Page 4 of 15
PH2.7 | PH2.7 | Non-Opioid Analgesics and NSAIDs — SDL Guide — SDL Guide
Learning Objectives
- Define pain and explain the role of prostaglandins in peripheral and central sensitisation.
- Classify non-opioid analgesics (non-selective NSAIDs, selective COX-2 inhibitors, paracetamol, and pyrazolones) with named examples.
- Describe the mechanism of action, salient pharmacokinetics, pharmacodynamics, therapeutic uses, and adverse drug reactions of analgesics including NSAIDs.
- Identify contraindications, drug interactions, and the clinical basis for rational NSAID selection in individual patients.
INSTRUCTIONS
Pain is the most common presenting complaint in clinical medicine. Non-opioid analgesics — from the ubiquitous paracetamol to the double-edged NSAIDs — are drugs you will prescribe every single day. Getting their pharmacology right means your patients get effective pain relief without preventable GI bleeds, acute kidney injury, or cardiovascular events. This module takes you from the arachidonic acid cascade to bedside prescribing decisions, covering every drug class in NMC competency PH2.7.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed. Jaypee; 2019. Ch 14 (Non-steroidal anti-inflammatory drugs & analgesic-antipyretics) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. McGraw-Hill; 2018. Ch 34 (Anti-inflammatory, antipyretic, and analgesic agents) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old software engineer with a history of chronic knee pain due to osteoarthritis visits your clinic. He has been taking ibuprofen 400 mg three times daily for the past three months and now presents with epigastric pain and black tarry stools. His haemoglobin is 9.2 g/dL. His colleague, who has the same knee pain, had been on celecoxib and has no GI complaints. Meanwhile, a third colleague has been managing his mild headaches with paracetamol and asks: 'Is paracetamol an anti-inflammatory?' How do you answer, and what does this case teach you about choosing between an NSAID and a coxib?
WHY THIS MATTERS
Non-opioid analgesics are the first rung of the WHO analgesic ladder and are the most prescribed drugs globally. In India, self-medication with NSAIDs (particularly diclofenac and ibuprofen) is extremely common. NSAID-related upper GI bleeding causes approximately 1–2% of hospitalised patients to present with acute haemorrhage — a largely preventable iatrogenic event. Understanding COX selectivity, patient risk factors, and contraindications allows you to prescribe these drugs effectively while protecting vulnerable patients. NMC competency PH2.7 is directly tested through prescribing OSCEs, ward-based case discussions, and pharmacology written papers.
RECALL
Before proceeding, recall three foundational concepts:
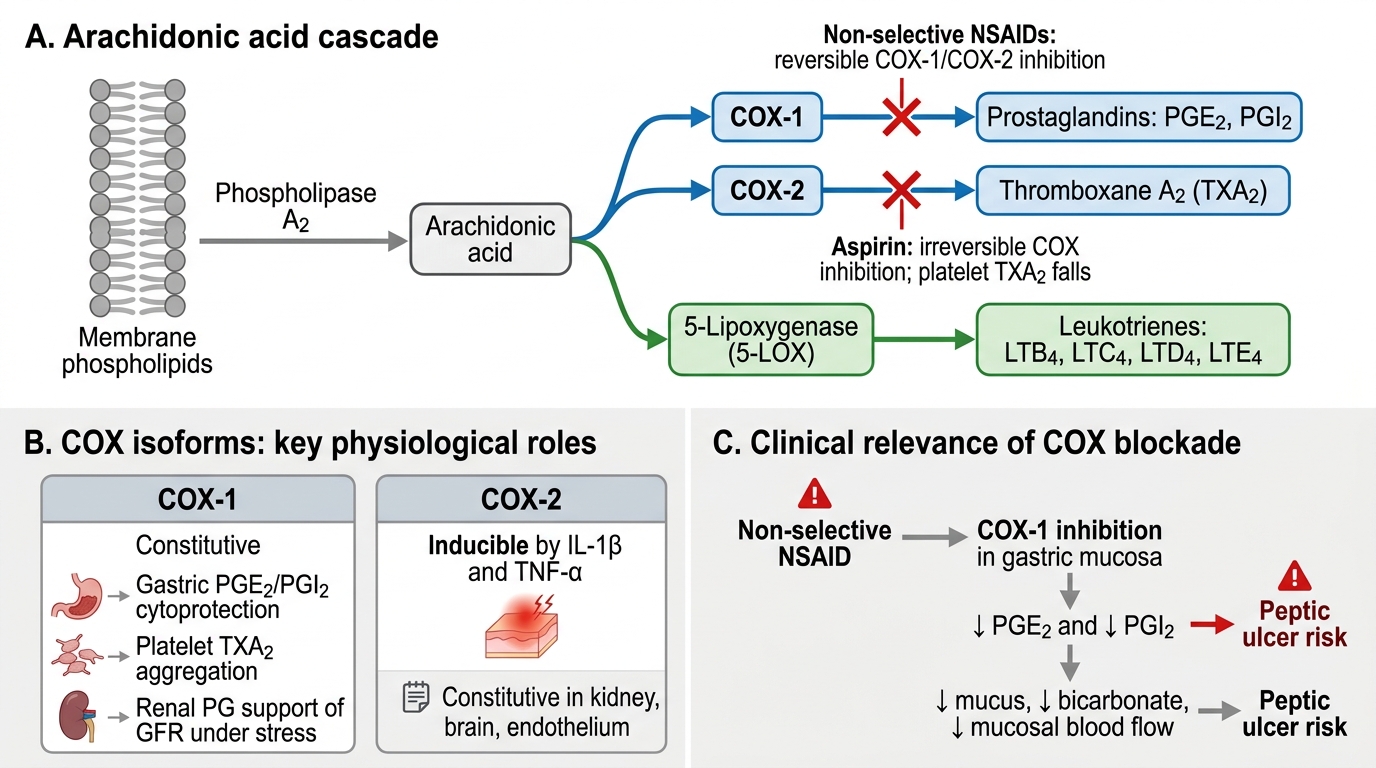
