Page 10 of 30
PH10.7 | PH10.7 | Pharmacogenomics and Pharmacoeconomics in Drug Choice — SDL Guide — SDL Guide
Learning Objectives
- Describe how pharmacogenomic variation (CYP450 polymorphisms, HLA alleles, enzyme deficiencies) affects drug response and prescribing decisions
- Explain the four types of pharmacoeconomic analysis and their outcome metrics
- Apply pharmacoeconomic reasoning to find and compare the price of given medications using available resources
INSTRUCTIONS
Two patients receive the same drug at the same dose — one achieves the target effect, one has a toxicity reaction, and a third has no effect at all. Why? Pharmacogenomics provides one answer: genetic variation in drug-metabolising enzymes, transporters, and drug targets creates measurable differences in individual drug response. Pharmacoeconomics provides a complementary lens: even when two drugs produce equivalent outcomes, they may differ substantially in cost — and the difference matters to patients, healthcare systems, and equity. This module integrates both frameworks into the applied skill of personalising drug selection.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 2 (Pharmacogenomics) and Ch 4 (Pharmacoeconomics) (textbook)
- Clinical Pharmacogenomics Implementation Consortium (CPIC) Guidelines — cpicpgx.org (guideline)
- Jan Aushadhi Portal (India) — janaushadhi.gov.in for generic drug pricing (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients on a rheumatology ward are both started on azathioprine for autoimmune disease. Within three weeks, one patient develops severe pancytopenia requiring hospital admission — the other is fine on the same dose. Your registrar mentions that this patient 'probably has TPMT deficiency.' What is TPMT, why does it matter, and how could this reaction have been anticipated and prevented? And while looking at the drug charts, you notice the hospital is purchasing branded azathioprine at five times the cost of the generic listed on the hospital formulary. Who pays the difference — and how do you find out?
WHY THIS MATTERS
The twin pillars of personalised medicine — pharmacogenomics and pharmacoeconomics — are no longer academic concepts. Regulatory agencies including the US FDA have added more than 200 pharmacogenomic annotations to drug labels, identifying variants that affect efficacy, safety, or dosing. In India, the relevance is acute: G6PD deficiency affects approximately 10% of some Indian populations, making G6PD screening before primaquine use a practical prescribing decision. At the same time, India's branded pharmaceutical market means that patients routinely pay 5–20 times the price of generic equivalents for the same molecule — and as a prescriber, you have the power to change this by knowing how to compare drug prices and choosing appropriately.
RECALL
Recall from your foundation pharmacology that drug metabolism in the liver primarily involves the CYP450 enzyme family — a superfamily of oxidases encoded by genes with significant inter-individual variation. You have also encountered the concept that some individuals are slow acetylators (e.g. for isoniazid) and others are fast acetylators, influencing drug levels and toxicity. These inter-individual differences in metabolism are now understood at the genetic level. Recall also that the P-drug framework includes cost as a selection criterion — this module equips you to operationalise that criterion quantitatively.
Why Patients Respond Differently to the Same Drug
Standard pharmacology teaching presents drug doses as producing predictable effects in an average patient — but clinical practice rapidly confronts this assumption. Individual variation in drug response is the rule, not the exception, and it arises from multiple sources: age, organ function, body composition, comedications, diet, and genetic background.
Genetic variation accounts for a substantial proportion of the variability that cannot be explained by these pharmacokinetic factors alone. Studies estimate that genetic factors account for 15–95% of the variability in the drug response of specific drugs — the range is wide because some drugs have highly polymorphic metabolism pathways while others do not.
The clinical consequences of ignoring this variability are not trivial. They include:
- Treatment failure in patients who are rapid or ultrarapid metabolisers of the active drug (the drug is cleared too quickly to reach therapeutic levels)
- Toxicity in patients who are poor metabolisers (drug accumulates to toxic concentrations at standard doses)
- Paradoxical responses in prodrug administration (e.g. clopidogrel requires CYP2C19 activation to become the active antiplatelet metabolite — poor metabolisers of CYP2C19 have reduced antiplatelet protection)
- Avoidable adverse drug reactions in patients with known pharmacogenomic risk variants (e.g. HLA-B*5701 carriers are at near-certain risk of abacavir hypersensitivity if pre-screening is not performed)
At the economic level, prescribing a drug without considering cost creates a parallel harm: patients who cannot afford the prescribed drug may take it incorrectly, share it with family members, or abandon treatment — all of which have direct clinical consequences.
Pharmacogenomics: Genetic Variation and Drug Response
Pharmacogenomics is the study of how an individual's genetic makeup affects their response to drugs — encompassing pharmacokinetic variation (absorption, distribution, metabolism, excretion) and pharmacodynamic variation (drug-target sensitivity). The dominant clinical application today is in drug metabolism, where the CYP450 enzyme system provides the most clinically actionable targets.
