Page 8 of 15
PH2.8 | PH2.8 | Case-Based Anti-Inflammatory Therapeutics — SDL Guide — SDL Guide (Part 2)
Management Plan for Acute and Chronic Gout
Patient A (52-year-old man, acute right first MTP joint attack, UA=9.8 mg/dL, on hydrochlorothiazide) provides the template for a complete gout management plan.
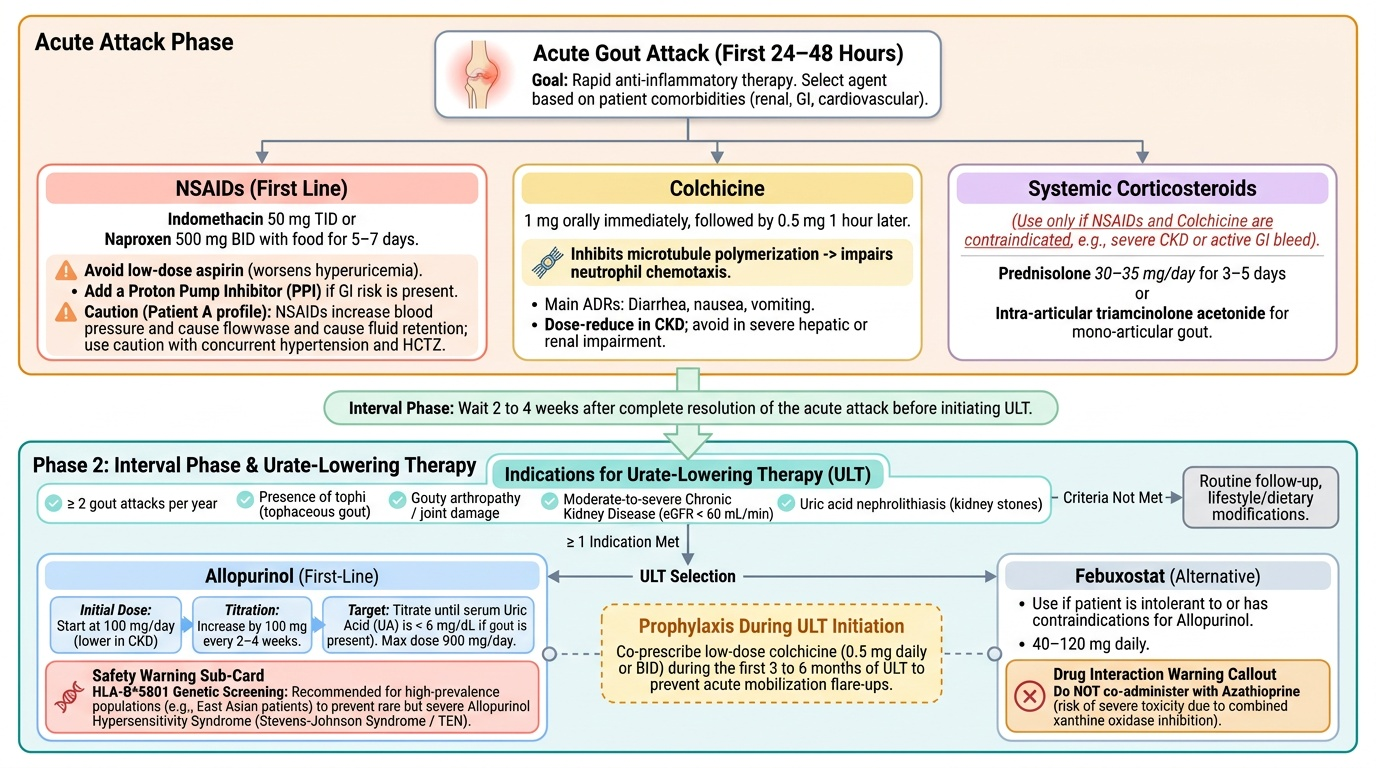
Acute attack management (first 24–48 hours):
The goal is rapid anti-inflammatory therapy. Three options exist; select based on the patient's renal function, GI history, and co-morbidities:
- NSAIDs (first choice if no contraindication): Indomethacin 50 mg three times daily or naproxen 500 mg twice daily, taken with food, for 5–7 days. Avoid aspirin (worsens hyperuricaemia at low doses). Consider adding a PPI if GI risk is present. For Patient A (on hydrochlorothiazide, possibly hypertensive), be mindful that NSAIDs can raise blood pressure and cause fluid retention.
