Page 11 of 18
PH2.5 | PH2.5 | Local Anaesthetics and Administration Techniques — SDL Guide — SDL Guide (Part 2)
Pharmacokinetics, Pharmacodynamics, Uses, and Adverse Effects of Local Anaesthetics
The pharmacokinetic determinants of LA activity are pKa, protein binding, and lipid solubility. These three properties, together with the metabolic pathway, predict which agent to choose for which clinical need.
Three PK determinants:
| PK property | What it governs | Example |
|---|---|---|
| pKa | Onset speed — lower pKa → more unionised at pH 7.4 → faster membrane penetration | Lignocaine pKa 7.9: ~25% unionised at pH 7.4 → fast onset. Bupivacaine pKa 8.1: ~15% unionised → slower onset. |
| Protein binding | Duration — higher protein binding → drug stays bound in tissue → slower redistribution | Bupivacaine 95% protein-bound → long duration (4–8h). Lignocaine 65% → intermediate duration (1–2h). |
| Lipid solubility | Potency (lower concentration needed) AND cardiac toxicity (greater CNS/cardiac partitioning) | Bupivacaine: highly lipid soluble → very potent AND cardiotoxic. |
Maximum doses (critical for safe clinical use):
- Lignocaine: 3 mg/kg without adrenaline; 7 mg/kg with adrenaline (vasoconstriction slows systemic absorption → more drug can be safely used locally).
- Bupivacaine: 2 mg/kg (adult). NEVER use for IV regional anaesthesia (Bier's block) — if the tourniquet deflates prematurely, the high cardiac toxicity of bupivacaine can cause fatal cardiac arrest that is refractory to resuscitation.
- Ropivacaine: maximum dose not as tightly codified as bupivacaine; typically ≤3 mg/kg in clinical practice.
Systemic toxicity — LA systemic absorption causing CNS and cardiac effects:
Systemic toxicity occurs when blood concentrations rise above the threshold for Na⁺ channel blockade in excitable tissues outside the target nerve:
- CNS toxicity (earlier, at lower plasma concentration): Circumoral numbness and tingling → tinnitus (the earliest symptom) → visual disturbances, metallic taste → seizures (paradoxically caused by excitation — LA blocks inhibitory interneurons first, leaving excitatory circuits unopposed) → CNS depression, coma, respiratory arrest.
- Cardiac toxicity (higher plasma concentration): Na⁺ channel block in cardiac conduction system → PR prolongation → QRS widening → bradycardia → VF/PEA → cardiac arrest. Bupivacaine binds cardiac Na⁺ channels with slower rate of recovery ('fast in, slow out') — meaning bupivacaine-induced cardiac arrest is resistant to standard resuscitation protocols; standard ACLS may not work.
Treatment of LA systemic toxicity:
1. Stop injection immediately. Call for help.
2. Airway: high-flow O₂, intubate if needed.
3. Seizures: benzodiazepine (diazepam/midazolam) or propofol (small doses).
4. Cardiac arrest: ACLS — prolonged CPR may be required (bupivacaine dissociates slowly from cardiac Na⁺ channels).
5. Lipid emulsion rescue (Intralipid): 20% lipid emulsion 1.5 mL/kg IV bolus over 1 minute, then infusion 15 mL/kg/hour (AAGBI/ACLS protocol). Mechanism: lipid sink hypothesis — the large lipid phase created in plasma 'extracts' the lipophilic LA from cardiac tissue, reducing its effective cardiac concentration. Evidence from animal models and case reports (no RCT — ethical impossibility). Should be available wherever bupivacaine is used.
Allergy:
- Esters → PABA metabolite → more common allergic reactions (rash, urticaria, anaphylaxis). Cross-reactivity between esters is likely.
- Amides → true allergy is rare. Most 'amide allergy' is either a vasovagal reaction to injection, allergy to the preservative (methylparaben — structurally similar to PABA), or misattributed adrenaline effects (palpitations).
SELF-CHECK
A 70 kg patient undergoing a femoral nerve block receives 20 mL of 1% lignocaine WITH adrenaline. Is this within the safe maximum dose?
