Page 32 of 46
PH8.10 | PH8.10 | Antiviral Drugs Including HIV Therapy — SDL Guide — SDL Guide
Learning Objectives
- Discuss the types, kinetics, dynamics, adverse effects, indications, and contraindications of drugs used for viral diseases including HIV
- Explain the mechanism of selective toxicity in aciclovir, oseltamivir, and major antiretroviral classes
- Describe first-line ART for HIV as per Indian national guidelines and key drug interactions
- Apply antiviral pharmacology to clinical scenarios involving herpetic infections, influenza, and HIV management
INSTRUCTIONS
Antiviral pharmacology has undergone a revolution in the past three decades — from the first antiretroviral (AZT, 1987) to the modern era of one-pill once-daily HIV suppression and the cure of hepatitis C with direct-acting antivirals. India carries a significant burden of viral disease: HIV (~2.3 million people on ART under NACO), chronic HBV (~40 million), and HCV (~6 million). Understanding how antiviral drugs exploit viral-specific machinery — while sparing human cells — is fundamental to safe and effective prescribing.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 61–62 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 62–63 (textbook)
- NACO National Guidelines for HIV Care and Treatment, India 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman presents at 8 weeks of pregnancy with a new HIV diagnosis (CD4 count 320 cells/μL, viral load 85,000 copies/mL). She is terrified — she does not want her baby to be infected. She has been told she will need to take medicines 'for life.' She asks: 'Will the medicines harm my baby? And how does HIV even work — what are these drugs actually doing?' You need to explain HIV pharmacotherapy in a way that makes the regimen comprehensible and the commitment to adherence psychologically achievable. The pharmacological answers — how viral reverse transcriptase, integrase, and protease work; why combination therapy is necessary; why the viral load can reach zero — will not just inform your clinical decision but will build the patient's trust and adherence.
WHY THIS MATTERS
India is home to 2.3 million people living with HIV — the third-largest epidemic globally. The scale-up of ART through the NACO free treatment programme has saved millions of lives. Understanding HIV pharmacology is essential not only for infectious disease but for all specialists — HIV-positive patients present to every department. HCV direct-acting antivirals have achieved cure rates >95% — one of the most dramatic pharmacological success stories in medicine. Herpesvirus infections (HSV, VZV, CMV) are ubiquitous in both immunocompetent and immunocompromised patients. The pharmacological principles in this SDL — selective toxicity exploiting viral enzymes, resistance prevention through combination therapy, and the management of drug interactions — are directly clinically applicable.
RECALL
From general pharmacology (PH1): prodrug activation — drugs requiring conversion to active form for effect; nucleoside analogues — structural mimics of natural nucleosides that compete with them as enzyme substrates. From the antibacterials SDL: resistance prevention by combination therapy — using multiple drugs simultaneously prevents the selection of single-gene resistant mutants; the same principle applies to HIV. From the TB SDL: rifampicin as CYP3A4 inducer — reduces levels of most HIV PIs by >90% and NNRTIs substantially — the most clinically important drug interaction in HIV-TB co-treatment.
Viral Replication Pathophysiology: Why Antiviral Drug Targets Are Limited
Viruses are the most pharmacologically challenging pathogens because they are obligate intracellular parasites that co-opt the host cell's own machinery for replication. The challenge of selective antiviral toxicity is that viral replication occurs inside human cells, using many of the same enzymes, ribosomes, and metabolic pathways as the host cell. Unlike bacteria (prokaryotes with distinctive 70S ribosomes, cell walls, and metabolic pathways), viruses use human 80S ribosomes, human DNA polymerase (for DNA viruses in the late replication phase), and human metabolic pathways for ATP generation.
The exploitable differences between viral and host machinery that antiviral drugs target:
1. Virus-specific enzymes: Some viruses encode unique enzymes absent in human cells: viral thymidine kinase (TK) in herpes viruses; reverse transcriptase in retroviruses (HIV, HBV) and lentiviruses — transcribes RNA→DNA, absent in normal human cells; HIV integrase — integrates viral cDNA into the host chromosome; HIV protease — cleaves viral polyprotein precursors (human cysteine/serine proteases are structurally different and less susceptible to HIV protease inhibitors); influenza neuraminidase — cleaves sialic acid (human neuraminidase is structurally different).
2. Viral structural proteins: Envelope glycoproteins (used in entry inhibitors); viral capsid assembly processes.
3. Viral-specific nucleic acid synthesis: Some viral DNA polymerases (herpesvirus) or RNA-dependent RNA polymerases (influenza, HCV) have structural differences from human polymerases that allow selective inhibitors.