- Colchicine (if NSAIDs are contraindicated or poorly tolerated): Low-dose regimen: 1 mg orally, then 0.5 mg one hour later. Main ADRs: diarrhoea, nausea, vomiting. Dose-reduce in CKD; avoid in severe hepatic or renal impairment. Its mechanism is unique — it inhibits microtubule polymerisation, impairing neutrophil chemotaxis to the urate crystal site, thereby blunting the inflammatory cascade.
- Systemic corticosteroids (if both NSAIDs and colchicine are contraindicated — e.g., severe CKD, severe GI disease): Prednisolone 30–35 mg/day for 3–5 days, or intra-articular triamcinolone acetonide for mono-articular gout.
Interval management and urate-lowering therapy (ULT):
Wait until the acute attack has fully resolved (typically 2–4 weeks) before initiating ULT. Indications for starting ULT: ≥2 gout attacks per year; presence of tophi; gouty arthropathy or joint damage; CKD (eGFR <60 mL/min); uric acid nephrolithiasis.
- Allopurinol (first-line ULT): Start at 100 mg/day, increase by 100 mg every 2–4 weeks until target UA <6 mg/dL is achieved (or <5 mg/dL in tophaceous gout). Maximum dose 900 mg/day. Do not start during an acute attack. Important: allopurinol hypersensitivity syndrome (rare but severe — Stevens-Johnson syndrome, TEN) is more common in HLA-B*5801 carriers (East Asian patients) — genetic screening is recommended in high-prevalence populations.
- Febuxostat (alternative if allopurinol intolerant or contraindicated): More selective xanthine oxidase inhibitor; 40–120 mg daily. Note: febuxostat should NOT be co-administered with azathioprine (both inhibit XO — azathioprine toxicity risk).
- Probenecid (uricosuric agent): Increases renal urate excretion by inhibiting URAT1. Avoid in patients with urinary uric acid overexcretion, uric acid nephrolithiasis, or eGFR <30 mL/min.
- Colchicine prophylaxis during ULT initiation: 0.5 mg once or twice daily for the first 3–6 months of ULT, to prevent mobilisation-triggered flares as urate deposits dissolve.
For Patient A specifically: Review and if possible discontinue or switch hydrochlorothiazide (thiazide diuretics reduce renal urate excretion, raising serum uric acid). If antihypertensive is needed, losartan (ARB) has mild uricosuric properties and is preferred. Dietary advice: reduce purine-rich foods (red meat, shellfish, organ meat), limit alcohol (especially beer — high in purines), avoid high-fructose corn syrup beverages. Maintain adequate hydration.
Provided image
SELF-CHECK
A patient with recurrent gout has chronic kidney disease (eGFR 25 mL/min). During an acute attack, which drug is the MOST appropriate anti-inflammatory treatment?
A. High-dose indomethacin 50 mg three times daily for 7 days
B. Allopurinol 300 mg daily, started immediately
C. Oral prednisolone 30 mg daily for 3–5 days
D. Probenecid for rapid uricosuric effect
Reveal Answer
Answer: C. Oral prednisolone 30 mg daily for 3–5 days
In severe CKD (eGFR 25 mL/min), both NSAIDs (risk of further AKI) and colchicine (accumulates in renal failure, causing severe GI and neuromuscular toxicity) are contraindicated or high-risk. Systemic corticosteroids (prednisolone 30–35 mg/day for 3–5 days) are the safe alternative in this setting. Allopurinol must never be started during an acute attack (worsens or prolongs the flare). Probenecid is contraindicated in CKD (eGFR <30 mL/min) and has no role in acute attack management.
Management Plan for Osteoarthritis and Rheumatoid Arthritis
Patient B (55-year-old woman, bilateral symmetric hand arthritis, morning stiffness >1 hour, positive RF and anti-CCP) has RA — not OA. The management plan for RA differs fundamentally from OA. Conflating the two is a significant prescribing error.