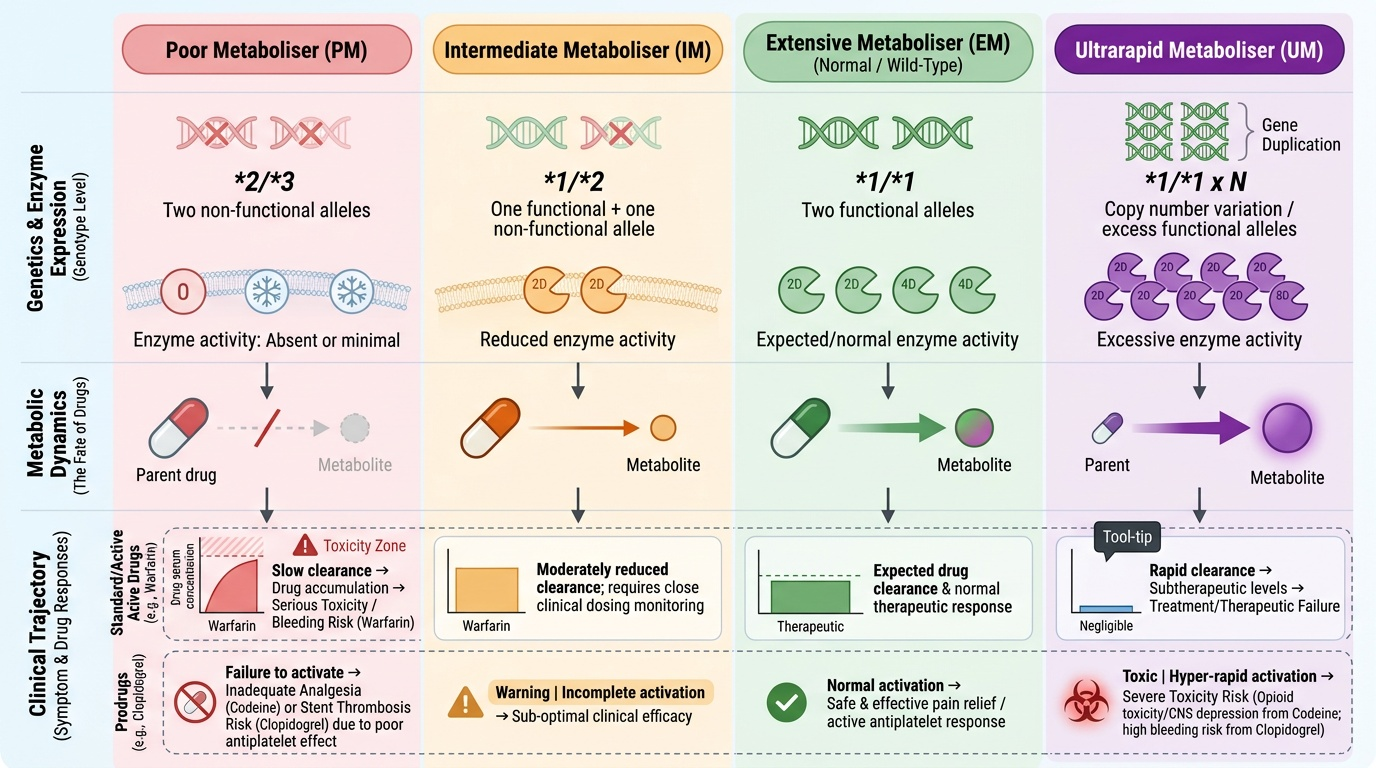
CYP450 metaboliser phenotypes:
Genes encoding CYP450 enzymes are highly polymorphic. Based on their combination of functional alleles, individuals are classified as:
- Poor metabolisers (PM): carry two non-functional alleles; enzyme activity is absent or minimal → drug accumulates → toxicity risk (for parent drugs); prodrugs may fail to be activated
- Intermediate metabolisers (IM): one functional + one non-functional allele; reduced enzyme activity
- Extensive metabolisers (EM): the 'normal' phenotype — two functional alleles; expected drug levels
- Ultrarapid metabolisers (UM): carry gene duplications producing excess enzyme activity → drug cleared too rapidly → therapeutic failure (for parent drugs); prodrugs converted too rapidly → toxicity from excess active metabolite
Clinically important CYP450 polymorphisms:
- CYP2D6: metabolises approximately 25% of all drugs — codeine (prodrug → morphine), tamoxifen (prodrug → endoxifen), many antidepressants (SSRIs, TCAs), beta-blockers (metoprolol, propranolol). PM phenotype: codeine → little morphine → inadequate analgesia. UM phenotype: codeine → rapid morphine → opioid toxicity (neonatal death cases in breastfeeding UM mothers led to FDA codeine warnings).
- CYP2C19: metabolises clopidogrel (prodrug), omeprazole, warfarin (partially), diazepam. PM phenotype: clopidogrel → reduced active metabolite → inadequate antiplatelet effect (increased stent thrombosis risk); UM phenotype: clopidogrel → excess active metabolite → higher bleeding risk.