- Arachidonic acid pathway: Membrane phospholipids are cleaved by phospholipase A2 (stimulated by inflammation/injury) to release arachidonic acid. This enters two divergent pathways: the cyclo-oxygenase (COX) pathway, generating prostaglandins and thromboxane A2; and the lipoxygenase (LOX) pathway, generating leukotrienes. NSAIDs act on the COX branch.
- COX-1 vs COX-2 functions: COX-1 is constitutively expressed and produces prostaglandins that protect the gastric mucosa (by stimulating mucus/bicarbonate secretion and mucosal blood flow), maintain renal blood flow, and synthesise platelet TXA2 (promoting aggregation). COX-2 is primarily inducible at sites of inflammation and produces pro-inflammatory prostaglandins (PGE2, PGI2) that sensitise nociceptors and cause fever.
- Pain definitions: Nociception is the detection of noxious stimuli. Peripheral sensitisation occurs when inflammatory mediators (PGE2, bradykinin) lower the threshold of nociceptors, producing primary hyperalgesia. Central sensitisation (wind-up) produces secondary hyperalgesia and allodynia via NMDA receptor activation in the dorsal horn.
Pathophysiology of Pain and the Prostaglandin Pathway
Pain is defined by the International Association for the Study of Pain (IASP) as 'an unpleasant sensory and emotional experience associated with actual or potential tissue damage.' At the tissue level, injury or inflammation triggers the release of a cascade of chemical mediators — histamine, bradykinin, substance P, and prostaglandins — that act on peripheral nociceptors (free nerve endings of Aδ and C fibres) to initiate pain signalling.
The central role of prostaglandins in pain amplification begins at the plasma membrane. Phospholipase A2 is activated by tissue injury, releasing arachidonic acid from membrane phospholipids. Arachidonic acid is the substrate for both the cyclo-oxygenase (COX) and lipoxygenase (LOX) pathways. The COX pathway generates prostaglandins (PGE2, PGD2, PGF2α) and thromboxane A2 (TXA2) via the sequential actions of COX and isomerases. PGE2 is the principal prostaglandin responsible for sensitising peripheral nociceptors — it lowers their firing threshold, producing hyperalgesia (exaggerated response to painful stimuli) and allodynia (pain from normally non-painful stimuli). PGE2 also acts on the hypothalamic thermostat via EP receptors to elevate the set-point, producing fever.
Arachidonic Acid Cascade and NSAID Sites of Action
Two isoforms of COX exist with distinct physiological roles. COX-1 is constitutively expressed in most tissues, including the gastric mucosa (where PGE2 and PGI2 protect the epithelium), platelets (where TXA2 drives aggregation), and kidneys (where PGs maintain glomerular filtration rate under haemodynamic stress). COX-2 is predominantly inducible by inflammatory cytokines (IL-1β, TNF-α) at sites of tissue injury; however, it is constitutively expressed in the kidney, brain, and endothelium. Understanding these two isoforms is the key to predicting every major adverse effect of NSAIDs.
SELF-CHECK
Which of the following correctly explains why non-selective NSAIDs cause peptic ulceration?
