Page 14 of 30
PH10.9-10 | PH10.{9-10} | Patient-Specific Dose Calculation and Therapeutic Drug Monitoring — SDL Guide — SDL Guide (Part 2)
Therapeutic Drug Monitoring: Principles and Indications
Therapeutic drug monitoring (TDM) is the measurement of drug concentration in a biological fluid (usually plasma or serum) to guide dosing decisions. It is clinically applicable when: (1) the drug has a narrow therapeutic index (the difference between the minimally effective concentration and the toxic concentration is small); (2) there is a predictable relationship between plasma concentration and clinical effect/toxicity; (3) significant inter-individual pharmacokinetic variability exists; and (4) the clinical response cannot be easily and quickly measured otherwise.
TDM adds nothing when the drug has a wide therapeutic index (most penicillins), when dose-response is poorly correlated with plasma levels, or when a direct clinical endpoint is easily measurable.
Drugs commonly requiring TDM:
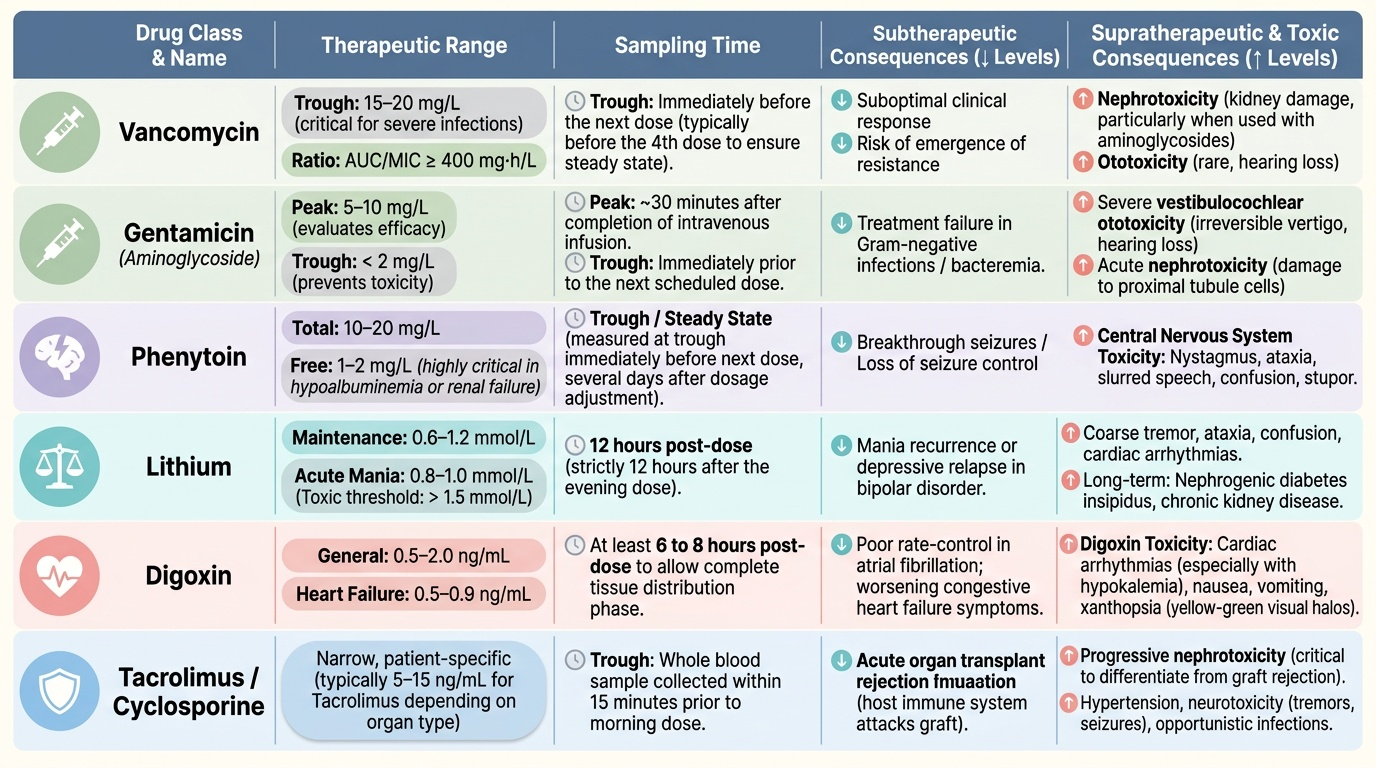
- Antibiotics: Vancomycin (trough 15–20 mg/L for serious infections; or AUC/MIC >400 mg·h/L — the modern PK/PD target); aminoglycosides (gentamicin trough <2 mg/L, peak 5–10 mg/L for gram-negative infections)
- Anticonvulsants: Phenytoin (10–20 mg/L total; free level 1–2 mg/L; especially important in hypoalbuminaemia or renal failure where protein binding is altered); carbamazepine (4–12 mg/L); valproate (50–100 mg/L)
- Mood stabilisers: Lithium (0.6–1.2 mmol/L maintenance; 0.8–1.0 mmol/L for acute mania; toxic >1.5 mmol/L — narrow index with serious toxicity including renal diabetes insipidus, tremor, neurotoxicity, cardiac arrhythmia)
- Cardiac: Digoxin (0.5–2 ng/mL; heart failure target 0.5–0.9 ng/mL; >2 ng/mL likely toxic); theophylline (10–20 mg/L)
- Immunosuppressants: Cyclosporine, tacrolimus, sirolimus — all narrow therapeutic index transplant drugs with complex CYP3A4 interactions requiring TDM
- Anticoagulants: Warfarin is monitored by the INR (a surrogate TDM endpoint) rather than drug level
Provided image
SELF-CHECK
A patient on phenytoin 300 mg/day for epilepsy is found to have a serum albumin of 2.1 g/dL (normal: 3.5–5 g/dL) following hospitalisation for hepatitis. Her measured total phenytoin level is 9 mg/L. What is the most appropriate interpretation?