HIV lifecycle — the master model for antiretroviral targets: HIV is a lentivirus (retrovirus) with a lifecycle that involves: (1) CD4 receptor + CCR5/CXCR4 co-receptor binding (target: entry/fusion inhibitors); (2) membrane fusion (target: enfuvirtide); (3) reverse transcription of viral RNA → viral DNA by HIV reverse transcriptase (RT) — a RNA-dependent DNA polymerase unique to retroviruses (target: NRTIs, NNRTIs); (4) nuclear transport and integration of viral cDNA into the host chromosome by HIV integrase (target: INSTIs — integrase strand transfer inhibitors); (5) viral gene transcription and translation using host machinery; (6) assembly and budding of viral polyprotein precursors; (7) HIV protease cleavage of polyprotein → structural proteins and enzymes (target: PIs — protease inhibitors). Only then does a mature, infectious virion emerge.
Therapeutic Goal: Stage-Specific Targeting and Viral Suppression
The therapeutic goals of antiviral pharmacotherapy are fundamentally different for different viruses:
For herpes viruses (HSV, VZV, CMV): The goal is suppression of active replication during acute episodes (reducing severity, duration, complications) and prevention of recurrence (suppressive therapy in frequent recurrers). True eradication is not achieved — viruses establish latency in neuronal ganglia (HSV, VZV) or peripheral blood mononuclear cells (CMV) and cannot be eliminated. Selective toxicity in aciclovir is elegantly exploited: aciclovir is activated ONLY by viral thymidine kinase (TK) — host TK has 3000-fold lower affinity for aciclovir. Thus, only herpes virus-infected cells accumulate the active form, concentrating the drug where it is needed.
For influenza: Goal is early treatment (within 48 hours of symptom onset, when viral replication is peaking) to reduce symptom duration by 1–2 days and reduce risk of complications (pneumonia). Neuraminidase inhibitors prevent viral spread from infected cells — they do not kill intracellular virus directly. Hence: the earlier you treat, the more virions are prevented from spreading.
For HIV: The goal is durable viral suppression — reducing viral load to undetectable levels (<50 copies/mL) and maintaining this suppression indefinitely. Because HIV cannot be cured (integrated provirus persists in long-lived CD4 cells), treatment is lifelong. Complete viral suppression: (1) allows CD4 count recovery → immune restoration; (2) prevents AIDS-defining illnesses; (3) prevents HIV transmission (Undetectable = Untransmittable: U=U). Three-drug combination therapy (ART) is standard — not for synergy, but to prevent resistance: HIV replicates at >10⁹ virions/day with error-prone reverse transcriptase (no proofreading) → natural resistance mutations always present. Any one drug would select resistant mutants; three drugs targeting three different enzymes/steps make the probability of simultaneous triple-drug resistance essentially zero.
For HCV (direct-acting antivirals): Goal is virological cure — sustained virological response (SVR12: undetectable HCV RNA at 12 weeks post-treatment = cure in 99%+ of cases). Modern pan-genotypic DAA regimens (glecaprevir+pibrentasvir, sofosbuvir+velpatasvir) achieve SVR >95% with 8–12 weeks of treatment, with minimal adverse effects — a pharmacological miracle compared to the 48-week interferon-ribavirin regimen it replaced.
Classification of Antiviral Drugs
Antiviral drugs are classified by their target virus and mechanism:
Provided image
Anti-herpetic agents (viral TK-dependent activation):
- Aciclovir (acyclovir) — HSV-1, HSV-2, VZV; prodrug activated by viral TK
- Valaciclovir — oral prodrug of aciclovir (L-valyl ester → better bioavailability ~55% vs aciclovir 20%)
- Ganciclovir — CMV; activated by CMV UL97 kinase (not TK); valaciclovir NOT active vs CMV
- Valganciclovir — oral prodrug of ganciclovir (high bioavailability)
- Famciclovir — HSV/VZV; oral prodrug of penciclovir
- Cidofovir — broad-spectrum antiviral, activated by host kinases (not viral TK) — used for CMV retinitis when ganciclovir fails
Anti-influenza agents:
- Oseltamivir (Tamiflu) — neuraminidase inhibitor; influenza A and B; oral
- Zanamivir (Relenza) — neuraminidase inhibitor; inhaled (not oral)
- Baloxavir marboxil — cap-dependent endonuclease inhibitor (different mechanism from NA inhibitors); influenza A and B; single dose
Anti-hepatitis agents:
- Chronic HBV: Tenofovir disoproxil fumarate (TDF) or tenofovir alafenamide (TAF), Entecavir — nucleos(t)ide RT inhibitors; suppress HBV replication but do not eradicate cccDNA (treatment long-term or lifelong). Pegylated interferon-alpha (48-week course, finite duration, higher rate of seroconversion but significant ADRs: flu-like syndrome, depression, cytopaenia).
