Page 7 of 15
PH2.8 | PH2.8 | Case-Based Anti-Inflammatory Therapeutics — SDL Guide — SDL Guide
Learning Objectives
- Devise a complete management plan for a case of acute and chronic gout using appropriate anti-inflammatory and urate-lowering drugs.
- Formulate a management plan for osteoarthritis and rheumatoid arthritis, distinguishing the pharmacological strategies for each.
- Construct a management plan for acute migraine attack and migraine prophylaxis, selecting appropriate drugs based on patient profile.
- Identify common prescribing errors (e.g., starting allopurinol during an acute gout attack) and explain the pharmacological rationale.
INSTRUCTIONS
This module shifts from 'what do drugs do' to 'how do I use them.' NMC competency PH2.8 is explicitly about devising management plans — not just listing drugs. Three common clinical presentations — gout, arthritis, and migraine — demand distinct strategies. Some share the same drug class but use it differently; others require combinations that would be harmful if applied to the wrong condition. This module trains you to think in the way a prescriber must: starting from the patient's presentation and building a rational, sequenced plan.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed. Jaypee; 2019. Ch 14 (Drugs used in gout, rheumatoid arthritis) and Ch 31 (Migraine and other headaches) (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed. McGraw-Hill; 2018. Ch 34 (Gout and uricosuric agents), Ch 25 (Migraine treatment) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients walk into your outpatient clinic in the same afternoon:
- Patient A, 52-year-old man: woke up at 3 AM with excruciating pain, swelling, and redness of his right big toe. His serum uric acid is 9.8 mg/dL. He is on hydrochlorothiazide for hypertension.
- Patient B, 55-year-old woman: bilateral symmetric hand joint pain and morning stiffness lasting >1 hour for the past 6 months. Her RF and anti-CCP are positive. She tried ibuprofen — it helps the pain but her joints are still swollen.
- Patient C, 28-year-old woman: recurrent severe unilateral throbbing headache with nausea and photophobia, 3–4 times a month. Simple paracetamol barely touches it.
All three need you to devise a management plan using appropriate pharmacology. Each condition requires a distinct strategy. Where do you start, and how do you reason through each one?
WHY THIS MATTERS
Gout, arthritis, and migraine collectively account for millions of outpatient visits in India every year. Gout is increasingly prevalent in the context of dietary change and diuretic use. Rheumatoid arthritis causes progressive joint destruction if not adequately treated early. Migraine is the sixth leading cause of years lived with disability globally. The drugs used across these three conditions overlap — NSAIDs appear in all three — but the strategies and sequences differ fundamentally. Being able to devise a complete management plan (not just name a drug) is a core clinical competency that will be tested in final MBBS pharmacology practical examinations and ward rounds.
RECALL
This module builds directly on PH2.7 (NSAIDs and non-opioid analgesics). Before proceeding, confirm these connections:
- Indomethacin (acetic acid NSAID) is among the most potent COX inhibitors and has been a traditional first-choice NSAID for acute gout — though naproxen and celecoxib are now also standard.
- Prostaglandins drive inflammation in both arthritis and gout; this is why NSAIDs are useful in both conditions. But arthritis — especially RA — has an additional autoimmune component that NSAIDs alone cannot modify.
- Uric acid is the end product of purine metabolism: adenine and guanine → hypoxanthine/xanthine → uric acid via xanthine oxidase. Hyperuricaemia (serum UA >7 mg/dL in men, >6 mg/dL in women) predisposes to monosodium urate crystal deposition in joints, bursae, and tendons — the substrate for gout.
Pathophysiology of Gout, Arthritis, and Migraine: Setting the Clinical Stage
Understanding why these three conditions require different drugs begins with understanding their different pathophysiological drivers.