A. No — 1% lignocaine is too high a concentration for nerve blocks, regardless of dose
B. Yes — 20 mL of 1% lignocaine = 200 mg. Maximum dose with adrenaline = 7 mg/kg × 70 kg = 490 mg. 200 mg is well within the safe limit.
C. No — 200 mg exceeds the 3 mg/kg limit (210 mg for 70 kg)
D. Yes, but only if given slowly — the rate of injection determines toxicity more than total dose
Reveal Answer
Answer: B. Yes — 20 mL of 1% lignocaine = 200 mg. Maximum dose with adrenaline = 7 mg/kg × 70 kg = 490 mg. 200 mg is well within the safe limit.
1% lignocaine = 10 mg/mL. 20 mL × 10 mg/mL = 200 mg. The maximum dose of lignocaine WITH adrenaline is 7 mg/kg: 7 × 70 = 490 mg. 200 mg is well within the safe limit. The 3 mg/kg limit (= 210 mg for 70 kg) applies WITHOUT adrenaline. With adrenaline, the vasoconstriction slows systemic absorption, allowing a higher total dose. This calculation is a high-yield exam question that tests knowledge of the dose-limit difference between plain and adrenaline-containing formulations.
Administration Techniques and Methods of LA Administration
The clinical effectiveness and safety of local anaesthesia depend as much on correct administration technique as on the drug itself. The competency PH2.5 explicitly requires the ability to demonstrate methods of LA administration — knowing which technique to use for which clinical context is the applied pharmacological skill.
Method 1: Topical application
The LA is applied directly to mucous membranes or skin. Absorption is site-dependent: nasal/pharyngeal mucosa absorbs rapidly (near-IV kinetics for some agents); skin requires an occluded patch (EMLA — eutectic mixture of lignocaine and prilocaine, 2.5% each) for 45–60 minutes to penetrate intact skin. Uses: throat spray before endoscopy, urethral gel before catheterisation, EMLA cream before IV insertion in children, cocaine/lignocaine spray for nasal endoscopy.
Method 2: Local infiltration
The LA is injected directly into the tissue at and around the surgical site, blocking nerve endings in situ. The simplest technique — suitable for skin closure, wound repair, and minor excisions. Inject slowly, in a fan distribution, aspirating before each injection to avoid intravascular placement. Risk: total dose exceeded if large areas are infiltrated.
Method 3: Peripheral nerve block
The LA is deposited near a named peripheral nerve or nerve plexus (e.g. brachial plexus block for arm surgery, femoral nerve block for knee surgery, sciatic nerve block for foot surgery). Ultrasound guidance has transformed this technique — real-time needle visualisation reduces the risk of intravascular injection, intraneural injection, and block failure. Drugs of choice: lignocaine (intermediate duration), bupivacaine or ropivacaine (long duration).
Method 4: IV regional anaesthesia (Bier's block)
LA is injected intravenously into an exsanguinated limb maintained bloodless by a proximal tourniquet. The LA distributes along the vascular tree to reach nerves throughout the limb. Drug of choice: lignocaine 0.5%, up to 3 mg/kg. The tourniquet MUST remain inflated for ≥20 minutes. NEVER use bupivacaine for Bier's block — if the tourniquet deflates prematurely, systemic bupivacaine causes rapid, refractory cardiac arrest. Suitable for forearm and hand procedures lasting <90 minutes.
Method 5: Epidural anaesthesia
The LA is injected into the epidural space (between the ligamentum flavum and the dura mater), blocking nerve roots as they exit the spinal cord. A catheter can be left in place for continuous infusion. Standard technique for obstetric analgesia (0.0625–0.1% bupivacaine + opioid = dense analgesia with minimal motor block), and for thoracoabdominal surgical analgesia and post-operative pain. The epidural space is a potential space — correct placement is confirmed by the loss of resistance technique (to saline or air). Complications: hypotension (sympathetic block), dural puncture (postdural puncture headache), motor block, epidural haematoma (rare but serious).
