Page 1 of 15
PH2.6 | PH2.6 | Antihistamines for Allergic Rhinitis — SDL Guide — SDL Guide
Learning Objectives
- Classify H1 antihistamines into first-generation (sedating) and second-generation (non-sedating) with named examples from each class.
- Explain the H1-receptor-mediated mechanism of action and the pharmacological basis for generation differences (BBB penetration, receptor selectivity, anticholinergic effects).
- Describe salient pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of key antihistamines.
- Outline the management of allergic rhinitis and common cold with appropriate drug selection based on patient profile and severity.
INSTRUCTIONS
Antihistamines are among the most widely prescribed drugs in clinical practice, and a working knowledge of their differences separates a safe prescriber from a dangerous one. Every doctor will encounter patients with allergic rhinitis, urticaria, and the common cold. Choosing the right antihistamine — first or second generation, oral or topical — requires understanding the pharmacology behind sedation, anticholinergic burden, and the H1 vs H2 receptor distinction. This module builds that clinical reasoning from the pathophysiology up.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed. Jaypee; 2019. Ch 21 (Autacoids & their antagonists) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. McGraw-Hill; 2018. Ch 32 (Histamine, bradykinin, and their antagonists) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old college student comes to the outpatient clinic in April complaining of sneezing, watery nasal discharge, nasal itching, and red, itchy eyes that worsen every time she studies outdoors in the campus garden. She has been self-medicating with her father's leftover chlorpheniramine tablets but reports she keeps falling asleep during lectures after each dose. She asks whether there is 'a better medicine that won't knock me out.' What would you prescribe, and why does her father's drug cause so much sedation?
WHY THIS MATTERS
Allergic rhinitis affects roughly 10–30% of the global population and is one of the top five reasons for outpatient visits in India. As a clinician, you will prescribe antihistamines multiple times every week — for rhinitis, urticaria, insect bites, drug reactions, and the common cold. Understanding the generation-based pharmacological differences allows you to tailor therapy: a truck driver and a student sitting an exam need the same anti-allergic effect but very different sedation profiles. The skills in this module map directly to NMC competency PH2.6 and will be tested through prescribing OSCEs.
RECALL
Before beginning, recall three foundations from your earlier courses:
- Mast cells are tissue-resident immune cells that store histamine, heparin, and proteases in granules. On re-exposure to an allergen, cross-linking of surface-bound IgE triggers rapid degranulation — releasing histamine into surrounding tissue.
- H1 and H2 histamine receptors are G-protein-coupled receptors with distinct locations and functions. H1 receptors are found on smooth muscle, vascular endothelium, and bronchial epithelium; H2 receptors are predominantly on gastric parietal cells.
- Anticholinergic blockade of muscarinic receptors produces the classic cluster: dry mouth, blurred vision, urinary retention, constipation, and tachycardia. Several 1st-generation antihistamines possess this additional action, which determines their ADR profile.
Pathophysiology of Allergic Rhinitis and the Role of Histamine
Allergic rhinitis is a type I IgE-mediated hypersensitivity reaction affecting the nasal mucosa. The sequence begins with sensitisation: on first exposure to an allergen (pollen, dust mite, animal dander), dendritic cells present antigenic peptides to Th2 lymphocytes, which orchestrate B-cell class switching to produce allergen-specific IgE. This IgE binds to high-affinity FcεRI receptors on the surface of mast cells and basophils, effectively arming them for rapid response.
On re-exposure, the allergen cross-links adjacent IgE molecules on the mast cell surface, triggering a cascade of intracellular signals that result in exocytosis of preformed granule contents — predominantly histamine and tryptase — within seconds. Histamine then acts on H1 receptors in the nasal mucosa, conjunctiva, and skin to produce the immediate symptoms: sneezing (reflex via the trigeminal nerve), rhinorrhoea (vasodilation and increased vascular permeability), nasal itching (sensory nerve stimulation), and nasal congestion (venous sinusoidal engorgement). The late-phase reaction, occurring 4–8 hours later, is driven by newly synthesised eicosanoids and cytokines that contribute to chronic inflammation and mucosal hyper-reactivity.