Gout is a crystal-induced inflammatory arthropathy. When serum uric acid persistently exceeds its solubility limit (~6.8 mg/dL at body temperature), monosodium urate (MSU) crystals deposit in articular and periarticular tissues. During an acute attack, MSU crystals activate the NLRP3 inflammasome in synovial macrophages, triggering massive release of IL-1β and recruitment of neutrophils. Neutrophils attempt to phagocytose the crystals, releasing lysosomal enzymes and reactive oxygen species that perpetuate the intense inflammatory response — the cardinal hot, swollen, exquisitely tender joint of acute gout. Chronic hyperuricaemia leads to tophi (subcutaneous urate deposits) and chronic gouty arthritis with joint destruction.
Osteoarthritis (OA) is a degenerative joint disease driven by mechanical stress and age-related cartilage degradation. Chondrocyte-derived matrix metalloproteinases break down type II collagen and proteoglycans; subchondral bone remodelling and osteophyte formation follow. Inflammation in OA is secondary — less intense than RA — and NSAIDs primarily provide symptomatic relief rather than disease modification.
Rheumatoid arthritis (RA) is an autoimmune disease in which autoreactive T lymphocytes and B cells target synovial tissue, producing rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA/anti-CCP). Synovial macrophages and fibroblasts produce TNF-α, IL-1β, and IL-6, driving pannus formation — an invasive synovial tissue that erodes cartilage and bone. NSAIDs relieve RA symptoms but do NOT halt pannus-mediated joint destruction. Only disease-modifying antirheumatic drugs (DMARDs) — primarily methotrexate — prevent progressive structural damage.
Migraine is a complex neurovascular disorder. The current prevailing model involves cortical spreading depression (CSD) — a wave of neuronal and glial depolarisation that propagates across the cortex, initiating the aura phase. CSD activates the trigeminovascular system: trigeminal nerve endings around meningeal vessels release calcitonin gene-related peptide (CGRP), a potent vasodilator and neuroinflammatory mediator. This causes sterile meningeal inflammation and vasodilation, transmitting pain signals via the trigeminal nucleus caudalis to the thalamus and cortex — the pulsating, photophobic headache. The sensitisation of central pain neurons during this process explains why routine activities amplify migraine pain.