Method 6: Spinal (intrathecal) anaesthesia
The LA is injected into the subarachnoid space (CSF), producing immediate and dense block. Typically performed at L3/L4 or L4/L5 interspace (below the spinal cord termination at L1–L2 in adults). Drug of choice: hyperbaric (heavy) bupivacaine 0.5% in 8% dextrose (density >CSF — sinks to dependent areas → block is position-dependent). Uses: lower limb and pelvic surgery, caesarean section (most common), transurethral procedures. Onset: 3–5 minutes. Duration: 2–3 hours depending on dose. Complications: hypotension (sympathetic block), high/total spinal (respiratory arrest if block ascends to upper thoracic/cervical level), post-dural puncture headache.
Additives to LA solutions:
- Adrenaline (1:200,000 = 5 mcg/mL): α1-mediated local vasoconstriction → reduces systemic absorption → prolongs duration of block → reduces bleeding → increases maximum safe LA dose. Contraindicated in end-artery tissues: digits (fingers, toes), nose, penis, ears — ischaemia and gangrene can result.
- Opioids (fentanyl, morphine added to epidural/spinal): synergistic analgesia at spinal opioid receptors → allows lower LA dose → reduces motor block.
- Clonidine (α2 agonist): prolongs peripheral nerve block duration by ~2 hours via hyperpolarisation of sensory neurones and local vasoconstriction.
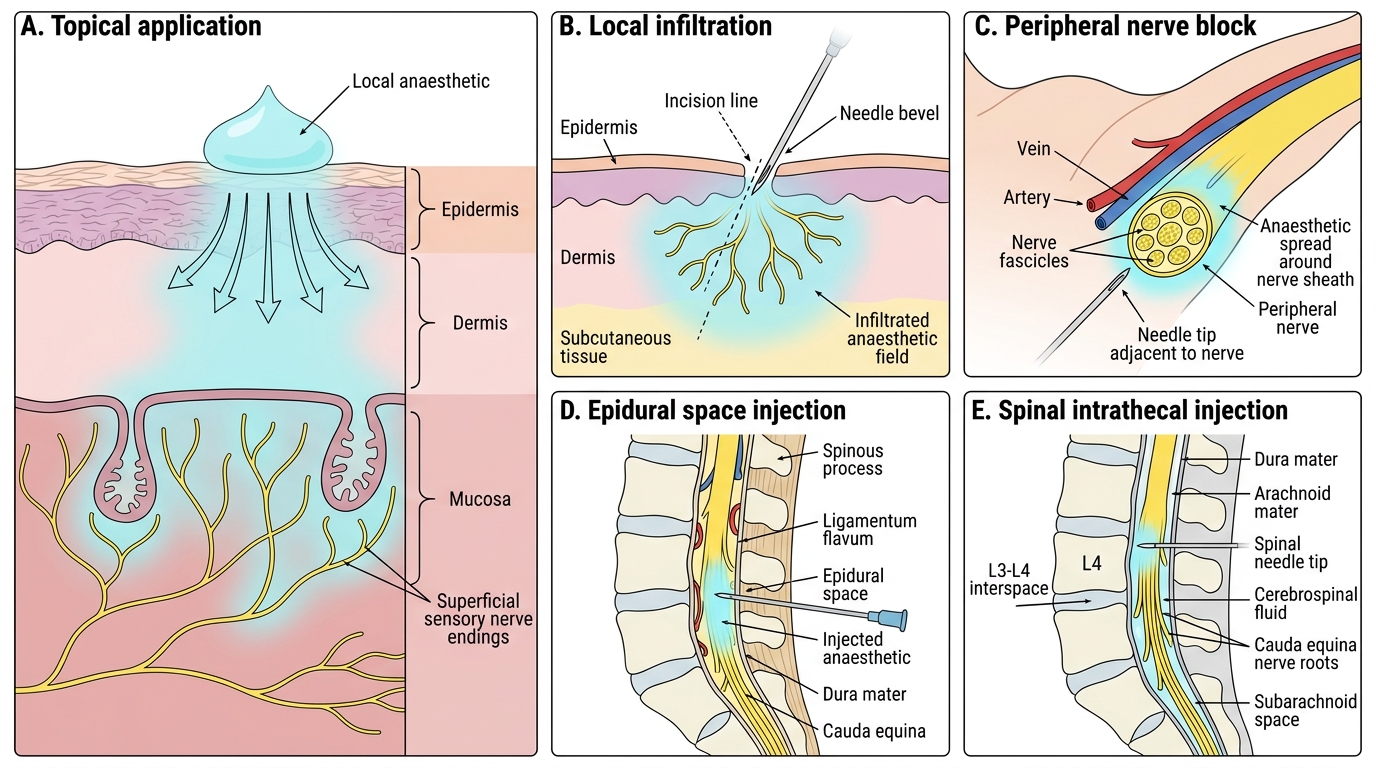
Methods of Local Anaesthetic Administration
SELF-CHECK
An orthopaedic surgeon wants to use IV regional anaesthesia (Bier's block) for a 45-minute carpal tunnel release on a 60 kg patient. She asks if she can use bupivacaine 0.5% for a longer-lasting block. What is your response?
