Page 13 of 30
PH10.9-10 | PH10.{9-10} | Patient-Specific Dose Calculation and Therapeutic Drug Monitoring — SDL Guide — SDL Guide
Learning Objectives
- Calculate the appropriate dose of a drug for individual patients including children, elderly, pregnant/lactating women, and patients with renal or hepatic dysfunction
- Identify when therapeutic drug monitoring (TDM) is indicated for a given patient and drug, determine the correct timing for sampling, and calculate a revised dose from the result
INSTRUCTIONS
The standard adult dose on a drug package insert assumes a healthy 70-kg adult with normal renal and hepatic function, approximately 25–40 years of age. Most patients you will prescribe for are not this person. An 8-year-old child, a 75-year-old with CKD stage 4, a woman at 28 weeks of gestation, and a patient with Child-Pugh class B cirrhosis all require systematic dose adjustment based on quantifiable physiological parameters. Errors in dose calculation are a leading cause of preventable drug toxicity — and for narrow-therapeutic-index drugs, the margin between efficacy and harm is thin. This module builds the numerical and clinical reasoning skills to dose drugs correctly for the actual patient in front of you.
References
- KD Tripathi, Essentials of Medical Pharmacology, 8th ed, Ch 3 (Dose modification in special populations) (textbook)
- BNF (British National Formulary) — renal and hepatic impairment dose tables (reference)
- Cockcroft DW, Gault MH. Nephron 1976;16:31–41 — original derivation of the CrCl estimation equation (reference)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 78-year-old woman with diabetes, hypertension, and an eGFR of 28 mL/min/1.73m² is admitted with a gram-negative bacteraemia. The infectious disease team recommends gentamicin. The standard dose is 3–5 mg/kg/day. Her weight is 48 kg, serum creatinine is 2.8 mg/dL. You write the standard dose without adjustment. The next morning, her creatinine has risen to 4.1 mg/dL and she reports tinnitus. The consultant asks you why you gave the standard dose to a patient with already-compromised renal function.
WHY THIS MATTERS
Prescribing errors related to dosing account for approximately 20–30% of all adverse drug events in hospitalised patients, and a disproportionate burden falls on patients at the extremes of age or with renal or hepatic impairment. Children are particularly vulnerable because many drugs are not systematically studied in paediatric populations, and dose extrapolation from adults without weight-based adjustment has caused tragedies. Equally, the elderly — who have physiologically reduced renal clearance, reduced hepatic mass, altered body composition, and polypharmacy — are at double risk of toxicity from standard adult doses. Therapeutic drug monitoring (TDM) for narrow-therapeutic-index drugs provides a quantitative safety net that reduces both under- and over-dosing when pharmacokinetics are unpredictable.
RECALL
Recall from your pharmacokinetics studies that drug clearance is the primary determinant of steady-state plasma concentration at a given dose — and that renal clearance depends on glomerular filtration rate (GFR). You will have encountered the concept of creatinine clearance (CrCl) as a surrogate for GFR, and the principle that drugs excreted by the kidney accumulate when GFR is reduced, requiring either dose reduction or interval extension. Recall also that hepatic clearance depends on intrinsic enzymatic activity and liver blood flow — and that cirrhosis reduces both, particularly affecting drugs with high first-pass extraction (oral bioavailability increases for high-extraction drugs).
When Standard Doses Are Not Safe: The Need for Patient-Specific Dosing
The pharmacokinetic diversity of human patients means that a single dose cannot be universally appropriate. Drug concentrations at the site of action — the determinant of effect — are shaped by absorption, distribution, metabolism, and excretion parameters that vary substantially with patient age, body composition, organ function, and genetics.
Four clinical scenarios most commonly require systematic dose adjustment:
Renal impairment: Drugs and their active metabolites excreted by the kidney accumulate when GFR is reduced. The relationship is not simply linear — below certain GFR thresholds, drug concentrations rise exponentially. Gentamicin, vancomycin, digoxin, enoxaparin, metformin, and lithium are among the most important renally cleared drugs requiring adjustment. Failure to adjust doses in renal impairment is one of the most common prescribing errors in hospital practice.
