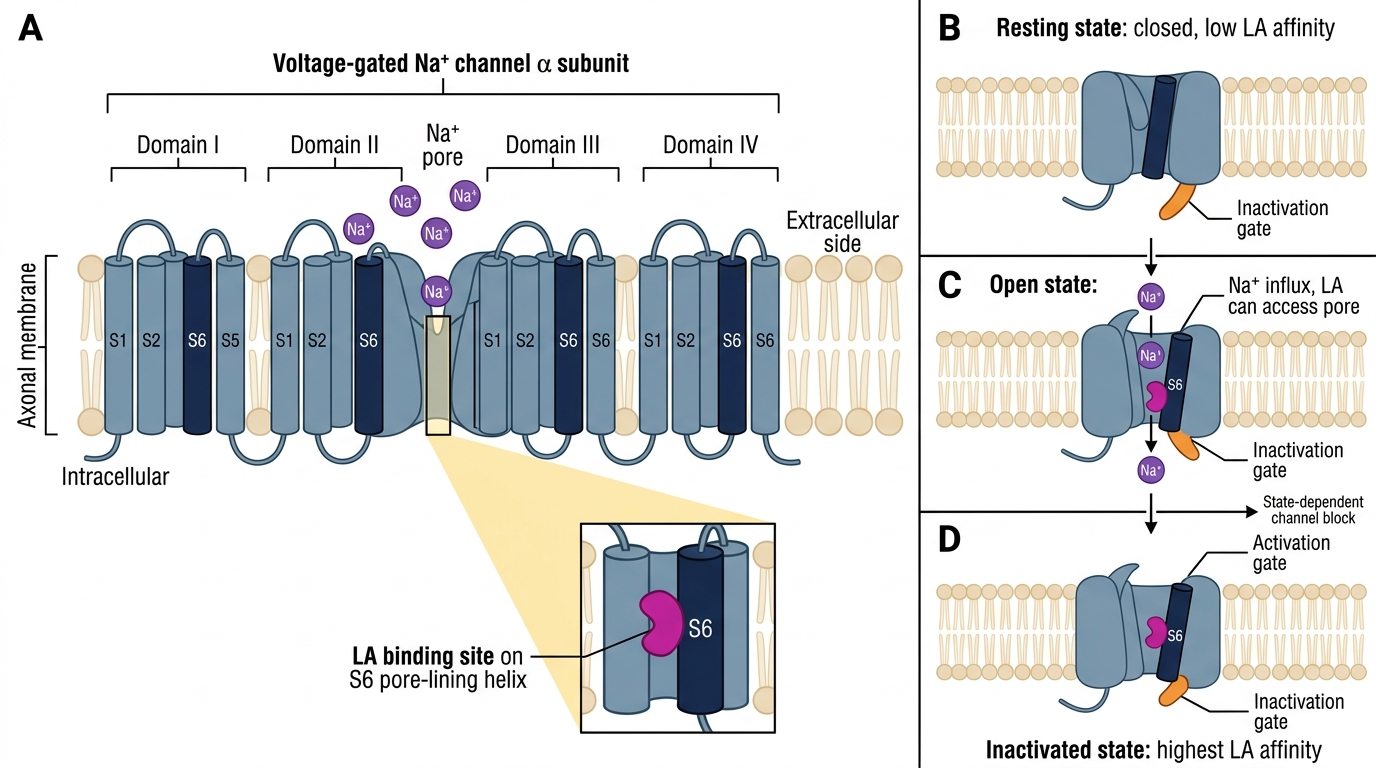
State-Dependent Local Anaesthetic Block of Voltage-Gated Na+ Channels
SELF-CHECK
A patient with an infected finger (abscess, pH ~6.0 due to local acidosis) receives lignocaine infiltration but achieves minimal pain relief. What is the pharmacokinetic explanation?
A. Infected tissue has increased Na⁺ channel density, requiring more drug to achieve blockade
B. At pH 6.0, the equilibrium shifts toward the ionised (BH⁺) form of lignocaine; less unionised drug is available to penetrate the axonal membrane, reducing intracellular concentration and block
C. Lignocaine is inactivated by bacterial toxins in infected tissue
D. Inflammation causes up-regulation of LA metabolism by local esterases
Reveal Answer
Answer: B. At pH 6.0, the equilibrium shifts toward the ionised (BH⁺) form of lignocaine; less unionised drug is available to penetrate the axonal membrane, reducing intracellular concentration and block
Local anaesthetics exist as a pH-dependent equilibrium between ionised (BH⁺) and unionised (B) forms, governed by the Henderson-Hasselbalch equation. The unionised form is lipophilic and penetrates the nerve membrane. At low pH (infected/inflamed tissue, pH ~6.0), the equilibrium shifts strongly toward the ionised form — far less unionised LA is available to diffuse through the axonal membrane. The result is a dramatically reduced effective concentration of drug inside the axon and a markedly inferior nerve block. This is a well-established clinical phenomenon; strategies include increasing the LA dose (with toxicity awareness), using carbonated LA preparations, or supplementing with nerve block rather than infiltration.