A. Yes — 0.5% bupivacaine at 3 mg/kg is within the safe dose range for Bier's block
B. No — bupivacaine must NEVER be used for Bier's block; if the tourniquet deflates prematurely, systemic bupivacaine causes rapid, refractory cardiac arrest; use lignocaine 0.5% instead
C. Yes — as long as the tourniquet is kept inflated for at least 30 minutes, the systemic release will be safe
D. No — bupivacaine cannot be used in an IV solution; it is only safe for infiltration
Reveal Answer
Answer: B. No — bupivacaine must NEVER be used for Bier's block; if the tourniquet deflates prematurely, systemic bupivacaine causes rapid, refractory cardiac arrest; use lignocaine 0.5% instead
Bupivacaine is absolutely contraindicated for IV regional anaesthesia (Bier's block). This is one of the most emphatic contraindications in all of anaesthetic pharmacology: the high cardiac toxicity of bupivacaine means that even a brief early tourniquet deflation (or tourniquet failure) releases bupivacaine systemically, causing cardiac arrhythmias and cardiac arrest that may be refractory to standard resuscitation. Multiple fatal cases have been documented. Lignocaine 0.5% (plain, no adrenaline — 3 mg/kg) is the only LA approved for Bier's block. For a 60 kg patient: maximum dose = 3 × 60 = 180 mg = 36 mL of 0.5% lignocaine.
CLINICAL PEARL
Lipid emulsion rescue for LA toxicity — have it ready wherever bupivacaine is used: The AAGBI (Association of Anaesthetists) and international resuscitation guidelines recommend that 20% lipid emulsion (Intralipid) must be immediately available in any location where bupivacaine or ropivacaine is administered. The 'lipid sink' mechanism — where an intravenous lipid phase extracts the lipid-soluble LA from cardiac tissue — can reverse otherwise-fatal cardiac arrest. Dose: 1.5 mL/kg IV bolus over 1 minute, followed by 15 mL/kg/hour infusion; repeat bolus if cardiac arrest recurs. Continue CPR during administration — bupivacaine will eventually dissociate from cardiac channels, and a heart that is adequately oxygenated via CPR during that window can be recovered. The lesson: the same high lipid solubility that makes bupivacaine so clinically effective (potent, long-lasting) is the property that makes its systemic toxicity so dangerous — and lipid emulsion exploits exactly that property to rescue the patient.
Second pearl — the 'NO ADRENALINE' rule for end-arteries: The mnemonic taught in clinical skills is 'PENIS' — Digits (fingers), Ear pinna, Nose, Intraocular, Scalp end-artery zones... or more practically: never add adrenaline to any LA injected around fingers, toes, nose tip, penis, or pinna. α1-mediated vasoconstriction in a terminal arterial distribution causes tissue ischaemia and potentially digital gangrene. The benefit of prolonged duration and reduced bleeding does NOT outweigh this risk in these anatomical sites.