Osteoarthritis management (for comparison):
OA is managed symptomatically in a stepwise fashion. Step 1: paracetamol (1 g up to 4 times daily) and topical NSAIDs (diclofenac gel) for localised joint symptoms — preferred in older patients and those with systemic NSAID risks. Step 2: Oral NSAIDs with PPI co-prescription in patients with GI risk. Step 3: intra-articular corticosteroid injection for flare relief. No DMARDs are used in OA — the disease is not autoimmune. Non-pharmacological measures (weight reduction, physiotherapy, assistive devices) are as important as pharmacotherapy.
Rheumatoid arthritis — integrated management plan:
For Patient B, NSAIDs alone are insufficient — they relieve pain and stiffness but do NOT prevent the joint erosion that ACPA positivity predicts will occur without DMARDs.
Step 1 — Symptom relief while awaiting DMARD onset: Start an NSAID (naproxen 500 mg twice daily with a PPI) for immediate pain and stiffness relief. A short course of oral prednisolone (5–10 mg/day) may be used as bridge therapy during DMARD initiation — corticosteroids are effective anti-inflammatory agents in RA but not suitable for long-term use (osteoporosis, adrenal suppression, infection risk).
Step 2 — Initiate DMARD therapy promptly (ideally within 3 months of diagnosis):
- Methotrexate (MTX) is the anchor DMARD in RA. Starting dose 7.5–15 mg/week orally or subcutaneously, titrated to 25 mg/week if tolerated. Folic acid (5 mg/week, on a different day from MTX) must be co-prescribed to reduce mucosal and haematological side effects of MTX. MTX takes 4–12 weeks to show clinical effect.
- Add hydroxychloroquine (HCQ) 200–400 mg/day for mild-to-moderate RA — it has a good safety profile and is particularly useful in women of childbearing age (safe in pregnancy; one of the few DMARDs that is). Annual ophthalmological monitoring for HCQ retinopathy.
- Sulfasalazine 2–3 g/day may be added for triple combination therapy (MTX + HCQ + SSZ) — shown to be equivalent to biologic therapy in some patients.
Step 3 — Biologic DMARDs for inadequate DMARD response (after 3–6 months of optimised conventional DMARD therapy without reaching remission or low disease activity): TNF-α inhibitors (adalimumab, etanercept), IL-6 receptor inhibitors (tocilizumab), or JAK inhibitors (baricitinib). These are beyond the scope of PH2.8 but important for clinical context.
Critical prescribing reminders for MTX:
- Absolute contraindications: significant hepatic disease, significant renal impairment (MTX is renally excreted — accumulation risk), active infection, pregnancy (teratogenic — Category X).