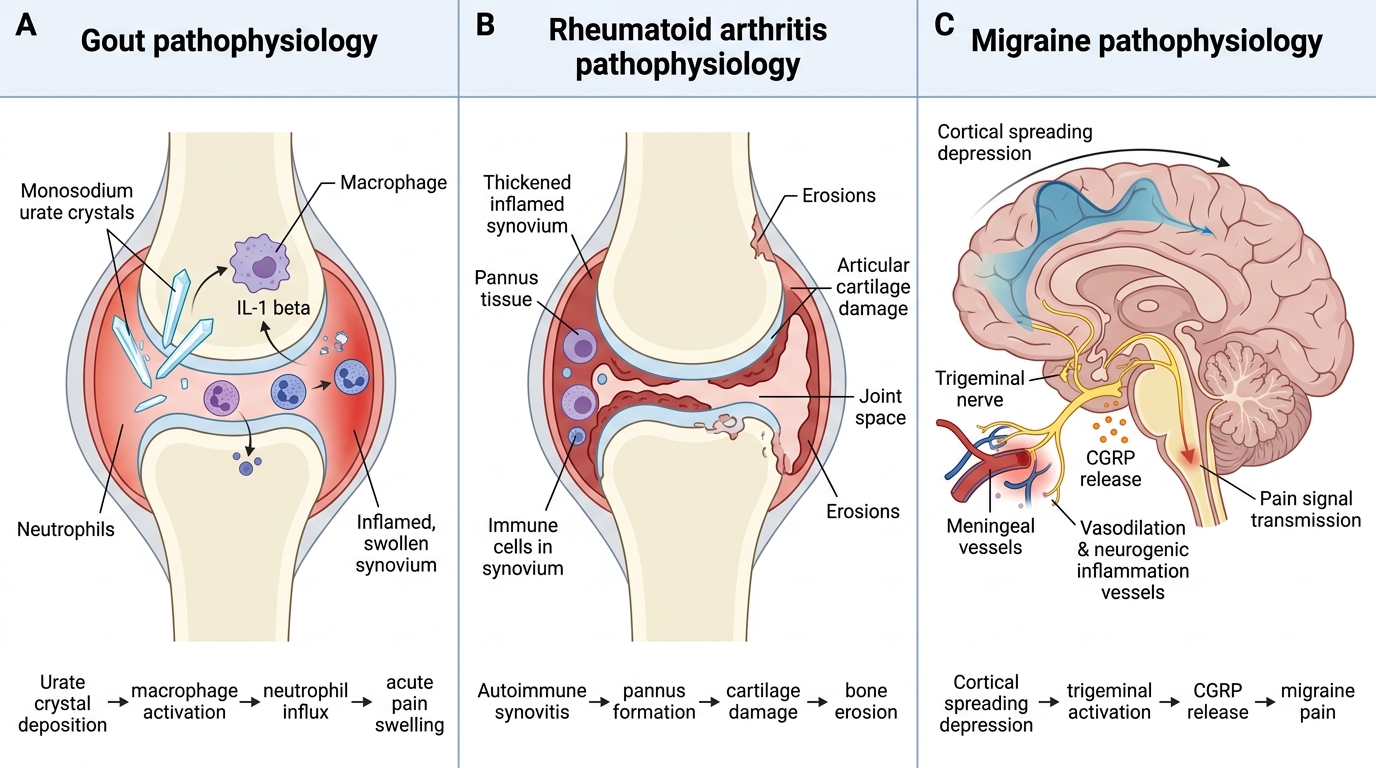
Pathophysiology of Gout, Rheumatoid Arthritis, and Migraine
SELF-CHECK
A patient with acute gout is prescribed a drug to lower his uric acid levels. He is started on allopurinol immediately. Three days later his gout attack has worsened. Why?
A. Allopurinol directly stimulates neutrophil recruitment in the joint
B. Allopurinol rapidly mobilises urate from tissue deposits, causing fluctuating serum uric acid levels that can precipitate or prolong acute attacks
C. Allopurinol inhibits COX-1, reducing gastric prostaglandins and worsening GI-related pain
D. Allopurinol increases IL-1β secretion from synovial macrophages
Reveal Answer
Answer: B. Allopurinol rapidly mobilises urate from tissue deposits, causing fluctuating serum uric acid levels that can precipitate or prolong acute attacks
Initiating urate-lowering therapy (including allopurinol) during an acute gout attack is a classic prescribing error. Rapid changes in serum uric acid levels — even a fall — destabilise existing urate deposits in the joint, causing crystal shedding and prolonging or worsening the acute attack. Allopurinol must be started only AFTER the acute attack has fully resolved (typically 2–4 weeks later), and colchicine prophylaxis should be co-prescribed for the first 3–6 months of ULT to prevent mobilisation-triggered flares.
Therapeutic Goals for Gout, Arthritis, and Migraine
Each condition has distinct immediate and long-term therapeutic goals. Conflating these leads to either under-treatment (failing to start DMARDs in RA) or harmful sequencing errors (starting allopurinol during acute gout).
Gout — dual-phase goals:
- Acute phase: Rapidly terminate the inflammatory attack and relieve pain within 24–48 hours. Anti-inflammatory drugs are the priority.
- Interval (chronic) phase: Lower serum uric acid to below the saturation threshold (<6 mg/dL; <5 mg/dL in tophaceous gout) using urate-lowering therapy (ULT) to prevent future attacks, dissolve tophi, and protect joints and kidneys. These goals are sequential — the acute attack must fully resolve before ULT is initiated.
