Page 2 of 15
PH2.6 | PH2.6 | Antihistamines for Allergic Rhinitis — SDL Guide — SDL Guide (Part 2)
Pharmacokinetics, Pharmacodynamics, and Adverse Effects of Antihistamines
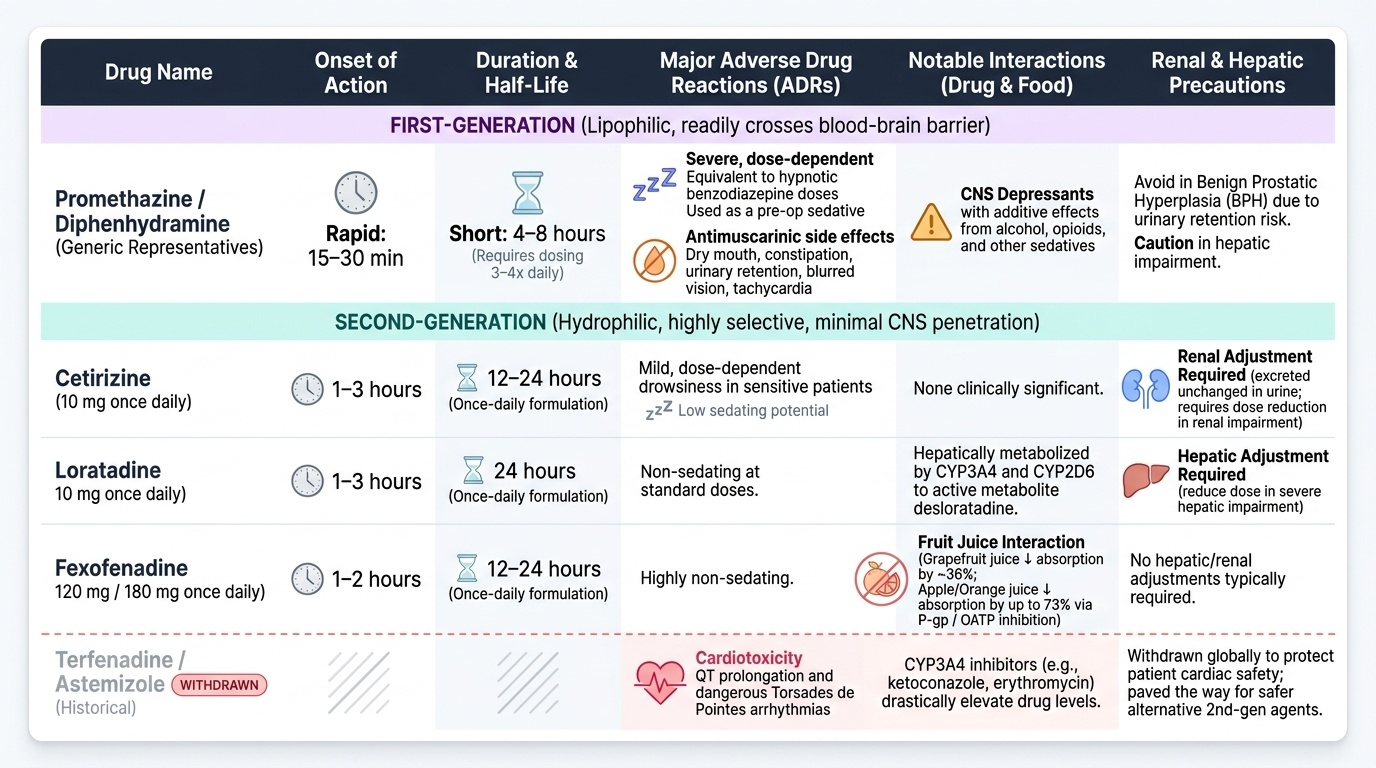
Understanding the pharmacokinetic profile of antihistamines explains why dosing schedules differ and why certain patient groups require dose adjustment. All oral H1 antihistamines are well absorbed from the gastrointestinal tract. First-generation agents have relatively short half-lives (4–8 hours for most), requiring dosing three to four times daily, while second-generation agents are formulated as once-daily drugs due to longer half-lives (12–24 hours) and active-metabolite accumulation.
First-generation antihistamines are extensively metabolised by hepatic CYP enzymes and excreted in urine. Their most clinically significant pharmacodynamic consequence beyond H1 blockade is antimuscarinic activity: dry mouth, constipation, urinary retention (caution in benign prostatic hyperplasia), blurred vision, and tachycardia. Sedation can reach a degree equivalent to a hypnotic dose of benzodiazepine — promethazine is used deliberately as a preoperative sedative and antiemetic. CNS depression is additive with alcohol, opioids, and other sedatives — a critical drug interaction. Tolerance to sedation develops over days, but tolerance to antihistaminic effect also develops, limiting long-term utility.
Second-generation antihistamines have wider therapeutic indices. Cetirizine (10 mg once daily) may cause mild sedation in some patients, especially at higher doses; dose reduction is required in renal impairment (excreted unchanged). Loratadine (10 mg once daily) is metabolised by CYP3A4 and CYP2D6 to desloratadine; dose adjustment in severe hepatic impairment. Fexofenadine (120 mg or 180 mg once daily) is a substrate of P-glycoprotein and organic anion transporters — co-administration of grapefruit juice, apple juice, or orange juice significantly reduces its bioavailability by up to 36–73% depending on the specific juice (grapefruit ~36%, apple or orange juice up to 73%) — a clinically relevant interaction to counsel patients about. Terfenadine and astemizole (historical 2nd-gen agents) were withdrawn because of QT prolongation and fatal arrhythmias (torsades de pointes) via CYP3A4-mediated drug interactions — this reinforces why newer agents were developed to avoid cardiac risk.
