Page 2 of 46
PH8.1-2 | PH8.1-2 | Antimicrobial Principles and Stewardship — SDL Guide — SDL Guide (Part 2)
How to Choose and Use Antimicrobials Rationally
Rational antimicrobial use is a systematic decision process, not a recipe. The prescriber works through four questions in order — and each answer narrows the choice:
Step 1: Is an antibiotic needed at all? Many febrile illnesses (viral upper respiratory tract infections, dengue, simple viral gastroenteritis) do not benefit from antibiotics. Prescribing antibiotics for viral infections is among the leading drivers of community resistance. The prescriber must resist patient pressure to prescribe.
Step 2: Identify the likely pathogen(s) and site of infection. Clinical syndrome guides empiric choice before cultures are available: community-acquired pneumonia (Streptococcus pneumoniae, atypicals); urinary tract infection (E. coli predominant, but local resistance patterns matter); meningitis (Neisseria meningitidis, S. pneumoniae in adults; Listeria in immunocompromised/elderly). Collect appropriate cultures BEFORE starting antibiotics whenever possible — this is the foundation of culture-guided therapy.
Step 3: Assess host factors that modify drug choice and dose:
- Allergy: penicillin allergy (true IgE-mediated allergy ~1–5% of claimed; careful history avoids unnecessary broad-spectrum substitution)
- Renal/hepatic function: aminoglycosides, vancomycin, carbapenems require renal dose adjustment; hepatically cleared drugs (metronidazole, rifampicin) require caution in liver disease
- Pregnancy: avoid tetracyclines (fetal bone/teeth), aminoglycosides (fetal VIII nerve), fluoroquinolones (fetal cartilage), TMP/sulfonamides near term (kernicterus risk)
- Immunosuppression: broader empiric cover; consider fungal co-infection
- Local resistance data (antibiogram): the hospital's antibiogram is an essential prescribing tool, particularly for gram-negatives
Step 4: De-escalation. Once culture and sensitivity results return (typically 48–72 hours), switch from broad empiric to the narrowest agent that covers the confirmed pathogen. De-escalation: (a) reduces selection pressure for resistance; (b) reduces adverse effects (e.g. Clostridioides difficile risk with broad-spectrum agents); (c) reduces cost. Evidence from ICU studies shows de-escalation does not increase mortality when done appropriately.
Duration of therapy matters as much as drug choice. Unnecessarily long courses drive resistance and increase adverse events. Evidence-based durations: uncomplicated UTI (nitrofurantoin/TMP-SMX) = 3–5 days; community-acquired pneumonia = 5 days; skin and soft tissue = 5–7 days; osteomyelitis (historically 6 weeks; emerging evidence supports shorter IV courses).
Antibiotic Stewardship in Practice
An Antibiotic Stewardship Programme (ASP) is a coordinated, institution-wide set of interventions designed to improve antibiotic use — selecting the right drug, dose, route, and duration — to improve patient outcomes while reducing resistance, adverse effects, and costs. The WHO, IDSA, and Indian guidelines (MoHFW) all mandate ASPs in tertiary hospitals.
The core components of an ASP at a teaching hospital like yours are:
1. Formulary restriction and prior authorisation. Certain high-risk or broad-spectrum antibiotics (carbapenems, colistin, cefoperazone-sulbactam) require approval from an ID specialist or microbiologist before dispensing. This reduces unnecessary broad-spectrum use and creates an educational touchpoint.
2. Prospective audit and feedback. A pharmacist or ID-trained physician reviews antibiotic orders after 48–72 hours (when culture data arrives) and provides real-time feedback to prescribers about de-escalation opportunities, dose optimisation, or unnecessary treatment.
3. IV-to-oral (IV→PO) switch. When a patient is clinically improving, afebrile, and able to take oral medication, switching from IV to oral antibiotics of equivalent bioavailability (e.g. IV amoxicillin → oral amoxicillin; IV levofloxacin → oral levofloxacin) is equally effective for many infections while reducing hospital stay, IV line complications, and cost.