A. A) The level is subtherapeutic (normal range 10–20 mg/L) — increase the dose
B. B) Hypoalbuminaemia reduces phenytoin protein binding, increasing free (active) drug fraction — the apparent total level may under-represent therapeutic free drug; measure free phenytoin level or apply Sheiner-Tozer correction before adjusting dose
C. C) The level is subtherapeutic regardless of albumin — always treat the total level
D. D) Reduce the dose because hepatitis increases free phenytoin levels to toxic concentrations
Reveal Answer
Answer: B. B) Hypoalbuminaemia reduces phenytoin protein binding, increasing free (active) drug fraction — the apparent total level may under-represent therapeutic free drug; measure free phenytoin level or apply Sheiner-Tozer correction before adjusting dose
B is correct. Phenytoin is highly protein-bound (approximately 90%) to albumin. In hypoalbuminaemia, a greater fraction of phenytoin exists as free (unbound, active) drug. The Sheiner-Tozer correction adjusts the measured total level: Corrected phenytoin = Measured level ÷ [(0.2 × Albumin g/dL) + 0.1]. For albumin 2.1 g/dL: corrected level = 9 ÷ [(0.2 × 2.1) + 0.1] = 9 ÷ 0.52 = 17.3 mg/L — well within the therapeutic range. Increasing the dose based on the uncorrected total level could cause toxicity. Measuring the free phenytoin level directly (target 1–2 mg/L) is the most accurate approach.
TDM in Practice: Sample Timing, Interpretation, and Dose Revision
The clinical value of TDM depends entirely on correct sample timing. A level drawn at the wrong time in the dosing cycle produces an uninterpretable result that may mislead rather than guide dosing. Understanding when to draw the sample — and what question you are trying to answer — is as important as knowing the therapeutic range.
Timing principles:
- Trough level (pre-dose, just before next dose): The lowest concentration in the dosing cycle. Used for most TDM assessments. Must wait for steady state (≥5 × half-life from initiation or dose change). Draw within 30 minutes before the scheduled next dose.
- Peak level (post-dose): The highest concentration — assessed for efficacy (aminoglycosides) and toxicity. Timing depends on route: IV drugs peak 30–60 minutes post-infusion; IM drugs peak later. For aminoglycosides, peak is drawn 30 minutes after the end of a 30-minute infusion.
- Random levels: For drugs with long half-lives and stable concentrations at steady state (e.g. digoxin, lithium — sample at trough for digoxin, 12 hours post-dose for lithium maintenance; both require steady state).
Interpreting the level:
1. Is the patient at steady state? (≥5 × t½ after last dose change)
2. Was the sample timed correctly?
3. Is the level within the therapeutic range for this patient's indication and clinical context?
4. Does the patient have clinical signs of toxicity or treatment failure?
Dose revision:
For drugs following first-order kinetics with linear pharmacokinetics (most drugs), plasma concentration is proportional to dose. The revised dose is calculated:
New dose = Current dose × (Target level ÷ Measured level)
Example: a patient on vancomycin 1000 mg every 12 hours has a trough of 8 mg/L. Target trough for serious infection: 15 mg/L.
New dose = 1000 × (15 ÷ 8) = 1875 mg — round to 1750 mg or 2000 mg every 12 hours (depending on renal function and available formulation), with repeat TDM after 3–4 doses.
Worked TDM case — lithium toxicity:
A 45-year-old bipolar patient on lithium 800 mg twice daily is admitted with tremor, confusion, and polyuria. Lithium level: 2.1 mmol/L (target maintenance: 0.6–1.2 mmol/L; toxic >1.5 mmol/L). Interpretation: supratherapeutic → lithium toxicity. Management: hold lithium, check renal function (lithium clearance = renal clearance), ensure adequate hydration (sodium depletion increases lithium retention), ECG (lithium prolongs QT), and consider renal replacement therapy for severe toxicity (lithium is dialysable). Restart at lower dose after recovery with renal monitoring.