Critically, H1 receptors mediate the allergy symptoms, while H2 receptors on gastric parietal cells regulate acid secretion — targeting H2 receptors (as with ranitidine) does nothing for rhinitis. This receptor distinction justifies why only H1 antagonists are used in managing allergic rhinitis.
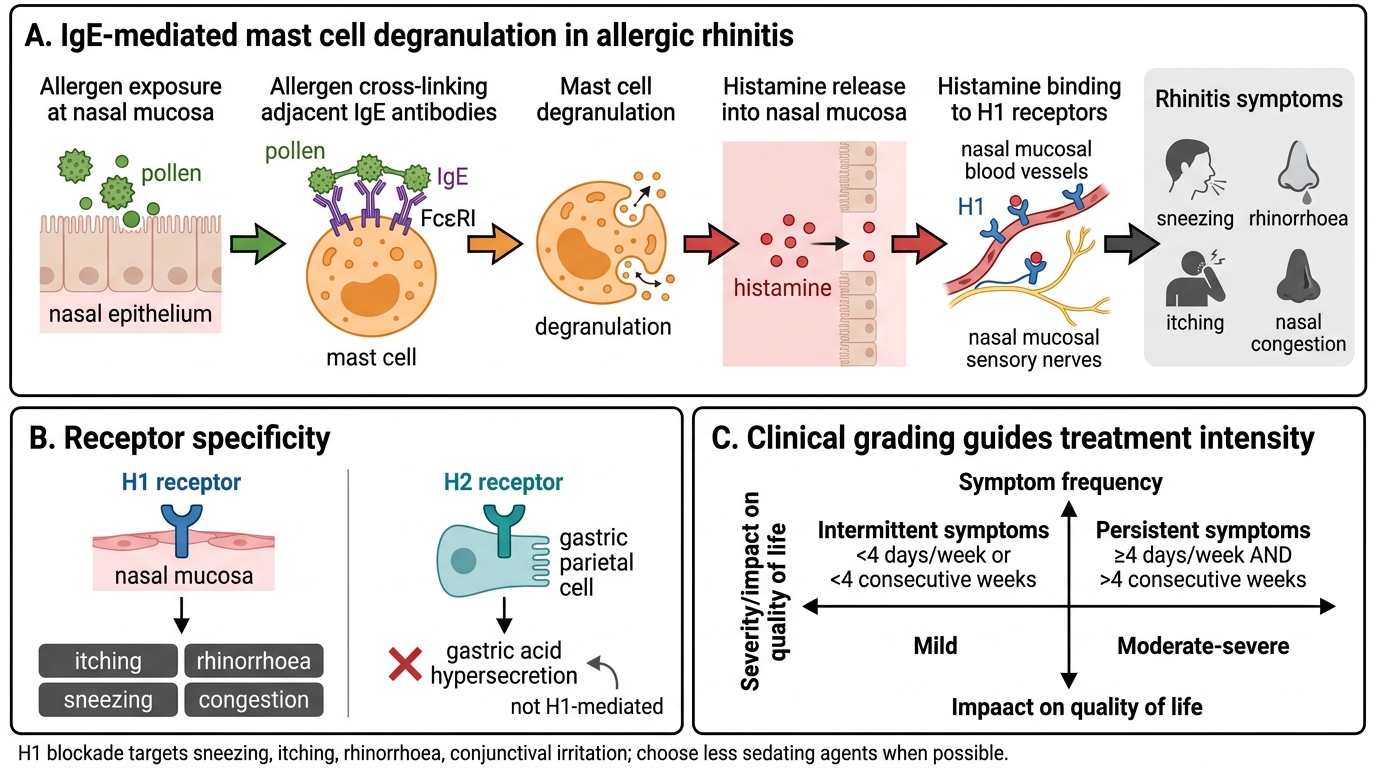
IgE-Mediated Mast Cell Degranulation in Allergic Rhinitis
The clinical presentation of allergic rhinitis divides into intermittent (symptoms <4 days/week or <4 consecutive weeks) and persistent (symptoms ≥4 days/week AND >4 consecutive weeks), with further grading into mild or moderate–severe based on impact on quality of life (ARIA classification). This staging guides treatment intensity.
