Page 16 of 30
PH10.{5,11-12} | PH10.{5,11-12} | Legal, Ethical and Regulatory Frameworks for Drug Use — SDL Guide — SDL Guide
Learning Objectives
- Identify and apply the legal and ethical regulations governing prescribing in India, including requirements for controlled drugs, off-label medicines, and prescribing for self or close family
- Describe the phases of clinical drug development and the principles of Good Clinical Practice
- Reflect on the role of research in developing new drugs and the ethical obligations of the prescriber and researcher
INSTRUCTIONS
Every drug you prescribe exists because a regulatory authority determined it was safe and effective enough for clinical use — and the conditions under which you prescribe it are shaped by a framework of laws, regulations, and ethical standards. Understanding this framework is not a bureaucratic exercise: the thalidomide disaster of the 1960s, the Bhopal-linked regulatory failures, and contemporary challenges with opioid overprescribing all illustrate what happens when this framework is absent or ignored. This module equips you to navigate drug regulations, prescribe controlled medicines safely and legally, and understand both the rigour and the ethical obligations of clinical drug development.
References
- Drugs and Cosmetics Act 1940 (India) — including Schedules H, H1, X (legislation)
- ICMR National Ethical Guidelines for Biomedical and Health Research Involving Human Participants, 2017 (guideline)
- ICH E6(R2) Good Clinical Practice Guideline (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are a junior resident at a busy medicine ward. A patient's relative — also a doctor — calls asking if you can prescribe him some diazepam (a benzodiazepine, Schedule X drug) for 'anxiety while travelling.' He is your senior colleague and you feel social pressure to help. Meanwhile, another patient's family member asks you about a drug you have never heard of — it was recommended by an oncologist in another city for off-label use in a non-cancer condition. How do you handle both situations — legally and ethically?
WHY THIS MATTERS
The regulatory framework governing drugs is not abstract bureaucracy — it is the accumulated response to disasters, abuses, and ethical failures that occurred when drugs were available without oversight. In India, cases of irrational antibiotic prescribing contributing to antimicrobial resistance, illegal clinical trials conducted without proper informed consent (the Indore trial scandal, 2012), and unregulated OTC availability of antibiotics and steroids are all direct consequences of regulatory gaps. As a prescriber, you operate within this framework: you have a legal duty to follow it and an ethical obligation to uphold it even when it is inconvenient. The NMC's professional code of conduct links regulatory compliance directly to medical registration.
RECALL
Recall from your pharmacology foundation year that drugs in India are classified under the Drugs and Cosmetics Act 1940 into categories based on prescription requirement and abuse potential. You have encountered Schedule H (requiring a physician's prescription) and likely heard of Schedule X (narcotics, psychotropics) requiring special prescription formats. Recall also from the rational prescribing SDL that the prescriber's registration number is a mandatory legal element of prescriptions for Schedule H and X drugs — it allows regulatory traceability of every prescription written.
The Legal Framework: Why Drug Regulation Exists
Drug regulation is one of the most consequential applications of public health law. The principle that a pharmaceutical product must be proven safe and effective before being marketed — seemingly obvious today — was established largely in response to catastrophic failures that occurred in the absence of such requirements.
The most instructive historical example is the thalidomide disaster (1957–1961). Thalidomide was marketed as a safe sedative and treatment for morning sickness in pregnancy. It had not been tested for teratogenicity. Approximately 10,000 children were born with severe limb malformations (phocomelia) before the drug was withdrawn. The disaster directly triggered major regulatory reforms — in the United States, the Kefauver-Harris Amendment (1962) required proof of efficacy and safety before drug approval; in Europe and India, similar strengthening occurred.
In India, the primary legislation governing drugs is the Drugs and Cosmetics Act 1940, which has been amended multiple times. Its key provisions include: requirements for manufacturing quality and licensing; prescription requirements for scheduled drugs; import and export controls; clinical trial regulations; and the establishment of the Central Drugs Standard Control Organisation (CDSCO) as the national drug regulatory authority. The CDSCO is equivalent in function to the FDA (United States) or EMA (European Union) — it approves new drugs for marketing, monitors drug safety post-marketing, regulates clinical trials, and maintains the list of approved drugs.
At the state level, State Drug Controllers work alongside CDSCO to implement the Act. The Pharmacy Act 1948 regulates the practice of pharmacy and the qualifications required to dispense drugs — it complements the Drugs and Cosmetics Act by regulating the dispensing side of the supply chain.