CLINICAL PEARL
Always wait for steady state before drawing a TDM level — except for suspected acute toxicity, where an immediate random level is informative. The most common TDM error is drawing a level after only 1–2 doses (before steady state), then misinterpreting a low level as requiring dose escalation when the drug simply has not equilibrated yet. For phenytoin (t½ 22–24 h), steady state is approximately 5 days. For lithium (t½ 18–24 h), steady state is approximately 5 days. For digoxin (t½ 36–48 h), steady state is approximately 7–8 days. Document the date and time of the last dose and the sample collection time on the TDM request — without this, the result cannot be correctly interpreted.
Critical Appraisal of Dose Decisions: Evaluating Adequacy and Safety
Beyond the mechanics of calculation, the clinician must also critically appraise dose decisions — asking whether the chosen dose is likely to be sufficient for efficacy and safe from toxicity for this specific patient at this point in time. This integrative skill links dose calculation with clinical monitoring and patient communication.
Signs suggesting under-dosing:
- Clinical treatment failure (infection not responding, seizures breakthrough, arrhythmia uncontrolled)
- TDM level below the therapeutic range at steady state with correct sampling
- Short half-life drug with rapid clearance in a patient known to be a rapid metaboliser (pharmacogenomic)
Signs suggesting over-dosing or toxicity:
- Clinical signs of drug toxicity (aminoglycoside: tinnitus, rising creatinine; phenytoin: nystagmus, ataxia, diplopia at >20 mg/L; lithium: coarse tremor, confusion, polyuria at >1.5 mmol/L; vancomycin: nephrotoxicity with trough consistently >20 mg/L)
- TDM level above the therapeutic range at correct sampling
- Declining renal function in a patient on a renally cleared drug (accumulation loop)
Interaction with pharmacy:
Clinical pharmacists are expert partners in TDM and dose adjustment. Best practice involves proactive pharmacy review of all doses for patients with renal/hepatic impairment, extremes of age, or narrow-therapeutic-index drugs. Many hospitals have formal pharmacy-run TDM services for vancomycin, aminoglycosides, and transplant immunosuppressants.
The accumulation loop trap:
Renal impairment causes drug accumulation → drug accumulation causes further nephrotoxicity (for nephrotoxic drugs like aminoglycosides, vancomycin, NSAIDs) → worsening renal impairment causes more drug accumulation. This positive feedback loop must be anticipated and interrupted with dose adjustment and renal function monitoring from the first dose.
Self-Assessment: Dose Calculation and TDM
Work through the following numerical exercises to consolidate your dose calculation and TDM skills.
Exercise 1 — Renal dose calculation:
A 65-year-old male, weight 70 kg, serum creatinine 3.2 mg/dL, requires gentamicin for a gram-negative urinary sepsis. Standard dose: 5 mg/kg/day.
(a) Calculate his CrCl using the Cockcroft-Gault formula.
(b) Given that the standard interval is 24-hourly, what dose adjustment would you make?
Expected answers:
(a) CrCl = (140−65) × 70 ÷ (72 × 3.2) = 75 × 70 ÷ 230.4 = 5250 ÷ 230.4 = 22.8 mL/min. (No ×0.85 as male.)
(b) CrCl ~23 mL/min = significant renal impairment. Options: (i) Reduce dose: 5 × 70 = 350 mg standard dose → reduce by approximately 50–60% for CrCl 20–30 mL/min → give approximately 130–140 mg once daily, with TDM to guide; or (ii) Maintain dose but extend interval (every 36–48 hours — calculate extended interval as standard interval × standard CrCl ÷ actual CrCl = 24 × 120 ÷ 23 ≈ 125 hours, which is excessive — therefore dose reduction is preferred for this severity of CKD). Practical approach: give a loading dose (5 mg/kg = 350 mg), then monitor TDM levels to determine the next dose and timing. Consult pharmacy.
Exercise 2 — TDM interpretation:
A patient on carbamazepine for epilepsy has a breakthrough seizure. Her carbamazepine level is drawn 2 hours after the morning dose and reported as 2.8 mg/L (therapeutic range 4–12 mg/L).
(a) Is this level interpretable? (b) What is the likely issue with the sample timing? (c) What would you recommend?
Expected answers:
(a) The level is NOT reliably interpretable as an assessment of steady-state trough. (b) The sample was drawn as a peak-ish level (2 hours post-dose), not a trough — carbamazepine Tmax is approximately 4–8 hours for conventional tablets. A 2-hour post-dose level does not reflect trough or steady-state. (c) Redraw the level at trough (just before the next scheduled dose), document the time of last dose and sample time on the request form, and ensure the patient is at steady state. If the trough level is then confirmed low (<4 mg/L), a dose increase is appropriate.