SELF-CHECK
A patient with seasonal rhinitis is started on a drug. The prescriber explains that this drug blocks H1 receptors on nasal mucosa smooth muscle. Which symptom is NOT primarily mediated by H1 receptor stimulation?
A. Nasal itching
B. Sneezing
C. Gastric acid hypersecretion
D. Increased vascular permeability causing rhinorrhoea
Reveal Answer
Answer: C. Gastric acid hypersecretion
Gastric acid secretion is mediated by H2 receptors on parietal cells, not H1 receptors. H1 receptors mediate smooth muscle contraction, increased vascular permeability (rhinorrhoea), itching, and sneezing. This is why H2 blockers like ranitidine are used for peptic ulcers, not for allergic rhinitis.
Therapeutic Goals and Rationale for H1 Blockade
The primary therapeutic goal in allergic rhinitis is to relieve the H1-receptor-mediated symptoms — sneezing, itching, rhinorrhoea, and conjunctival irritation — while minimising the sedation and anticholinergic burden that impair the patient's daily functioning. Modern therapy also aims to prevent the late-phase inflammatory response wherever possible.
Histamine H1 antagonists work by competitive, reversible blockade of H1 receptors. Because they are inverse agonists rather than simple competitive blockers, they do not merely prevent histamine from binding — they also suppress the constitutive activity of H1 receptors, reducing baseline allergic tone. This mechanistic nuance explains why antihistamines taken prophylactically (before allergen exposure) are more effective than those taken after symptoms are already established.
The rationale for choosing H1 blockade as the cornerstone of rhinitis therapy rests on three pillars:
1. Precision: H1 receptors are the primary mediators of itching, sneezing, rhinorrhoea, and urticaria — directly countering the mast cell's key mediator.
2. Speed: Oral antihistamines work within 30–60 minutes, providing rapid symptomatic relief.
3. Safety window: When the correct generation is chosen for the clinical context, the benefit-risk profile is excellent.
It is equally important to understand what antihistamines do NOT do: they do not prevent allergen sensitisation, reverse mucosal oedema due to chronic inflammation, or treat the bacterial component of sinusitis. For nasal congestion and late-phase inflammation, intranasal corticosteroids (e.g., fluticasone, mometasone) are more effective and are recommended as first-line for moderate–severe persistent allergic rhinitis.
Classification of H1 Antihistamines
All clinically used H1 antihistamines can be divided into two generations based on their pharmacological profile, particularly their ability to penetrate the blood-brain barrier (BBB) and their receptor selectivity. Understanding the basis of this generation distinction is essential for rational prescribing.
First-generation H1 antihistamines are lipophilic, low-molecular-weight compounds that readily cross the BBB, occupying central H1 receptors and producing sedation, cognitive impairment, and psychomotor slowing. They also bind muscarinic, adrenergic, serotonin, and dopamine receptors to varying degrees, explaining their broad anticholinergic and other side effects. Key drugs: chlorpheniramine (the Indian workhorse; available in most OTC cold combinations), diphenhydramine (prototype; strong anticholinergic and sedative; also used as a hypnotic), promethazine (phenothiazine derivative; strong D2 and H1 blockade; antiemetic, motion sickness), hydroxyzine (useful in anxiety + pruritus), cyproheptadine (H1 + antiserotonin; used as appetite stimulant in children).
Second-generation H1 antihistamines are designed to minimise CNS penetration through high molecular weight, active P-glycoprotein efflux at the BBB, and reduced lipophilicity. They are selective for peripheral H1 receptors, producing minimal sedation and no anticholinergic effects. Key drugs: cetirizine (active metabolite of hydroxyzine; modest CNS penetration — mild sedation possible at higher doses), loratadine (truly non-sedating at therapeutic doses; prodrug converted to desloratadine), fexofenadine (active metabolite of terfenadine; no CNS penetration; preferred when zero sedation is critical), levocetirizine (R-enantiomer of cetirizine; slightly more potent), desloratadine (active metabolite of loratadine; once-daily dosing), azelastine (topical intranasal antihistamine; rapid local action, minimal systemic absorption).