Osteoarthritis — symptomatic goals:
OA has no drug that reverses cartilage loss or modifies disease progression. Goals are entirely symptomatic: reduce pain, maintain joint function, preserve quality of life. Non-pharmacological measures (physiotherapy, weight reduction, orthotic supports) are co-equal to pharmacotherapy. Drug therapy is escalated stepwise from paracetamol to NSAIDs to intra-articular injections.
Rheumatoid arthritis — two intertwined goals:
- Symptom control: Reduce pain, swelling, and morning stiffness — achievable with NSAIDs.
- Disease modification: Halt or slow structural joint damage (erosion, cartilage loss) — achievable ONLY with DMARDs. The principle of 'treat-to-target' (achieving remission or low disease activity as measured by clinical and inflammatory markers) drives modern RA management. Early DMARD initiation (ideally within 3–6 months of diagnosis) significantly improves long-term outcomes.
Migraine — acute vs preventive goals:
- Acute attack: Abort the headache rapidly, restore function, and avoid analgesic overuse (medication overuse headache is a complication of frequent analgesic use).
- Prophylaxis: Reduce attack frequency by ≥50%, decrease severity, and prevent analgesic overuse. Initiated when attacks are ≥4 per month, or when each attack is severely debilitating, or when acute medications fail or are contraindicated.
Therapeutic Goals and Drug Strategies in Autacoid-Related Disorders
Drug Classes Used in Each Condition
Mapping the right drug class to the right condition is the clinical application of the pharmacology covered in PH2.6 and PH2.7. This section provides the framework before the case-based management plans.
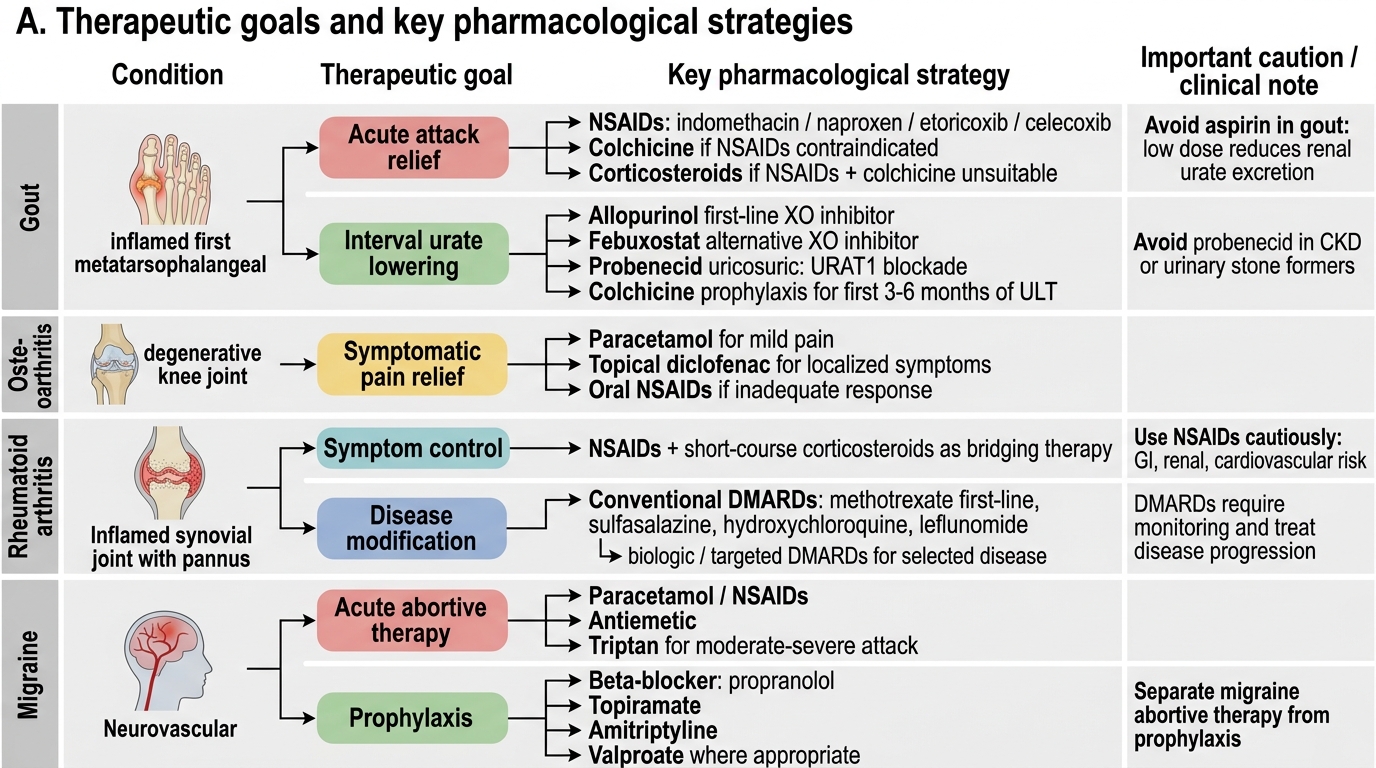
Gout — drug mapping:
- Acute attack: NSAIDs (indomethacin, naproxen, etoricoxib, celecoxib); colchicine (especially when NSAIDs are contraindicated); systemic corticosteroids (prednisolone oral or intra-articular injection) when both NSAIDs and colchicine are contraindicated (e.g., severe CKD). Do NOT use aspirin — at low doses it decreases renal urate excretion and can worsen hyperuricaemia.