A. They directly irritate the gastric mucosa only when taken without food
B. They inhibit COX-1, reducing prostaglandin synthesis that normally maintains gastric mucosal cytoprotection
C. They stimulate COX-2 in the gastric mucosa, increasing pro-inflammatory prostaglandins
D. They block H2 receptors on parietal cells, increasing gastric acid
Reveal Answer
Answer: B. They inhibit COX-1, reducing prostaglandin synthesis that normally maintains gastric mucosal cytoprotection
Non-selective NSAIDs inhibit COX-1 in the gastric mucosa. COX-1 generates PGE2 and PGI2, which stimulate mucus and bicarbonate secretion, maintain mucosal blood flow, and suppress acid secretion. Inhibiting COX-1 removes this cytoprotection, leading to mucosal erosion and ulceration. The effect occurs even with IV or rectal NSAID administration (not merely local irritation), confirming it is a systemic prostaglandin-mediated mechanism.
Therapeutic Goals: Analgesia, Anti-inflammation, and Antipyresis
The three therapeutic goals — analgesia, anti-inflammation, and antipyresis — are related but mechanistically separable, and not every non-opioid analgesic achieves all three. Understanding which drug does what prevents irrational prescribing.
Analgesia (pain relief) is achieved through two routes: peripherally, by inhibiting prostaglandin synthesis and thereby preventing sensitisation of nociceptors; and centrally, by reducing prostaglandin-mediated facilitation of pain transmission in the spinal cord and brain. Most NSAIDs act primarily peripherally; paracetamol has a more prominent central mechanism. Opioids, by contrast, act entirely centrally via μ-opioid receptors — they are outside the scope of this module but are the third rung of the WHO analgesic ladder.
Anti-inflammation requires inhibition of prostaglandin synthesis at the inflamed tissue. This is where COX-2 inhibition is the critical target. Paracetamol — a crucial distinction — does NOT produce clinically meaningful anti-inflammatory effects at therapeutic doses, because it does not meaningfully inhibit COX-1 or COX-2 at the concentration achieved in inflamed peripheral tissue. Its mechanism is debated (possible inhibition of a variant COX isoform in the CNS, or action on the endocannabinoid system), but the clinical implication is clear: paracetamol is an analgesic and antipyretic, not an anti-inflammatory. A patient with rheumatoid arthritis needs an anti-inflammatory — paracetamol alone is inadequate.
Antipyresis is achieved by inhibiting prostaglandin synthesis (PGE2) in the hypothalamic thermostat region, restoring the set-point to normal. Both NSAIDs and paracetamol are effective antipyretics via this central COX-inhibiting mechanism. This is why paracetamol, despite lacking peripheral anti-inflammatory action, is an effective fever reducer.
The WHO analgesic ladder (three-step approach) places non-opioid analgesics at Step 1 (mild-to-moderate pain), with opioids added at Steps 2–3 for moderate-to-severe pain. Effective pain management requires starting at the appropriate step based on pain severity, then escalating systematically.
