Page 1 of 46
PH8.1-2 | PH8.1-2 | Antimicrobial Principles and Stewardship — SDL Guide — SDL Guide
Learning Objectives
- Discuss general principles of chemotherapy with emphasis on antimicrobial resistance
- Discuss rational use of antimicrobials
- Describe the antibiotic stewardship programme and its components
- Apply stewardship principles to common clinical prescribing decisions
INSTRUCTIONS
Antimicrobial drugs are unique in pharmacology: their target is a living organism inside a living patient. Every prescribing decision balances the need to kill the pathogen against the risk of selecting for resistance and harming the host. This module builds the conceptual foundation — selective toxicity, resistance mechanisms, pharmacokinetic/pharmacodynamic principles — and then translates them into the structured practice of antimicrobial stewardship, preparing you to prescribe responsibly in an era of rising resistance.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 55–57 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 55 (textbook)
- WHO AWaRe Classification 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 40-year-old woman is brought to the emergency department with fever, rigors, and right-flank pain. She was started empirically on intravenous ceftriaxone three days ago at a private clinic, but her fever persists. Urine culture returns Klebsiella pneumoniae — resistant to cephalosporins, fluoroquinolones, and trimethoprim-sulfamethoxazole (TMP-SMX), sensitive only to meropenem and amikacin. Her treating physician wonders: 'Did my empiric choice drive this resistance, or was she already colonised?' And more immediately: 'When do I switch, and what do I switch to?' Every facet of this scenario — the biology of resistance, the logic of drug selection, the role of culture results, the stewardship duty to de-escalate — is grounded in the principles you will learn today.
WHY THIS MATTERS
Antimicrobial resistance has been declared a global health emergency by the WHO, threatening to undo a century of progress in managing infectious disease. India bears a disproportionate burden: it is one of the world's largest consumers of antibiotics, and resistance rates to common agents — fluoroquinolones, third-generation cephalosporins, carbapenems — are among the highest globally. As a prescriber, you are simultaneously a clinician (selecting the right drug for the right patient) and a steward (protecting the antibiotic armamentarium for future patients). The principles in this module are not abstract; they underpin every antimicrobial order you will write for the rest of your career.
RECALL
Before we build on pharmacology, recall these foundations from Year 1:
Microbiology: bacterial cell structure — the peptidoglycan cell wall (absent in humans, target for β-lactams); the 70S ribosome with 30S (aminoglycoside/tetracycline target) and 50S (macrolide/chloramphenicol/clindamycin target) subunits; the DNA-gyrase/topoisomerase IV enzymes (fluoroquinolone target); fungal ergosterol (antifungal target).
Pharmacokinetics: volume of distribution (Vd) governs where a drug goes — drugs with low Vd (e.g. vancomycin, aminoglycosides) stay in plasma/extracellular fluid; drugs with high Vd (e.g. azithromycin) penetrate tissue and cells. Protein binding, half-life, and renal/hepatic clearance determine dosing intervals and adjustment needs.
Host defences: the immune status of the host profoundly modifies antimicrobial choice — immunocompromised patients need broader empiric cover; neutropenic patients are at risk of fatal bacteraemia from organisms ordinarily of low virulence.
Why Antimicrobials Are Different: Problem Framing
Selective toxicity is the cornerstone concept of antimicrobial pharmacology. Unlike most drugs that act on human receptors or enzymes, antimicrobial agents must target structures unique to — or sufficiently different in — the pathogen, while sparing host cells. The ideal antimicrobial exploits a metabolic pathway or structural element that exists in the microorganism but not in the human host. Paul Ehrlich's concept of the 'magic bullet' — a compound that seeks and destroys the pathogen without harming the host — defines this principle. In practice, selective toxicity is never absolute; every antimicrobial has some host toxicity, and the therapeutic window (the ratio of the toxic dose to the effective dose) varies greatly.