- CYP2C9: warfarin metabolism; PM phenotype → warfarin accumulation → bleeding risk at standard doses
Non-CYP450 pharmacogenomic variants:
- TPMT (thiopurine S-methyltransferase): metabolises azathioprine and 6-mercaptopurine. TPMT deficiency (homozygous, ~1 in 300 individuals) → accumulation of thioguanine nucleotides → severe myelosuppression. TPMT genotyping before azathioprine initiation allows dose reduction or alternative immunosuppressant selection.
- G6PD deficiency: affects 10–30% of individuals in malaria-endemic populations including India. Oxidant drugs (primaquine, dapsone, nitrofurantoin, rasburicase) trigger haemolytic anaemia. G6PD screening before primaquine administration is standard practice in India's malaria programme.
- HLA alleles (pharmacogenomic immunotoxicology): HLA-B5701 is strongly associated with abacavir hypersensitivity reaction (HSR) — an immune-mediated, potentially fatal multi-organ reaction. Prospective HLA-B5701 screening before abacavir initiation (validated in the PREDICT-1 trial) has virtually eliminated abacavir HSR in screened populations.
Provided image
SELF-CHECK
A 35-year-old woman is prescribed clopidogrel after coronary stent placement. Pharmacogenomic testing reveals she is a CYP2C19 poor metaboliser. What is the PRIMARY clinical concern and the preferred management approach?
A. A) She will metabolise clopidogrel too rapidly, increasing her bleeding risk — reduce the dose
B. B) She will produce insufficient active clopidogrel metabolite — inadequate antiplatelet protection, with increased stent thrombosis risk — consider alternative antiplatelet such as ticagrelor or prasugrel
C. C) She will have increased omeprazole levels if concurrently prescribed — stop the PPI
D. D) CYP2C19 status does not affect clopidogrel response — no change needed
Reveal Answer
Answer: B. B) She will produce insufficient active clopidogrel metabolite — inadequate antiplatelet protection, with increased stent thrombosis risk — consider alternative antiplatelet such as ticagrelor or prasugrel
B is correct. Clopidogrel is a prodrug that requires CYP2C19 activation to form the active thiol metabolite that inhibits platelet ADP receptors. Poor metabolisers of CYP2C19 produce significantly less active metabolite, resulting in inadequate platelet inhibition and an increased risk of stent thrombosis. Current guidelines (ACC/AHA) recommend considering ticagrelor or prasugrel (which do not require CYP2C19 activation) in confirmed CYP2C19 PM patients after coronary stenting. Option A describes the ultrarapid metaboliser risk. CYP2C19 does affect omeprazole levels (PPIs), but this is a separate concern — not the primary issue here.
Pharmacogenomic Screening in Practice: When and How
Pharmacogenomic testing has moved from research laboratories into routine clinical practice for a defined set of drug-gene pairs where the clinical evidence for testing is strong and the test is actionable. Understanding when to request a test, how to interpret it, and how to adjust prescribing accordingly is the practical skill this section develops.
The Clinical Pharmacogenomics Implementation Consortium (CPIC) publishes continuously updated guidelines for pharmacogenomic-guided prescribing. CPIC grades evidence and translates genotype into actionable prescribing recommendations. Key clinically implemented tests in India include:
| Gene | Drug Affected | Clinical Consequence | Recommended Action |
|---|---|---|---|
| G6PD | Primaquine, dapsone, nitrofurantoin, rasburicase | Haemolytic anaemia (oxidant stress) in G6PD-deficient individuals | Screen before primaquine; avoid oxidant drugs in G6PD deficiency |
| TPMT | Azathioprine, 6-mercaptopurine, thioguanine | Severe myelosuppression (poor metabolisers) | Test before initiation; dose-reduce 10-15 fold for homozygous deficiency |
| HLA-B*5701 | Abacavir (HIV antiretroviral) | Abacavir hypersensitivity reaction (life-threatening) | Screen before abacavir; do not use abacavir in carriers |
| CYP2D6 | Codeine, tramadol, tamoxifen, many antidepressants | Poor metabolisers: codeine toxicity risk; ultra-rapid: opioid overdose | Avoid codeine in known ultrarapid metabolisers (especially in breastfeeding); use alternative opioids |
| CYP2C19 | Clopidogrel, omeprazole, diazepam | PM: reduced antiplatelet effect with clopidogrel | Consider ticagrelor/prasugrel for PM patients post-ACS/stenting |
Practical prescribing adjustments:
- For a patient with documented G6PD deficiency requiring radical cure of Plasmodium vivax malaria, the standard primaquine course should be replaced with a modified low-dose regimen (0.75 mg/kg weekly for 8 weeks) or an alternative where available and locally approved — avoidance of primaquine altogether risks relapse in vivax malaria.
- For a TPMT-deficient patient requiring azathioprine for myasthenia gravis, the dose must be reduced by approximately 10–15 fold compared to standard dosing, with close haematological monitoring.
- Always document the pharmacogenomic result in the patient's medical record and medication summary so future prescribers can access this information.