4. PK/PD-guided dosing. For critically ill patients with augmented renal clearance (increased drug elimination), standard doses may be subtherapeutic. For patients with renal impairment, standard doses may be toxic. Therapeutic drug monitoring (TDM) — measuring trough/peak vancomycin or aminoglycoside levels — guides dose adjustment.
5. Education and guidelines. Regular sessions for prescribers, updated local antibiotic guidelines reflecting current resistance patterns, clinical decision support tools (computer alerts for double anaerobic cover, redundant β-lactam combinations).
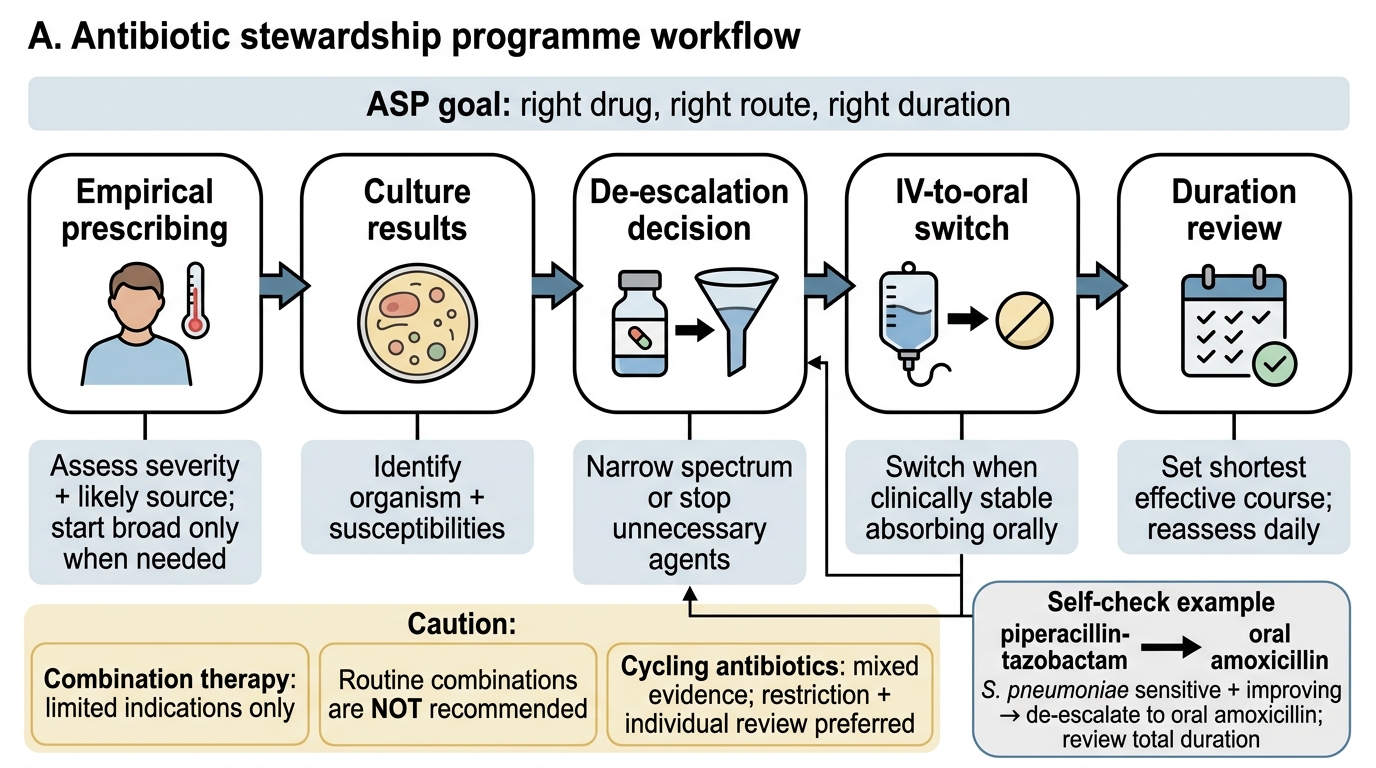
Antibiotic Stewardship Workflow
Combination therapy is used in specific situations: (a) to broaden empiric cover pending cultures in critically ill patients (not a stewardship goal, but a safety necessity); (b) to achieve synergism (e.g. β-lactam + aminoglycoside for enterococcal endocarditis); (c) to prevent resistance emergence (e.g. rifampicin must never be used as monotherapy — combination partner prevents rapid single-step resistance). Routine combination therapy for common infections is NOT recommended and does not prevent resistance.