The major structural/biochemical targets exploited for selective toxicity include: (1) the bacterial cell wall (peptidoglycan), which has no human equivalent — targeted by β-lactams, vancomycin, and fosfomycin; (2) the 70S bacterial ribosome, which differs structurally from the human 80S ribosome — targeted by aminoglycosides (30S), tetracyclines (30S), macrolides (50S), chloramphenicol (50S), and clindamycin (50S); (3) bacterial DNA-gyrase and topoisomerase IV, which differ from human topoisomerases — targeted by fluoroquinolones; (4) folic acid synthesis, an essential bacterial pathway absent in humans (who absorb dietary folate) — targeted by sulfonamides (inhibit dihydropteroate synthase) and trimethoprim (inhibit dihydrofolate reductase); (5) cell membrane integrity — targeted by polymyxins (bacterial lipopolysaccharide) and the antifungal agents amphotericin B and azoles (fungal ergosterol).
Static vs cidal activity describes the functional outcome of drug-pathogen interaction. A bacteriostatic drug inhibits growth and replication, leaving clearance to the host immune system; if the immune system is impaired, bacteriostatic drugs may fail. A bactericidal drug kills the organism directly. Key groupings:
- Bacteriostatic: tetracyclines, macrolides, sulfonamides (± TMP), chloramphenicol, clindamycin, linezolid
- Bactericidal: β-lactams (penicillins, cephalosporins, carbapenems, monobactams), aminoglycosides, fluoroquinolones, vancomycin, metronidazole, rifampicin, daptomycin
An important exception: aminoglycosides are bactericidal despite inhibiting protein synthesis at the 30S subunit. Unlike tetracyclines (which reversibly block aminoacyl-tRNA attachment), aminoglycosides bind irreversibly to the 30S subunit, cause misreading of the genetic code, and generate aberrant proteins that insert into the membrane — a lethal event independent of replication. This exception is a common exam and clinical point.
The static/cidal distinction also matters clinically: in bacterial endocarditis, meningitis, and infections in immunocompromised hosts, bactericidal agents are strongly preferred because host immune clearance is unreliable.
Governing Principles of Chemotherapy
The efficacy of an antimicrobial is not determined by the blood level alone — it depends on the relationship between the drug's pharmacokinetics (what the body does to the drug) and pharmacodynamics (what the drug does to the organism). Three PK/PD indices predict clinical efficacy and guide dosing:
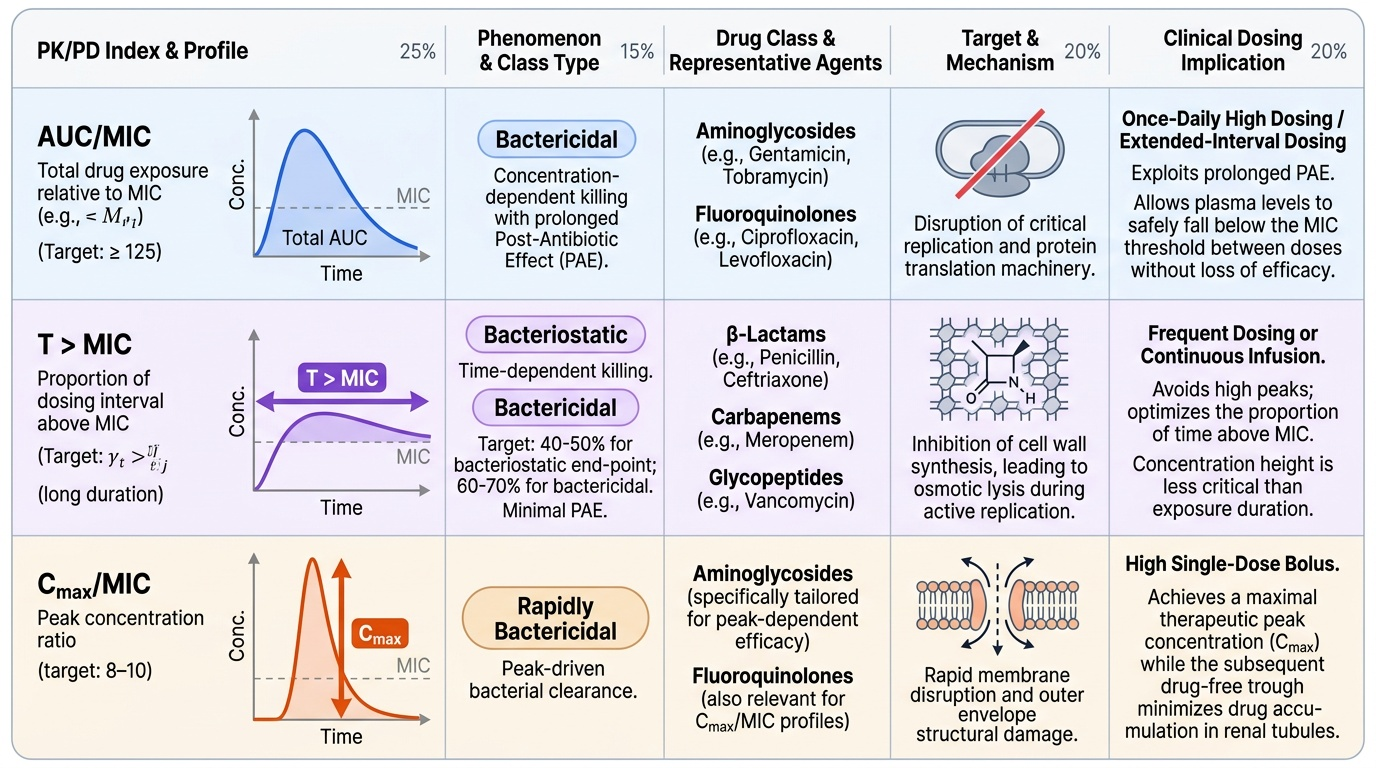