Therapeutic Rationale for Local Anaesthesia
The fundamental rationale for local anaesthesia is to interrupt nociceptive transmission at a discrete anatomical location — preventing the pain signal from reaching consciousness without altering the patient's state of awareness. This approach offers several pharmacological advantages over general anaesthesia: preservation of airway reflexes, avoidance of systemic opioid effects, reduced nausea/vomiting, earlier ambulation, and superior post-operative analgesia when used as part of a multimodal regimen.
Key therapeutic goals matched to clinical settings:
- Surgical analgesia without general anaesthesia: minor surgery (skin repair, dental extraction, circumcision), day-case surgery (peripheral limb procedures), and high-risk patients for whom general anaesthesia carries unacceptable risk.
- Regional anaesthesia: provides complete sensorimotor block of a body region — allows major surgery (hip replacement, lower limb orthopaedic, caesarean section) while the patient remains awake, reducing general anaesthesia risks.
- Obstetric pain relief: epidural bupivacaine (with an opioid) is the gold standard for labour analgesia — achieves pain relief without motor block at the low concentrations used (0.0625–0.1% bupivacaine).
- Post-operative analgesia: continuous peripheral nerve block catheters (e.g. femoral nerve catheter for hip arthroplasty) or wound infiltration catheters reduce opioid requirements by 30–60% in multimodal analgesia protocols.
- Antiarrhythmic therapy: lignocaine (lidocaine) is a Class 1b antiarrhythmic — its Na⁺ channel blocking action on Purkinje fibres and ventricular myocardium suppresses ventricular ectopy and was formerly used IV for VT (now largely replaced by amiodarone but retained in some ACLS protocols).
- Diagnostic and therapeutic nerve blocks: used in chronic pain management to identify the source of pain (diagnostic block) or provide temporary relief (therapeutic).
Classification of Local Anaesthetics
Local anaesthetics are classified by the chemical linkage between their aromatic ring and the amine group. This structural distinction is clinically important because it determines the metabolic pathway, allergy risk, and pharmacokinetic properties.
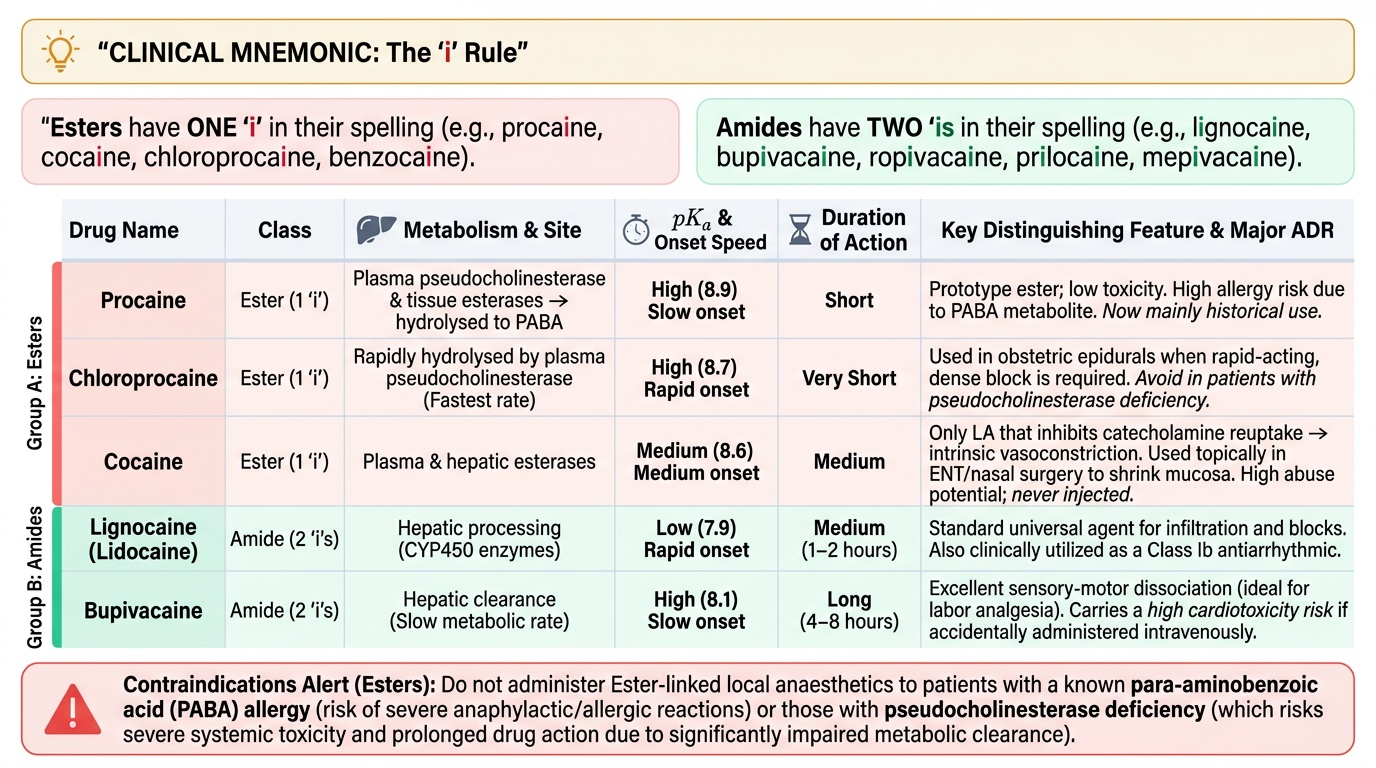
Mnemonic: Amides have TWO 'i's in their name before '-caine' (lignocaine, bupivacaine, ropivacaine, prilocaine, mepivacaine); esters have ONE (procaine, cocaine, chloroprocaine, benzocaine).