- Interval phase (ULT): Allopurinol (xanthine oxidase inhibitor — first-line); febuxostat (selective XO inhibitor — alternative, especially with allopurinol hypersensitivity or azathioprine co-use caution); probenecid (uricosuric — blocks URAT1 renal reabsorption, avoid in urinary stone formers and CKD). Colchicine prophylaxis (0.5 mg once or twice daily) during the first 3–6 months of ULT initiation.
Osteoarthritis — drug mapping:
- Step 1: Paracetamol (1 g up to 4 times daily) — first-line for mild pain; topical NSAIDs (diclofenac gel) for localised joint symptoms.
- Step 2: Oral NSAIDs (ibuprofen, naproxen, diclofenac) — add PPI if GI risk present.
- Step 3: Intra-articular corticosteroid injections (short-term relief); intra-articular hyaluronic acid (variable evidence).
- Symptomatic slow-acting drugs (SSAODs): glucosamine sulfate, chondroitin — limited but positive evidence in some patients.
Rheumatoid arthritis — drug mapping:
- Symptomatic: NSAIDs (step-appropriate as in OA); short-course corticosteroids as bridge therapy at initiation.
- Disease-modifying (conventional synthetic DMARDs): Methotrexate (anchor; 7.5–25 mg/week oral or SC + folic acid supplementation); hydroxychloroquine (mild disease or triple combination); sulfasalazine; leflunomide. Triple therapy (MTX + HCQ + SSZ) is often used.
- Biologic DMARDs (for inadequate DMARD response): TNF-α inhibitors (adalimumab, etanercept), IL-6 inhibitors (tocilizumab), JAK inhibitors (baricitinib, tofacitinib) — beyond PH2.8 scope but important for context.
Migraine — drug mapping:
- Acute mild-moderate: Paracetamol + metoclopramide (prokinetic enhances paracetamol absorption); simple NSAIDs (ibuprofen, naproxen).
- Acute moderate-severe: Triptans — sumatriptan (oral 50–100 mg or SC 6 mg), rizatriptan, zolmitriptan — selective 5-HT1B/1D receptor agonists that constrict dilated meningeal vessels and inhibit trigeminal nociceptive neurotransmission.
- Older acute agents: Ergotamine (non-selective vasoconstrictor; more side effects; not first-line); ergotamine tartrate + caffeine (Cafergot).