- AUC/MIC (area under curve / minimum inhibitory concentration): the total drug exposure over time relative to the concentration required to inhibit the organism. The target for aminoglycosides against gram-negatives is AUC/MIC >125. Fluoroquinolones also exhibit concentration-dependent killing with an AUC/MIC target of >30–125 depending on the pathogen. These are concentration-dependent killers with a prolonged post-antibiotic effect (PAE) — growth suppression persists after drug levels fall below MIC — permitting once-daily dosing.
- T>MIC (time above MIC): the proportion of the dosing interval during which the free drug concentration exceeds the MIC. β-Lactams are the archetype of time-dependent killers: efficacy correlates with the percentage of the dosing interval that free drug remains above MIC (target: 40–50% for bacteriostatic endpoint; >60–70% for bactericidal). This is why β-lactams are dosed frequently or via continuous infusion rather than high single doses; their PAE is minimal for most gram-negatives.
- Cmax/MIC (peak concentration/MIC): relevant for aminoglycosides and fluoroquinolones; Cmax/MIC >8–10 for aminoglycosides. This underpins extended-interval (once-daily) aminoglycoside dosing — giving the total daily dose as a single bolus achieves a high peak, maximising bactericidal activity, while the drug-free trough allows renal tubular recovery (reducing nephrotoxicity).
Understanding these indices allows a prescriber to reason about dose optimisation without simply escalating dose.
Provided image
| PK/PD Index | Killing Pattern | Drug Class Examples | Clinical Dosing Implication |
|---|---|---|---|
| AUC/MIC | Concentration-dependent | Aminoglycosides, fluoroquinolones | Once-daily or high-dose intervals; exploit PAE |
| T>MIC | Time-dependent | β-Lactams, carbapenems, vancomycin | Frequent dosing or continuous infusion |
| Cmax/MIC | Concentration-dependent | Aminoglycosides (peak) | High single-dose strategy to maximise Cmax |
Spectrum of activity is the range of organisms a drug covers. Broad-spectrum agents (carbapenems, fluoroquinolones, third-generation cephalosporins) cover gram-positives, gram-negatives, and sometimes anaerobes — invaluable empirically but powerful drivers of resistance. Narrow-spectrum agents (penicillin G, metronidazole, clindamycin) are preferred when the pathogen is known, reducing collateral pressure on the microbiome and resistance ecology. The principle of rational prescribing: use the narrowest effective spectrum once the pathogen is identified (de-escalation).