- Regular monitoring: full blood count (bone marrow suppression), liver enzymes (hepatotoxicity), renal function.
- Drug interaction: NSAIDs + MTX — NSAIDs reduce renal MTX clearance and displace it from protein binding, increasing toxicity risk. If NSAIDs are continued for RA symptoms, monitor carefully or use a different analgesic.
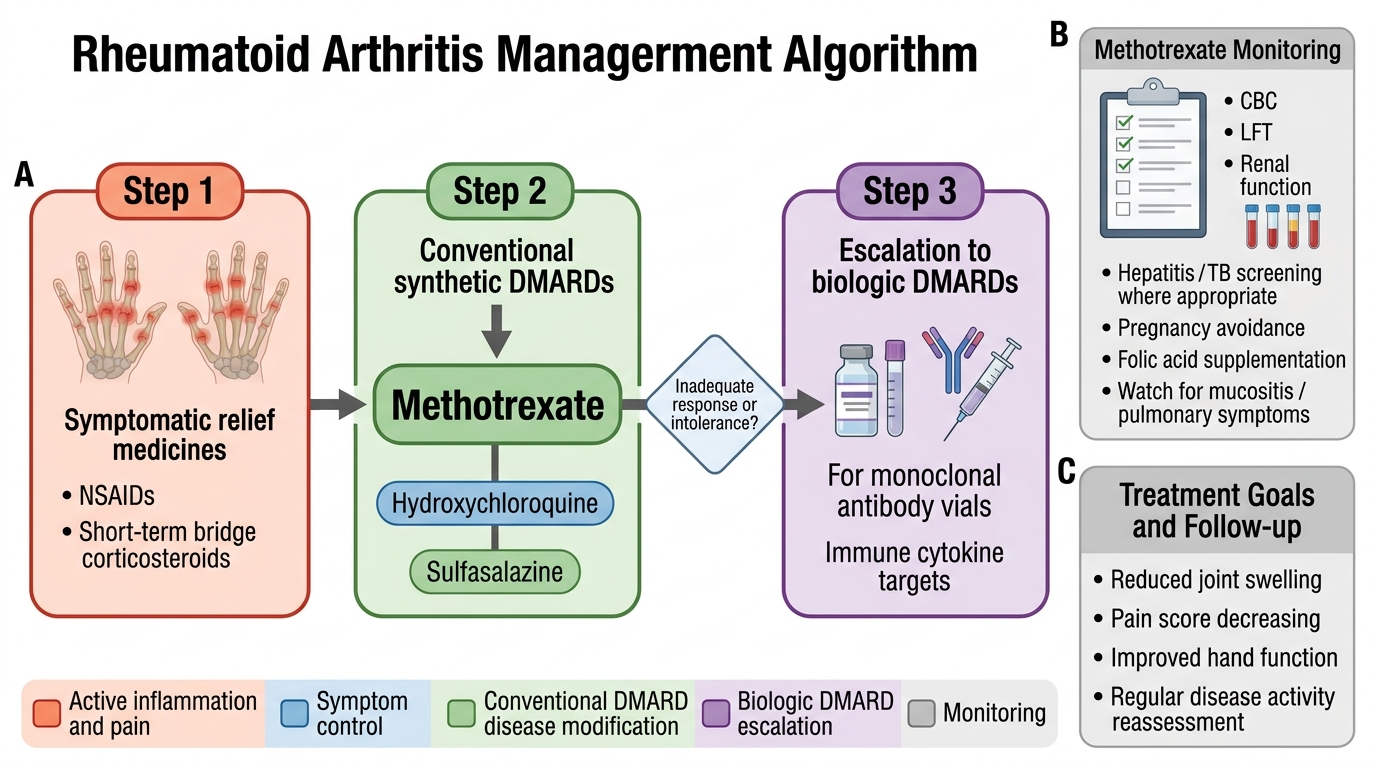
Stepwise Pharmacologic Management of Rheumatoid Arthritis
Management Plan for Migraine
Patient C (28-year-old woman, recurrent severe unilateral throbbing headache with nausea and photophobia, 3–4 attacks per month, inadequate response to paracetamol) has migraine that requires a two-pronged approach: a more effective acute abortive agent AND prophylaxis for attack frequency reduction.
Acute migraine attack management:
The choice of acute medication is stratified by attack severity:
- Mild attacks: Simple analgesics (paracetamol 1 g + metoclopramide 10 mg — the antiemetic also improves gastric motility, enhancing paracetamol absorption during the gastric stasis of migraine). Ibuprofen 400–800 mg is also effective for mild migraine.
- Moderate-to-severe attacks (Patient C's profile): Triptans are the drugs of choice. They are selective 5-HT1B/1D receptor agonists that act by: (1) causing vasoconstriction of dilated meningeal and cerebral vessels, reversing the neurogenic vasodilation; (2) inhibiting the release of CGRP and other neuropeptides from trigeminal terminals (presynaptic 5-HT1D); and (3) blocking pain transmission at the trigeminal nucleus caudalis (central 5-HT1B/1D).
- Sumatriptan: prototype; oral 50–100 mg, SC 6 mg (fastest onset), nasal spray 10–20 mg. Effective in 60–70% of attacks within 2 hours.
- Rizatriptan 10 mg oral: faster onset than sumatriptan; disintegrating tablet for patients with nausea.
- Zolmitriptan 2.5–5 mg: oral and nasal spray.
- Almotriptan, eletriptan, naratriptan (longer half-life, less headache recurrence).
- Contraindications to triptans: Established cardiovascular disease (IHD, CVA, peripheral arterial disease), uncontrolled hypertension, pregnancy, haemiplegic migraine, basilar migraine (relative contraindication due to risk of vasoconstriction in the posterior circulation).
- Ergotamine (older vasoconstrictor): Less selective than triptans; combined with caffeine (Cafergot) to enhance absorption. More side effects (nausea, vomiting, vasoconstriction — contraindicated in coronary artery disease and peripheral vascular disease). Not first-line.