Antimicrobial cycling (rotating formulary antibiotics in a unit on a schedule) was proposed to reduce resistance but evidence from clinical trials is mixed — cycling may actually accelerate exposure to each class. Most ASPs now prefer restriction-based and individualised approaches over cycling.
SELF-CHECK
A patient with healthcare-associated pneumonia is on day 3 of piperacillin-tazobactam. Sputum culture returns Streptococcus pneumoniae fully sensitive to amoxicillin. She is afebrile and clinically improving. What is the most appropriate ASP-guided action?
A. Continue piperacillin-tazobactam for the full 7-day course since it covers the pathogen
B. Switch to IV amoxicillin since oral is less effective for pneumonia
C. De-escalate to oral amoxicillin with a total 5-day course from clinical improvement
D. Add vancomycin coverage for possible MRSA co-infection
Reveal Answer
Answer: C. De-escalate to oral amoxicillin with a total 5-day course from clinical improvement
De-escalation is the core ASP action: once a pathogen is identified and the patient is improving, switch to the narrowest effective agent. S. pneumoniae sensitive to amoxicillin should be treated with amoxicillin, not broad-spectrum piperacillin-tazobactam. Amoxicillin has excellent oral bioavailability (~90%), making IV-to-oral switch appropriate in a clinically stable patient. The total course from clinical improvement should be 5 days for CAP (evidence-based). Adding vancomycin without MRSA indication is the opposite of stewardship.
Evaluating Stewardship Outcomes
Measuring the success of an ASP requires prospective tracking of both process metrics (what prescribers do) and outcome metrics (what happens to patients and the hospital ecosystem). A critical appraisal framework helps you distinguish effective ASP components from well-intentioned but evidence-poor interventions.
Key process metrics:
- Days of therapy (DOT) per 1,000 patient-days: measures antibiotic consumption; a falling DOT is the standard marker of ASP success. More informative than defined daily doses (DDD) because it adjusts for actual patient exposure.
- Adherence to empiric guidelines: percentage of prescriptions matching the hospital's approved empiric guidelines for each syndrome.
- IV-to-oral switch rate: proportion of eligible patients switched within 48–72 hours.
- Time to appropriate therapy: critical in sepsis — every hour of delay in appropriate antibiotics increases mortality; ASPs must balance de-escalation goals with rapid initiation.
Key outcome metrics:
- Clostridioides difficile infection (CDI) rate: CDI is the most sensitive marker of antibiotic overuse. Broad-spectrum antibiotics (especially clindamycin, fluoroquinolones, broad-spectrum cephalosporins) disrupt the gut microbiome and allow C. difficile spore germination. ASPs consistently reduce CDI rates by 30–50%.
- MDRO (multidrug-resistant organism) incidence: tracking MRSA, ESBL-producing organisms, and carbapenem-resistant organisms (CRE, CRAB) over time.
- Antibiotic expenditure: ASPs reliably reduce costs by 10–30%.
- Mortality and length of stay: primary patient safety metrics; well-designed ASPs do not increase mortality.
Critical appraisal of the evidence: Most stewardship trials are quasi-experimental (before-after designs) with risk of confounding — reductions in resistance may reflect infection-control interventions co-occurring with ASP. The strongest evidence supports: (a) prospective audit-and-feedback, (b) formulary restriction for carbapenems and colistin, and (c) IV-to-oral switch programmes. Weaker evidence exists for cycling and combination therapy as resistance-prevention strategies.
Limitations and the prescriber's role: ASPs require infrastructure (microbiology lab turnaround, electronic health records, ID specialists) often unavailable in resource-limited settings. In the absence of formal ASP, the individual prescriber can still apply core principles: culture before treatment, narrowest effective spectrum, shortest effective duration, and resistance surveillance at the local level.