SELF-CHECK
A patient with Pseudomonas pneumonia is prescribed tobramycin. The prescriber wants to maximise bactericidal killing while minimising nephrotoxicity. Which PK/PD dosing strategy is most appropriate?
A. Multiple small doses throughout the day to maintain T>MIC
B. A single high daily dose to maximise Cmax/MIC and allow drug-free trough
C. Continuous IV infusion to keep AUC/MIC constant
D. Oral dosing twice daily to reduce renal exposure
Reveal Answer
Answer: B. A single high daily dose to maximise Cmax/MIC and allow drug-free trough
Aminoglycosides exhibit concentration-dependent killing; efficacy correlates with Cmax/MIC and AUC/MIC. Extended-interval (once-daily) dosing achieves a high Cmax that maximises bactericidal activity, while the drug-free trough period allows renal tubular cell recovery, reducing accumulation and nephrotoxicity. Continuous infusion and frequent small doses fail to generate the high peak needed for concentration-dependent killing.
Understanding Antimicrobial Resistance
Antimicrobial resistance (AMR) is the ability of a microorganism to survive and replicate in the presence of a drug that would normally kill or inhibit it. Resistance is either intrinsic (natural, predictable — e.g. aerobic organisms are intrinsically resistant to metronidazole; gram-negative outer membrane limits vancomycin entry) or acquired (developed during or after antibiotic exposure).
Acquired resistance arises through two fundamental mechanisms:
1. Spontaneous mutation: errors in DNA replication generate mutant strains. In large bacterial populations, a mutant with reduced drug susceptibility may be present before treatment begins — antibiotic exposure then provides selective pressure, allowing the resistant mutant to dominate. This is the basis of resistance to rifampicin (single-step mutation in rpoB) and fluoroquinolones (mutations in gyrA/parC). Never use rifampicin as monotherapy (resistance emerges rapidly).
2. Horizontal gene transfer (HGT): transfer of resistance genes between bacteria via:
- Plasmids (extrachromosomal DNA): the most clinically important route. Plasmids carrying resistance genes (e.g. blaNDM encoding New Delhi Metallo-β-lactamase) spread within and between species. ESBL (extended-spectrum β-lactamase) genes on plasmids explain the epidemic of ceftriaxone-resistant E. coli and Klebsiella.