Analgesic overuse caution: Using acute migraine medications (including triptans, ergotamine, and simple analgesics) on >10–15 days per month causes medication overuse headache (MOH) — a paradoxical transformation where the medication intended to abort attacks ends up perpetuating them. Patient C, with 3–4 attacks per month, should begin prophylaxis.
Migraine prophylaxis:
Criteria for prophylaxis: ≥4 migraine days per month; attacks severely impair function despite acute treatment; acute medications are contraindicated or overused; patient preference.
- Propranolol (40–240 mg/day): Non-selective beta-blocker; first-line prophylaxis in most patients. Mechanism in migraine is not fully understood but involves inhibition of adrenergic-mediated vascular reactivity. Contraindicated in asthma, COPD, decompensated heart failure, and diabetes prone to hypoglycaemia.
- Topiramate (25–200 mg/day): First-line; antiepileptic; mechanism includes sodium channel blockade and GABA enhancement. ADRs: cognitive dulling ('dopamax'), weight loss, paraesthesias, nephrolithiasis. Avoid in pregnancy (teratogenic).
- Amitriptyline (10–75 mg at bedtime): Second-line; tricyclic antidepressant; effective for migraine even at sub-antidepressant doses; useful when migraine is comorbid with depression or insomnia. ADRs: sedation, anticholinergic effects, weight gain.
- Sodium valproate (500–1500 mg/day): Effective prophylaxis; strictly contraindicated in women of childbearing potential (teratogenic — neural tube defects, neurodevelopmental harm; PREVENT programme requires special documentation before prescribing). Safe to use in men.
- Flunarizine (5–10 mg at bedtime): Calcium channel blocker; effective prophylaxis; available in India; ADRs include sedation and parkinsonism (long-term).
- Patient C's plan: Given she is a 28-year-old woman, avoid valproate. A reasonable first-choice is propranolol (if no asthma) with amitriptyline as an alternative; topiramate if these are ineffective. For acute attacks, start sumatriptan 50 mg at attack onset (with metoclopramide for nausea), and counsel specifically about avoiding analgesic overuse.
CLINICAL PEARL
Low-Dose Aspirin Worsens Gout — A Counter-Intuitive Drug Interaction: Many patients with recurrent gout also have cardiovascular disease and are on low-dose aspirin (75–150 mg/day) for antiplatelet prophylaxis. At this dose range, aspirin acts on renal proximal tubule OAT (organic anion transporter) transporters to reduce renal uric acid excretion, paradoxically raising serum uric acid and increasing gout attack frequency. This is distinct from the uricosuric effect of high-dose aspirin (>3 g/day), which actually increases renal urate excretion — but that dose is not used clinically for its antiplatelet effect. The prescribing implication: never use low-dose aspirin as the NSAID for acute gout, and if a patient's gout is poorly controlled despite ULT, check whether they are on aspirin and optimise with concurrent allopurinol dosing. Switching the antihypertensive to losartan (mildly uricosuric ARB) when clinically appropriate is a rational therapeutic manoeuvre.
SELF-CHECK
A 28-year-old woman with 4 migraine attacks per month is started on sodium valproate for prophylaxis. What is the most critical counselling point before prescribing valproate in this patient?
A. Valproate must be taken with food to prevent GI side effects
B. Valproate should be avoided in this patient — it is teratogenic and strictly contraindicated in women of childbearing potential without specialist oversight and special documentation
C. Valproate can cause weight gain, so dietary counselling is necessary
D. Valproate must not be combined with propranolol due to drug interaction
Reveal Answer
Answer: B. Valproate should be avoided in this patient — it is teratogenic and strictly contraindicated in women of childbearing potential without specialist oversight and special documentation
Sodium valproate is classified as a highly teratogenic drug (Category X in pregnancy), associated with neural tube defects, craniofacial abnormalities, and neurodevelopmental harm in the exposed foetus. In women of childbearing potential, valproate for migraine prophylaxis is contraindicated unless all other options have failed and reliable contraception is confirmed — and even then, it requires a formalised informed consent programme. Alternatives for migraine prophylaxis in this 28-year-old woman include propranolol, topiramate (with effective contraception counselling — also teratogenic but less severely so), amitriptyline, or flunarizine.