Hepatic impairment: The liver is the primary site of drug metabolism for most drugs. Cirrhosis reduces hepatic enzyme activity, hepatic blood flow, and albumin synthesis (affecting protein binding and free drug fraction). Drugs with high first-pass hepatic extraction (e.g. propranolol, lignocaine, morphine) have dramatically increased bioavailability in cirrhosis. Coagulopathy in liver disease also interacts with anticoagulant prescribing.
Age extremes: Neonates and infants have immature metabolic enzymes (particularly CYP3A4 and glucuronidation), different body composition (higher body water fraction, lower fat content), and altered glomerular filtration. The elderly have physiologically reduced GFR even with normal serum creatinine (because reduced muscle mass lowers creatinine production), reduced hepatic mass and blood flow, and altered body composition (increased fat relative to lean mass, reducing Vd for water-soluble drugs).
Pregnancy and lactation: Pregnancy alters virtually every pharmacokinetic parameter — increased plasma volume, increased renal blood flow and GFR (increasing clearance of renally excreted drugs), altered protein binding, and changes in hepatic CYP activity. For lactating women, the key concern is drug transfer into breast milk and infant exposure — lipid-soluble, low-molecular-weight, low-protein-bound drugs transfer most readily.
Dose Adjustment Framework: Renal, Hepatic, Age, and Weight
A systematic framework for dose adjustment prevents both the under-dosing that leads to treatment failure and the over-dosing that causes toxicity. The framework for each clinical scenario is anchored to a quantifiable parameter.
Renal adjustment — Cockcroft-Gault equation:
The most widely used equation for estimating creatinine clearance in clinical dose adjustment is the Cockcroft-Gault formula:
CrCl (mL/min) = [(140 − Age) × Weight (kg)] ÷ [72 × Serum Creatinine (mg/dL)] × 0.85 (for females)
This equation was derived from adult patients and validated for clinical dose adjustment. Important caveats: it uses actual body weight (use ideal body weight for obese patients unless otherwise specified); it is not validated in extreme muscle wasting (creatinine production is very low, over-estimating CrCl) or extreme obesity (over-estimates CrCl). For drugs where the eGFR (MDRD or CKD-EPI) is specified in the product information, use that instead.
Once CrCl is calculated, most drug references provide dose adjustment tables indexed to CrCl ranges. The BNF renal impairment appendix and CIMS India provide drug-specific guidance.
Hepatic adjustment — Child-Pugh score:
The Child-Pugh score assesses hepatic functional reserve in cirrhotic patients, scoring five parameters (total bilirubin, albumin, prothrombin time, ascites, encephalopathy) from 1–3 each, giving a total of 5–15:
- Class A (5–6 points): well-compensated cirrhosis — standard doses often acceptable with monitoring
- Class B (7–9 points): significant functional impairment — dose reduction typically required for hepatically metabolised drugs
- Class C (10–15 points): decompensated cirrhosis — many drugs contraindicated or requiring major reduction
For drugs with high hepatic first-pass extraction (morphine, propranolol, lignocaine), oral bioavailability increases dramatically in cirrhosis — the same oral dose may produce several-fold higher plasma levels.
Paediatric dosing:
The gold standard for paediatric dosing is mg/kg body weight or, for chemotherapy and some other drugs, mg/m² body surface area (BSA). BSA is estimated by the Mosteller formula: BSA (m²) = √[(height(cm) × weight(kg)) ÷ 3600]. Drug paediatric doses are published in specialised references (BNF for Children, BNFC; WHO paediatric formulary).
Elderly dosing principles:
In the elderly, the physiological reduction in GFR means Cockcroft-Gault calculation is essential even with a 'normal' serum creatinine. Reduced hepatic mass reduces clearance of hepatically metabolised drugs. The principle of 'start low, go slow' applies — initiate at the lower end of the dose range and titrate based on response and tolerance.