Classification of Non-Opioid Analgesics
Non-opioid analgesics fall into four main groups, distinguished by their mechanism, chemical structure, and the relative importance of anti-inflammatory activity.
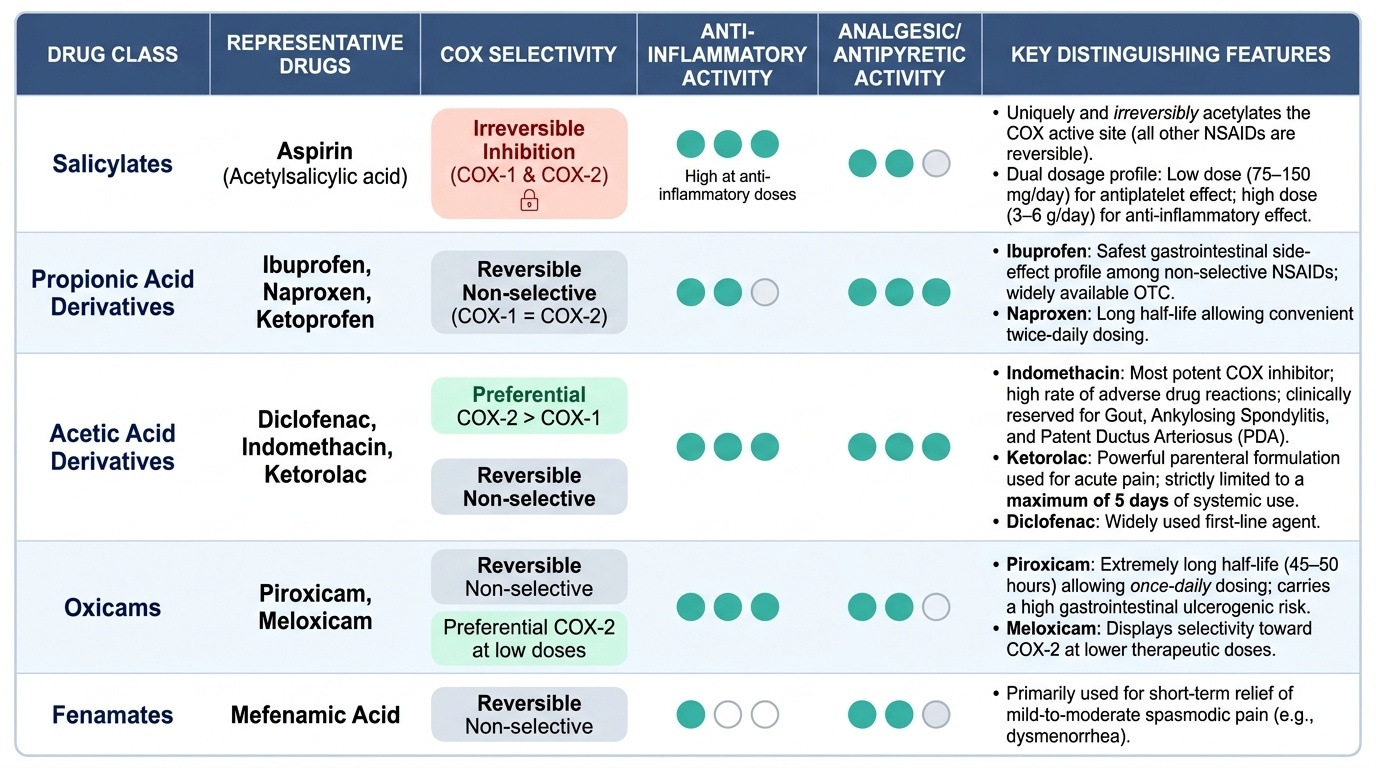
Group 1: Non-selective NSAIDs — These inhibit both COX-1 and COX-2, providing analgesia, anti-inflammation, and antipyresis, but at the cost of COX-1-mediated gastric and platelet effects. Subclasses include:
- Salicylates: aspirin (acetylsalicylic acid) — the prototype; at low doses (75–150 mg/day) used as an antiplatelet agent; at anti-inflammatory doses (3–6 g/day) an NSAID. Uniquely, aspirin irreversibly acetylates the COX active site — all other NSAIDs are reversible inhibitors.
- Propionic acid derivatives: ibuprofen (safest GI profile among non-selective NSAIDs; over-the-counter in many countries), naproxen (longer half-life, twice-daily dosing), ketoprofen.
- Acetic acid derivatives: diclofenac (preferential COX-2 > COX-1 at standard doses; widely used in India), indomethacin (most potent COX inhibitor; reserved for gout, ankylosing spondylitis, patent ductus arteriosus; high ADR rate), ketorolac (strong parenteral analgesic; maximum 5-day systemic use only).
- Oxicams: piroxicam (once-daily, long half-life 45–50 hours; high ulcerogenic risk), meloxicam (preferential COX-2 inhibitor at low doses, non-selective at higher doses).
- Fenamates: mefenamic acid (blocks prostaglandin synthesis AND receptors; short-term only; dysmenorrhoea).
Group 2: Selective COX-2 inhibitors (coxibs) — Designed to provide anti-inflammatory analgesia while sparing COX-1 (and thus gastric mucosa and platelet function). Key drugs: celecoxib, etoricoxib, parecoxib (parenteral). Trade-off: by inhibiting COX-2-derived PGI2 (prostacyclin) in the endothelium without suppressing COX-1-derived TXA2 in platelets, coxibs tip the prostacyclin/thromboxane balance toward platelet aggregation and vasoconstriction, increasing cardiovascular risk (MACE — myocardial infarction, stroke). This mechanism led to the withdrawal of rofecoxib (Vioxx) in 2004 following the APPROVe trial.
Group 3: Para-aminophenol derivatives — Paracetamol (acetaminophen): analgesic and antipyretic without meaningful peripheral anti-inflammatory activity. Mechanism is debated — likely central COX inhibition, endocannabinoid system modulation, or inhibition of a CNS-specific COX variant. Hepatotoxicity is the critical toxicity: dose-dependent, mediated by the reactive metabolite NAPQI (N-acetyl-p-benzoquinone imine) when glutathione stores are exhausted.
Group 4: Pyrazolone derivatives — Metamizole (dipyrone): analgesic, antipyretic, spasmolytic; widely used in India and Europe despite risk of agranulocytosis (rare but potentially fatal). Withdrawn in USA, UK, and some other countries.
Provided image