Drug Regulation in India: Key Acts, Schedules, and CDSCO
Understanding the specific drug schedules and the regulatory infrastructure they rest on is essential for compliant and safe prescribing. The key elements of India's drug regulatory framework relevant to prescribers are:
Drug Schedules:
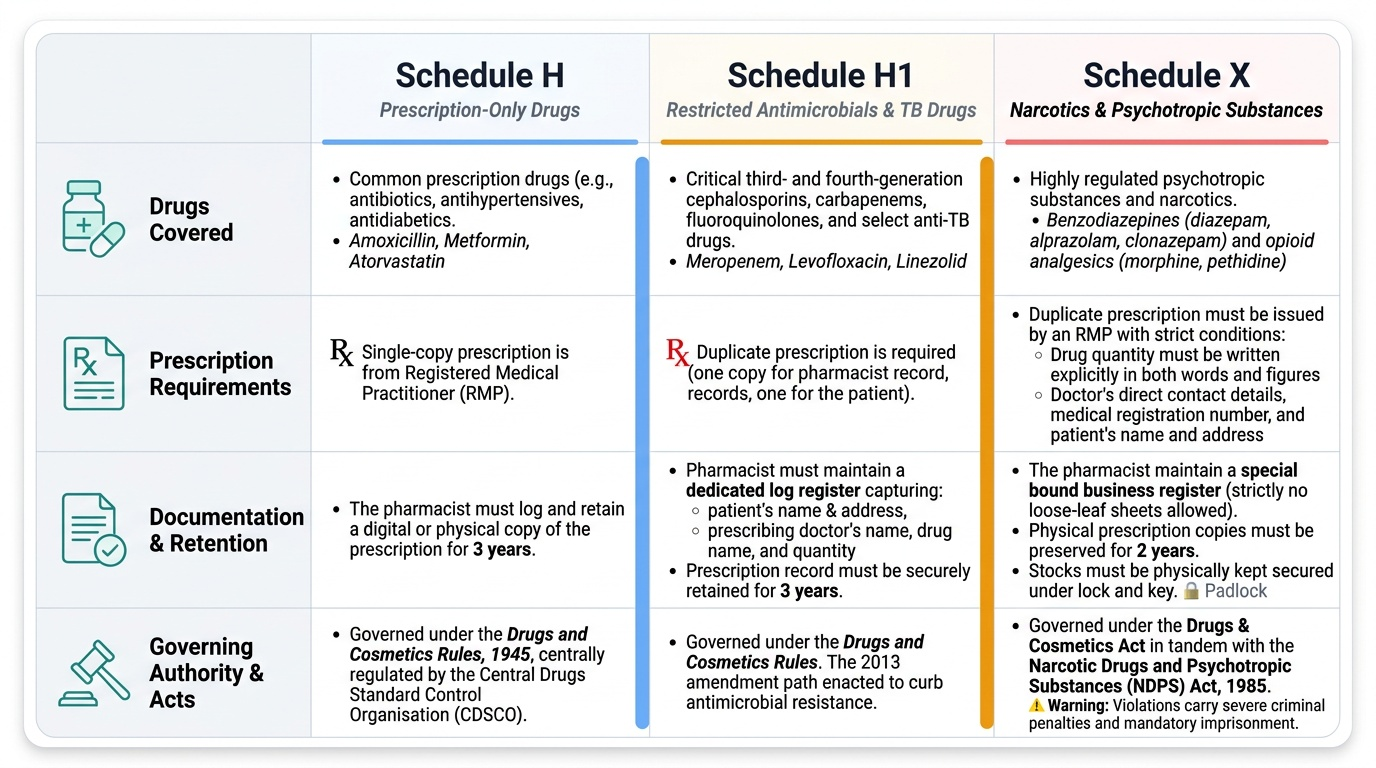
- Schedule H: Drugs that can only be supplied on a prescription from a registered medical practitioner. The pharmacist must retain a copy for 3 years. Most common prescription drugs (antibiotics, antihypertensives, antidiabetics) fall under Schedule H.
- Schedule H1: A stricter sub-category of Schedule H, introduced in 2013 primarily to address antimicrobial resistance. Includes specific third- and fourth-generation cephalosporins, carbapenems, fluoroquinolones, and other critical antimicrobials. Prescriptions must be in duplicate; the pharmacist keeps one copy for 3 years; stricter documentation required.