Pregnancy and lactation: Use pregnancy category ratings (FDA, WHO, Indian category) and lactation risk categories (Hale's Lactation Risk Categories, LactMed database) to assess benefit-risk. Avoid drugs in pregnancy category X (teratogenic with no acceptable benefit). For lactating women, drugs with low milk-to-plasma ratio, high oral bioavailability concerns in the infant, or high pharmacological potency require either avoidance or suspension of breastfeeding during treatment.
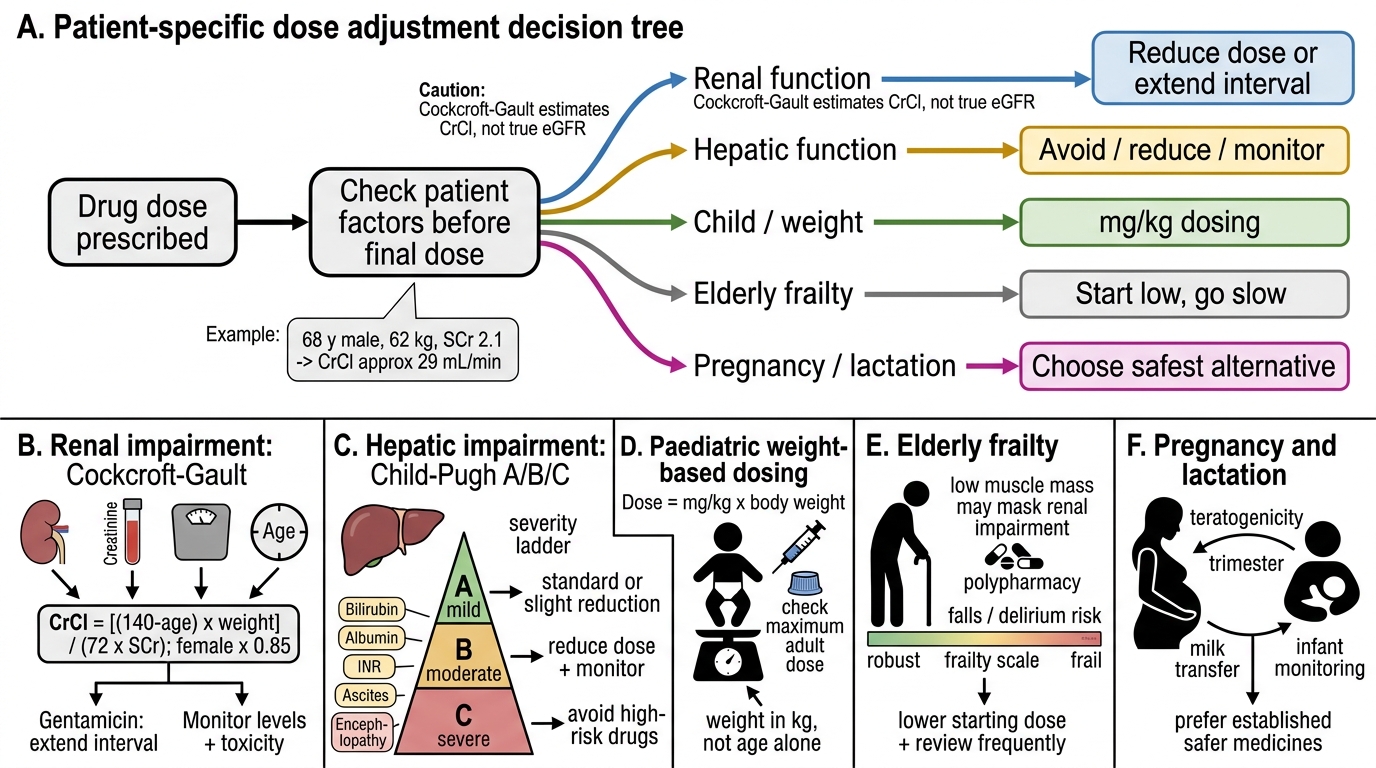
Patient-Specific Dose Adjustment Decision Tree
SELF-CHECK
A 68-year-old male patient (weight 62 kg, serum creatinine 2.1 mg/dL) requires gentamicin. Using the Cockcroft-Gault formula, what is his estimated creatinine clearance (CrCl)?