- Transposons ('jumping genes'): mobile elements that move resistance genes between plasmids and chromosomes.
- Integrons: capture and express gene cassettes encoding resistance enzymes.
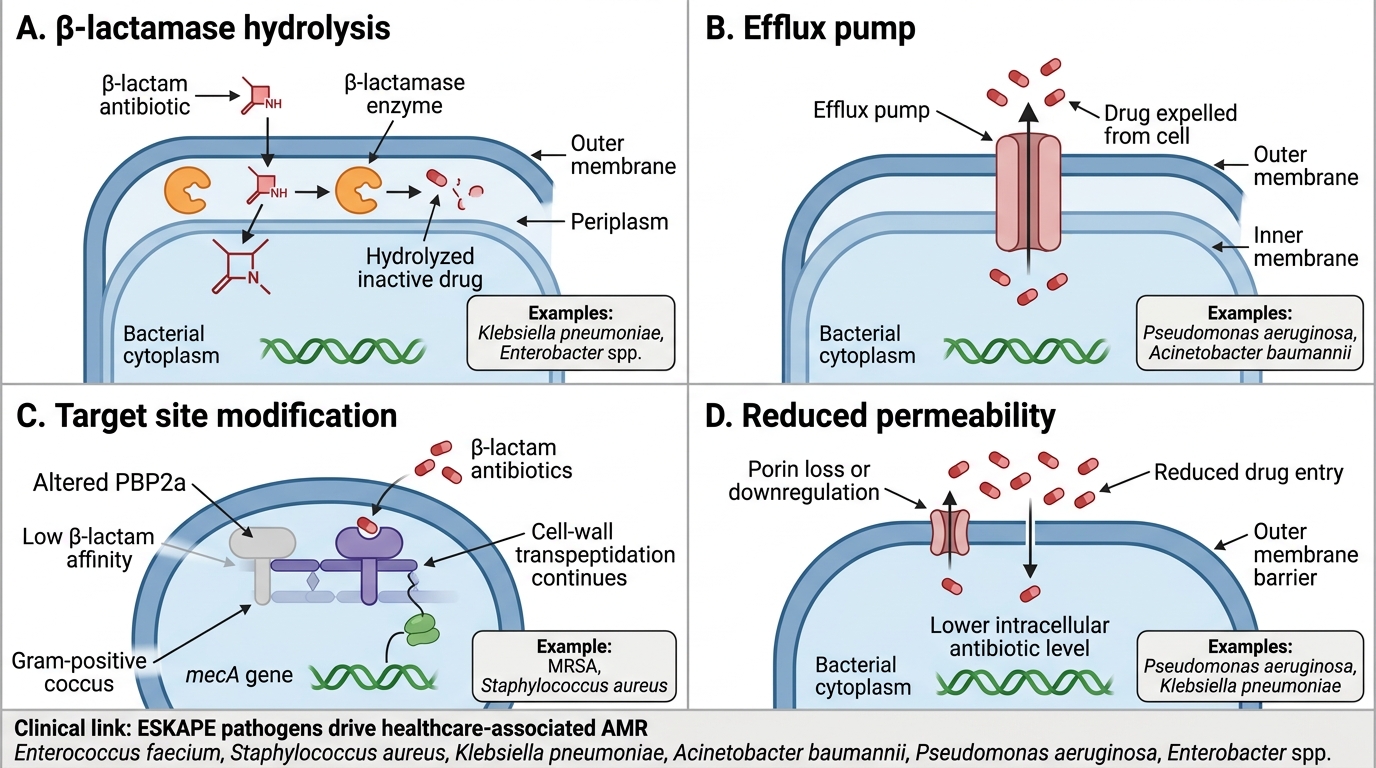
The four principal mechanisms of resistance at the molecular level are:
1. Enzymatic inactivation: β-lactamases hydrolyse the β-lactam ring (most important resistance mechanism globally); aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases).
2. Efflux pumps: active transporters that pump antibiotics out of the cell (e.g. mex pumps in Pseudomonas aeruginosa confer resistance to multiple classes including fluoroquinolones and β-lactams).
3. Target site modification: alteration of the drug binding site — e.g. altered PBPs (penicillin-binding proteins) in MRSA (methicillin-resistant Staphylococcus aureus) confer β-lactam resistance; methylation of the 23S rRNA confers macrolide resistance (MLSB phenotype).
4. Reduced permeability: loss of outer-membrane porins in gram-negatives reduces drug entry (e.g. OprD porin loss in carbapenem-resistant Pseudomonas).
Mechanisms of Antimicrobial Resistance
Clinical implications: ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, Enterobacter spp.) are the WHO priority organisms driving AMR-related mortality. Understanding their resistance mechanisms is essential for empiric choice in healthcare-associated infections.
SELF-CHECK
Which of the following resistance mechanisms allows MRSA to resist all beta-lactam antibiotics including carbapenems?
A. Production of extended-spectrum β-lactamase (ESBL)
B. Efflux pump upregulation expelling all β-lactams
C. Acquisition of an altered penicillin-binding protein (PBP2a) with low β-lactam affinity
D. Loss of outer-membrane porins reducing drug entry
Reveal Answer
Answer: C. Acquisition of an altered penicillin-binding protein (PBP2a) with low β-lactam affinity
MRSA carries the mecA gene (on mobile genetic element SCCmec), encoding PBP2a — a transpeptidase with very low affinity for all β-lactam antibiotics. Normal β-lactams bind and inhibit PBPs, blocking cell-wall synthesis and causing lysis; PBP2a can still carry out transpeptidation when normal PBPs are inhibited, conferring class-wide resistance. ESBLs are seen in gram-negative organisms. Efflux pumps and porin loss are gram-negative mechanisms and do not confer resistance to all β-lactams in the same way.