- Schedule X: Psychotropic substances and certain narcotics under the NDPS Act (Narcotic Drugs and Psychotropic Substances Act 1985) and the Drugs and Cosmetics Act. Requires: prescription in duplicate; quantity stated in words; prescriber's details and registration number; patient's name and address; pharmacist retains copy for 2 years. Examples: benzodiazepines (diazepam, alprazolam, clonazepam), opioid analgesics (morphine, pethidine), and other listed psychotropics.
DPCO (Drug Price Control Order): Issued under the Essential Commodities Act, the DPCO caps the maximum retail price of drugs listed in the NLEM. NPPA (National Pharmaceutical Pricing Authority) implements this.
NDPS Act 1985: Governs narcotic drugs and psychotropic substances. Creates a separate, stricter regulatory layer for Schedule X drugs with criminal penalties for violations.
Provided image
SELF-CHECK
A patient presents with severe cancer pain and requires oral morphine (an opioid — Schedule X). His family asks you to give a 3-month supply at once to avoid repeated visits. Which legal requirement for Schedule X prescriptions makes this request complicated?
A. A) Schedule X prescriptions cannot be issued for cancer patients — palliative care is a special exemption
B. B) Schedule X prescriptions must state quantity in words and are subject to a maximum quantity per prescription under state narcotic rules; a 3-month supply may exceed the permitted single-prescription quantity in some states
C. C) Morphine is no longer Schedule X — it was reclassified as Schedule H in 2021
D. D) Schedule X prescriptions can only be written by oncologists — general physicians cannot prescribe morphine
Reveal Answer
Answer: B. B) Schedule X prescriptions must state quantity in words and are subject to a maximum quantity per prescription under state narcotic rules; a 3-month supply may exceed the permitted single-prescription quantity in some states
B is correct. Schedule X (NDPS Act) prescriptions for opioids such as morphine require quantity in words, and most state narcotic rules limit the quantity that can be prescribed on a single prescription — often to a 1-month supply or less, depending on the state's rules under the NDPS Act. The prescriber must issue separate prescriptions for each dispensing period. Option A is incorrect: palliative care prescriptions are regulated but not prohibited. Option C is false: morphine remains a Schedule X / NDPS substance. Option D is incorrect: registered medical practitioners can prescribe morphine for bona fide therapeutic purposes.
Ethical Prescribing: Controlled Drugs, Off-Label Use, and Self-Prescribing
Legal compliance is the floor of prescribing conduct — ethical practice requires more. Three specific prescribing scenarios require both legal and ethical analysis: controlled drug prescribing, off-label use, and prescribing for oneself or close family.
Prescribing controlled drugs (Schedule X):
The legal requirements are clear: specific prescription format, quantity in words, patient identity documented. The ethical obligations go further: the prescriber must make an independent clinical assessment and have a documented therapeutic rationale. Prescribing controlled substances to someone you have not properly assessed — including a colleague who calls and asks for benzodiazepines — is both legally and ethically problematic. The risk of facilitating substance misuse is real; benzodiazepine dependence in healthcare workers is a documented occupational risk.
Off-label prescribing:
'Off-label' refers to prescribing a drug outside its approved indication, dose, route, or patient population. Off-label prescribing is not prohibited by the Drugs and Cosmetics Act — it is a common medical practice (oncology, paediatrics, and psychiatry all involve high proportions of off-label use, because drug approval often lags evidence). However, the ethical obligations are significant:
1. There should be a reasonable evidence base for the off-label use (published literature, expert guidelines)
2. The patient must be informed that the use is off-label — informed consent documentation is required
3. The clinical reasoning should be documented in the medical record
4. The prescriber bears additional responsibility for monitoring since post-marketing safety data for the off-label indication may be limited
Self-prescribing and prescribing for close family:
The NMC's code of professional conduct and the general medical ethics literature are clear: prescribing for oneself or close family members is strongly discouraged except in genuine emergencies when no other physician is available. The reasons are:
- Objectivity is compromised: personal emotional involvement impairs clinical judgment
- Examination is inadequate: self-examination and examination of family members lacks the objectivity of a third-party clinical assessment
- Risk of enabling self-medication with prescription or controlled substances
- In India, self-prescribing of controlled substances is particularly problematic — it creates an audit trail that may invite regulatory scrutiny and NMC disciplinary action
In practice, every doctor should have their own registered general practitioner for personal healthcare — using the healthcare system appropriately is both an ethical obligation and a self-care practice.