- Prophylaxis: Propranolol (40–240 mg/day) — first-line; topiramate (25–200 mg/day) — first-line; amitriptyline (10–75 mg at bedtime) — second-line; sodium valproate (500–1000 mg/day) — effective but teratogenic, avoid in women of childbearing potential.
- Anti-CGRP monoclonal antibodies (erenumab, fremanezumab): newer biologic prophylaxis, beyond routine PH2.8 scope.
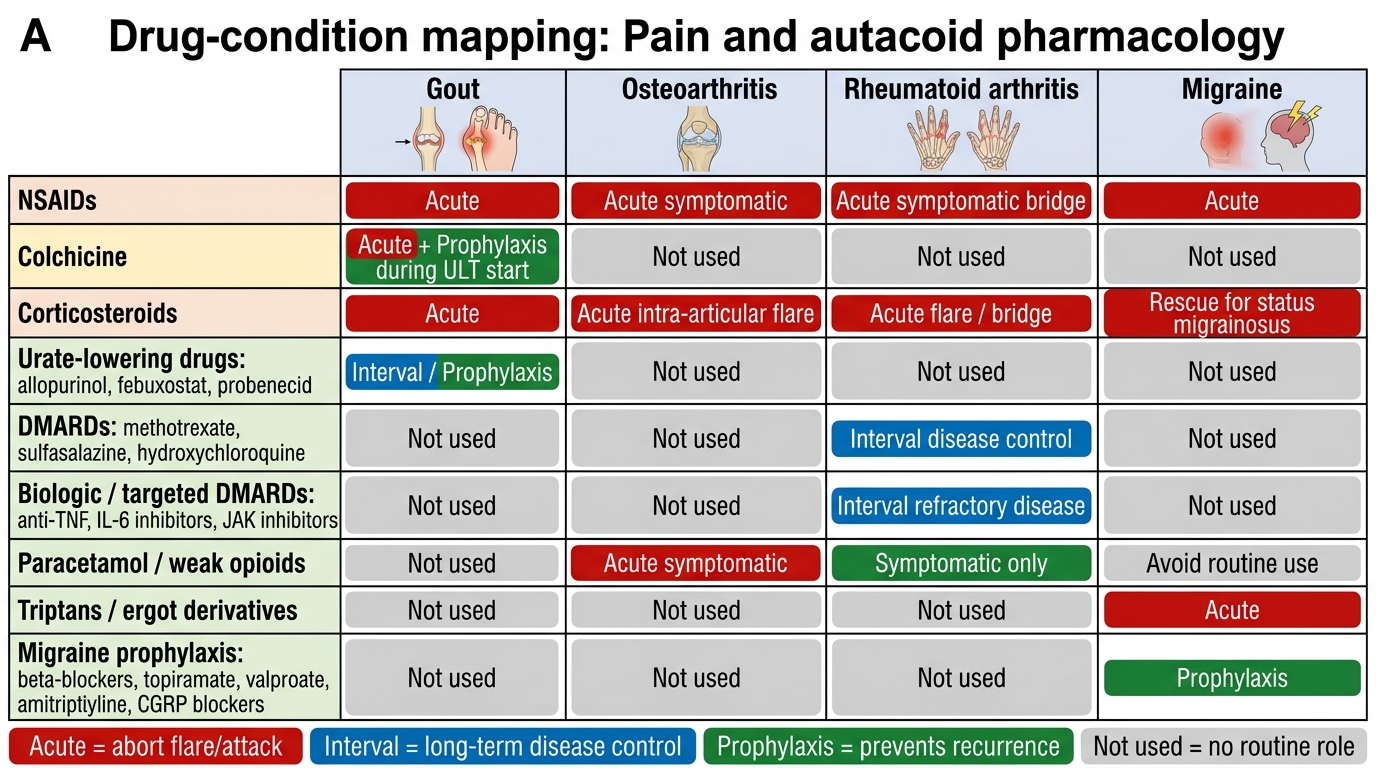
Drug Roles in Gout, Arthritis, and Migraine