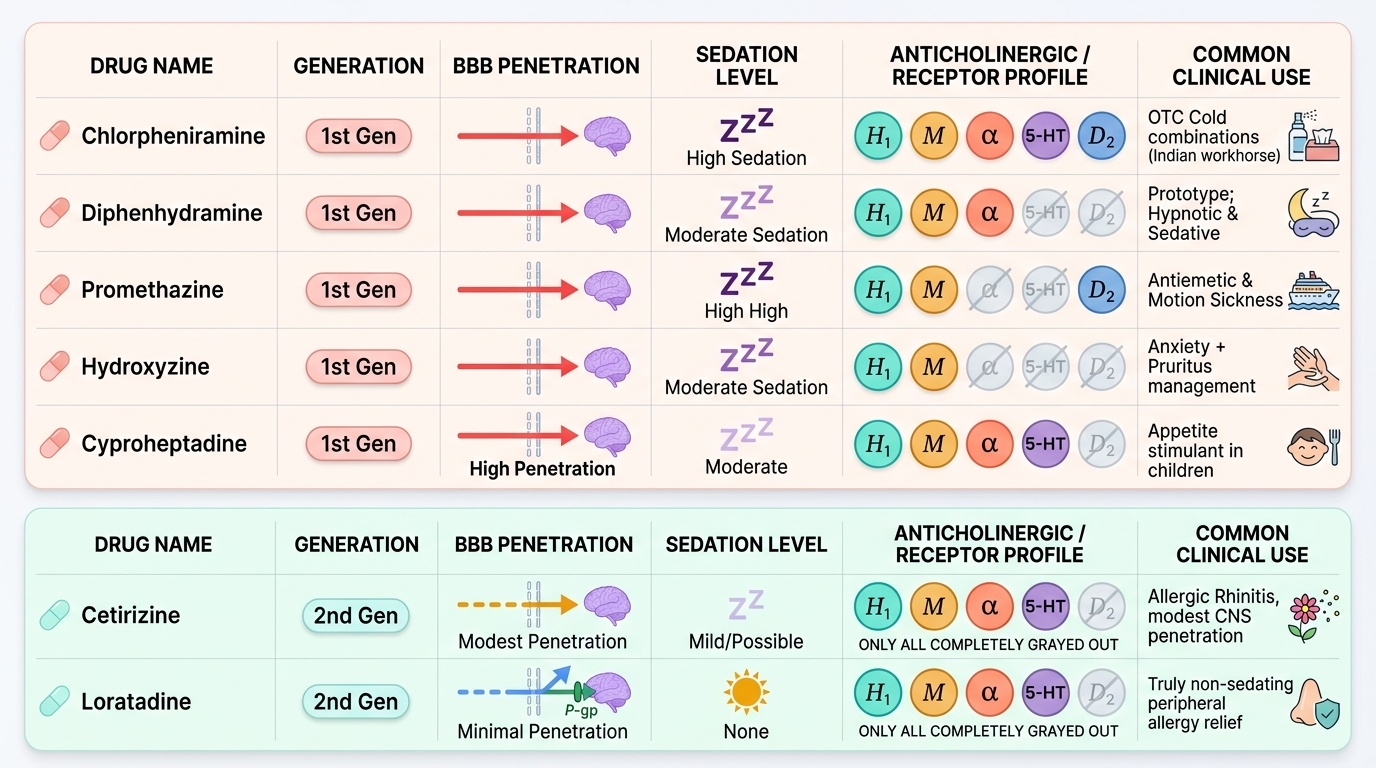
Provided image
A practical clinical rule: first-generation antihistamines should not be given to patients who must remain alert (drivers, machine operators, students sitting exams, the elderly who are at fall risk). Second-generation agents are the standard of care in outpatient allergic rhinitis management.