Provided image
The most common ADRs by generation:
- First-gen: sedation, dry mouth, urinary retention, blurred vision, constipation, tachycardia, weight gain (cyproheptadine via antiserotonin effect), extrapyramidal effects (promethazine, high doses)
- Second-gen: generally well tolerated; mild headache, dry mouth at higher doses; cetirizine — occasional drowsiness; fexofenadine — headache, nausea; rare cardiac risk with historical 2nd-gen only
SELF-CHECK
A 35-year-old truck driver presents with seasonal allergic rhinitis. Which antihistamine is MOST appropriate to prescribe for daytime symptom control?
A. Chlorpheniramine 4 mg three times daily
B. Promethazine 25 mg at night only
C. Fexofenadine 120 mg once daily
D. Diphenhydramine 25 mg as needed
Reveal Answer
Answer: C. Fexofenadine 120 mg once daily
Fexofenadine is a non-sedating second-generation antihistamine with negligible CNS penetration. It is the safest choice for patients who must remain alert, such as drivers. Chlorpheniramine, promethazine, and diphenhydramine are all first-generation agents with significant sedating effects that would impair driving and create serious safety risks.
Management of Allergic Rhinitis and Common Cold
The management of allergic rhinitis is stepwise, guided by symptom severity, frequency, and patient-specific factors. The ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines, widely adopted in India, provide a rational framework for prescribing decisions.
Mild intermittent allergic rhinitis: Oral second-generation antihistamines (cetirizine, loratadine, fexofenadine, levocetirizine) are the first-line treatment. They reliably control sneezing, itching, and rhinorrhoea. Topical azelastine nasal spray provides rapid local relief and is an alternative, especially for patients who prefer topical therapy.
Moderate–severe or persistent allergic rhinitis: Intranasal corticosteroids (e.g., fluticasone furoate, mometasone, budesonide) are the most effective single agents, addressing both early and late-phase inflammatory responses. They are recommended as first-line for moderate–severe persistent disease. Oral antihistamines may be added for breakthrough sneezing/itching. The combination of intranasal corticosteroid + antihistamine is superior to either alone for nasal congestion and discharge. Intranasal decongestants (oxymetazoline, xylometazoline) provide rapid decongestion but must not be used for more than 3–5 consecutive days to avoid rhinitis medicamentosa (rebound nasal congestion due to α-adrenergic receptor downregulation). Oral decongestants (pseudoephedrine) can be used short-term but are contraindicated in hypertension, hyperthyroidism, and ischaemic heart disease.
Management of the common cold: The common cold is caused by rhinoviruses and other respiratory viruses. Antihistamines are NOT proven to reduce the duration or severity of cold symptoms in otherwise healthy adults. First-generation antihistamines (chlorpheniramine) remain widely included in combination cold products in India — the rationale being their anticholinergic drying effect on rhinorrhoea — but evidence-based guidelines do not endorse them for cold management. Antibiotics are contraindicated in uncomplicated common cold. Management is supportive: adequate hydration, rest, saline nasal irrigation, and analgesics (paracetamol, ibuprofen) for fever and myalgia. Zinc acetate lozenges started within 24 hours of symptom onset may modestly reduce duration. Vitamin C supplementation in established colds has not shown clinically meaningful benefit.
Special populations:
- Children under 2 years: no antihistamines (first-gen are particularly hazardous; risk of paradoxical excitation and respiratory depression)
- Elderly: avoid first-generation antihistamines (fall risk from sedation + anticholinergic-induced confusion — anticholinergic burden worsens cognitive impairment in those at risk of dementia)
- Pregnancy: chlorpheniramine is traditionally preferred (longest safety record); second-gen agents (loratadine, cetirizine) are considered acceptable in the 2nd and 3rd trimester but avoid in the 1st trimester
- Glaucoma / BPH: avoid all anticholinergic antihistamines (first-generation); use only second-generation
CLINICAL PEARL
The 'Fexofenadine and Fruit Juice' Interaction: Patients on fexofenadine should be specifically counselled to take the drug with water, NOT with fruit juices. Grapefruit, apple, and orange juices inhibit intestinal OATP (organic anion transporting polypeptide) transporters, reducing fexofenadine bioavailability by up to 36–73%. This interaction is counter-intuitive to patients who assume 'natural juice' is harmless and may lead to apparent treatment failure. This is one of the rare instances where a food–drug interaction involves reduced (not increased) drug bioavailability — distinct from the grapefruit-CYP3A4 interaction that typically increases drug levels.
SELF-CHECK
A 60-year-old man with benign prostatic hyperplasia (BPH) and allergic rhinitis is prescribed an antihistamine. The next day he presents to the emergency department with acute urinary retention. Which drug was most likely prescribed?
A. Fexofenadine
B. Loratadine
C. Chlorpheniramine
D. Levocetirizine
Reveal Answer
Answer: C. Chlorpheniramine
Chlorpheniramine is a first-generation antihistamine with significant antimuscarinic (anticholinergic) activity. Muscarinic blockade of the detrusor muscle reduces bladder contractility, precipitating acute urinary retention in patients with pre-existing BPH who already have impaired bladder emptying. Second-generation agents (fexofenadine, loratadine, levocetirizine) lack anticholinergic effects and are safe in BPH patients.