Class 1: Ester-linked local anaesthetics
Metabolised by plasma pseudocholinesterase (butyrylcholinesterase) and tissue esterases. Rapid hydrolysis → shorter duration generally. Major metabolite from procaine/chloroprocaine: para-aminobenzoic acid (PABA) — PABA-based metabolites are responsible for the higher incidence of allergic reactions to ester LAs. Esters should not be used in patients with pseudocholinesterase deficiency (prolonged action) or known PABA allergy.
- Procaine: prototype ester; short duration; now mainly of historical significance (infiltration, spinal for short procedures). Low toxicity.
- Chloroprocaine: rapid onset, very short duration (hydrolysed fastest of all LAs); used for obstetric epidural when rapid dense block is needed.
- Cocaine: the only LA that also inhibits catecholamine reuptake → vasoconstriction. Used topically in ENT surgery (nasal mucosa — shrinks mucosa + provides LA). Abuse potential; not used for injection.
- Benzocaine: poorly water-soluble, not suitable for injection. Used as topical spray (throat, skin). Risk of methaemoglobinaemia in high doses — methylene blue antidote.
Class 2: Amide-linked local anaesthetics
Metabolised by hepatic CYP450 enzymes (reduced clearance in hepatic impairment). More stable, longer shelf life. True allergy is rare (no PABA metabolite). Generally preferred in clinical practice.
- Lignocaine (lidocaine): intermediate duration prototype amide; fastest onset among amides (low pKa = 7.9 → relatively more unionised at pH 7.4 → faster membrane penetration). Also Class 1b antiarrhythmic (IV). Most versatile: topical, infiltration, nerve block, IV regional, epidural, spinal, antiarrhythmic.
- Bupivacaine: long-acting amide; high protein binding (95%) and high lipid solubility → prolonged duration. High cardiac toxicity risk — binds cardiac Na⁺ and Ca²⁺ channels with greater affinity and longer duration than lignocaine; bupivacaine-induced cardiac arrest can be refractory to standard resuscitation (reason: lipid-soluble drug partitions into cardiac tissue, difficult to displace). Preferred for epidural (labour analgesia, surgical), spinal (heavy/hyperbaric for surgical), and long peripheral nerve blocks.
- Ropivacaine: long-acting amide similar to bupivacaine but with less cardiac toxicity (lower lipid solubility than bupivacaine → less cardiac uptake; also has intrinsic vasoconstriction reducing systemic absorption). Preferred for epidural analgesia (continuous infusion) and major peripheral nerve blocks where long duration is needed with a better safety margin.
- Prilocaine: amide; metabolised to o-toluidine → oxidises haemoglobin → methaemoglobinaemia. Limit dose to <600 mg in adults; avoid in infants (limited metHb reductase), sickle cell disease, G6PD deficiency. Used in EMLA cream (eutectic mixture with lignocaine — topical for children).
Provided image
SELF-CHECK
A surgeon plans a long peripheral nerve block for a below-knee orthopaedic procedure expected to last 3–4 hours, in a patient with known severe liver cirrhosis. Which LA is most appropriate?
A. Bupivacaine — longest duration, suitable for long procedures
B. Ropivacaine — long duration similar to bupivacaine; less cardiac toxicity; BUT amide metabolism is hepatic — reduced clearance in cirrhosis requires dose reduction and monitoring. Still preferred over bupivacaine for safety margin.
C. Procaine — ester, plasma hydrolysis, organ-independent — preferred in liver disease
D. Lignocaine — shortest amide; repeated top-ups possible; hepatic clearance is reduced in cirrhosis — accumulation risk
Reveal Answer
Answer: B. Ropivacaine — long duration similar to bupivacaine; less cardiac toxicity; BUT amide metabolism is hepatic — reduced clearance in cirrhosis requires dose reduction and monitoring. Still preferred over bupivacaine for safety margin.
Both bupivacaine and ropivacaine are amides requiring hepatic metabolism — both have reduced clearance in cirrhosis. However, ropivacaine's lower cardiac toxicity (less lipid solubility, less cardiac uptake) makes it the safer choice when the patient has hepatic impairment AND a long procedure requiring a potent long-acting LA. Dose reduction is appropriate in cirrhosis. Procaine is a short-acting ester unsuitable for a 3–4 hour procedure. The ester LA advantage (organ-independent hydrolysis) is real but does not help for long procedures. Lignocaine's intermediate duration would require multiple top-ups, increasing accumulation risk in cirrhosis.