A. A) Approximately 29 mL/min
B. B) Approximately 45 mL/min
C. C) Approximately 54 mL/min
D. D) Approximately 22 mL/min
Reveal Answer
Answer: A. A) Approximately 29 mL/min
A is correct. CrCl = (140−68) × 62 ÷ (72 × 2.1) = 72 × 62 ÷ 151.2 = 4464 ÷ 151.2 ≈ 29.5 mL/min. This is Stage 3b-4 CKD range and requires significant gentamicin dose reduction or extended interval dosing — the standard dose without adjustment in this patient would risk nephrotoxicity and ototoxicity. No female correction factor (×0.85) applies as this patient is male.
Dose Calculation in Practice: Worked Examples
Applying the dose adjustment framework to worked clinical problems converts principle into clinical skill. Three examples cover the most important patient populations encountered in practice.
Example 1 — Gentamicin in an elderly patient with CKD (renal dose adjustment):
Patient: 70-year-old female, weight 52 kg, serum creatinine 2.4 mg/dL. Indication: gram-negative bacteraemia requiring aminoglycoside.
Step 1 — Calculate CrCl (Cockcroft-Gault): CrCl = [(140−70) × 52] ÷ (72 × 2.4) × 0.85 = [70 × 52] ÷ 172.8 × 0.85 = 3640 ÷ 172.8 × 0.85 = 21.1 × 0.85 = 17.9 mL/min.
Step 2 — Apply dose adjustment: standard gentamicin 5 mg/kg/day. For CrCl 10–30 mL/min, the standard approach is extended interval dosing (once daily, but with a reduced or standard dose; or reduce to every 36–48 hours based on levels). For CrCl ~18 mL/min: give initial loading dose 5 mg/kg IV; extend interval to 48 hours; monitor trough levels (target <2 mg/L) and peak levels (5–10 mg/L).
Step 3 — Clinical note: document the calculation and monitoring plan. Flag for pharmacy review. Ensure TDM levels are drawn correctly.
Example 2 — Paediatric amoxicillin dosing:
Child: 4 years old, weight 16 kg. Indication: community-acquired pneumonia (moderate, requiring amoxicillin).
Standard paediatric dose for pneumonia: 40–90 mg/kg/day in 3 divided doses (high dose for pneumococcal coverage). Use 45 mg/kg/day for this case.
Dose per day = 45 × 16 = 720 mg/day. Divided in 3 doses = 240 mg per dose, TID. Formulation: amoxicillin 250 mg/5 mL suspension → each dose = (240/250) × 5 mL = 4.8 mL ≈ 5 mL TID. Duration: 5–7 days. Write complete prescription with all elements.
Example 3 — Hepatic adjustment for morphine in cirrhosis:
Patient: 55-year-old male with alcoholic cirrhosis (Child-Pugh Class B, score 8), requiring opioid analgesia for a painful pathological rib fracture.
Morphine is a high-hepatic-extraction drug — first-pass metabolism is substantially reduced in cirrhosis → oral bioavailability increased; glucuronidation (the major metabolic pathway) is also reduced → morphine accumulates; active metabolite morphine-6-glucuronide also accumulates and has respiratory depressant activity.
Adjustment: reduce dose by approximately 50% and extend interval; use with extreme caution; start at 2.5–5 mg oral 6-hourly rather than standard 10 mg 4-hourly; monitor closely for sedation and respiratory depression. Avoid if hepatic encephalopathy is present.