- Chronic HCV: Direct-acting antivirals (DAAs) — NS3/4A protease inhibitors (glecaprevir, voxilaprevir), NS5A inhibitors (pibrentasvir, velpatasvir), NS5B polymerase inhibitors (sofosbuvir — chain terminator). Pan-genotypic combinations achieve >95% SVR.
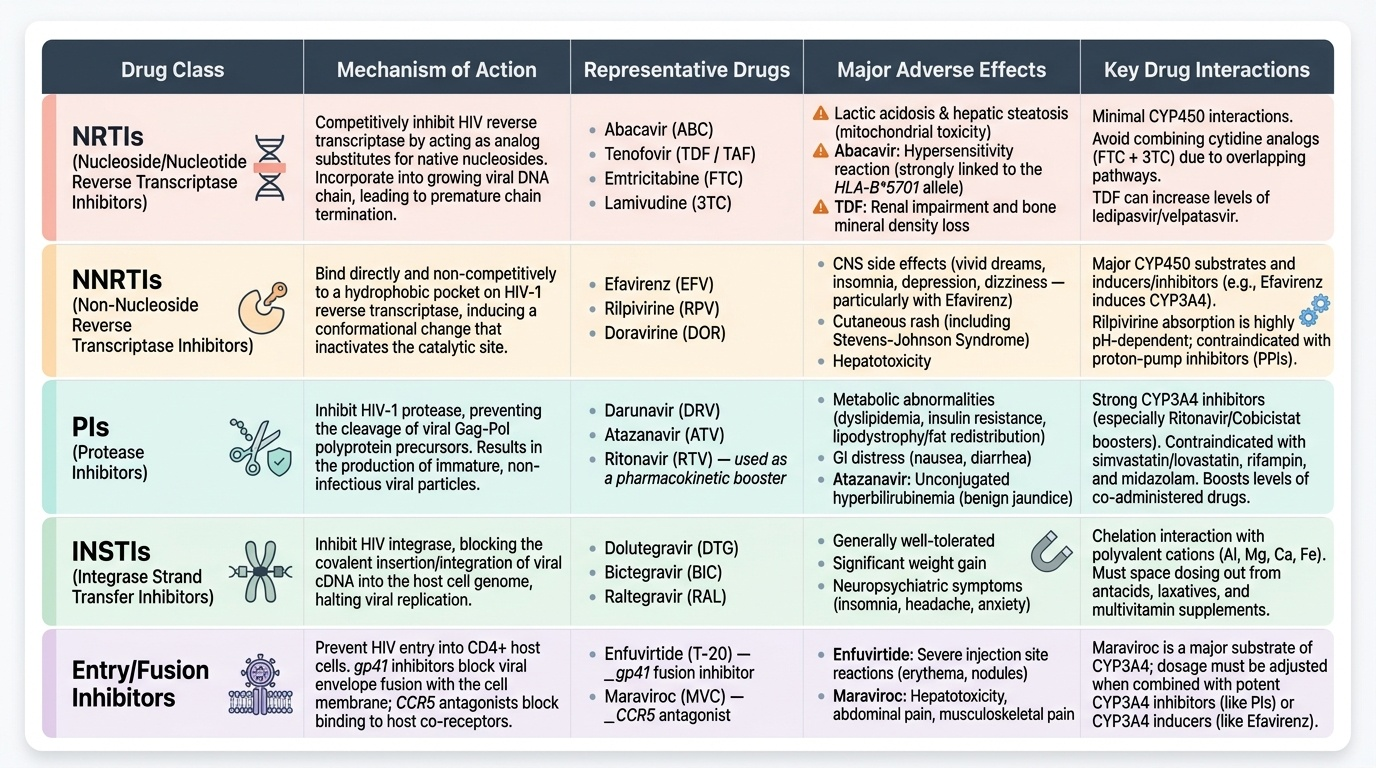
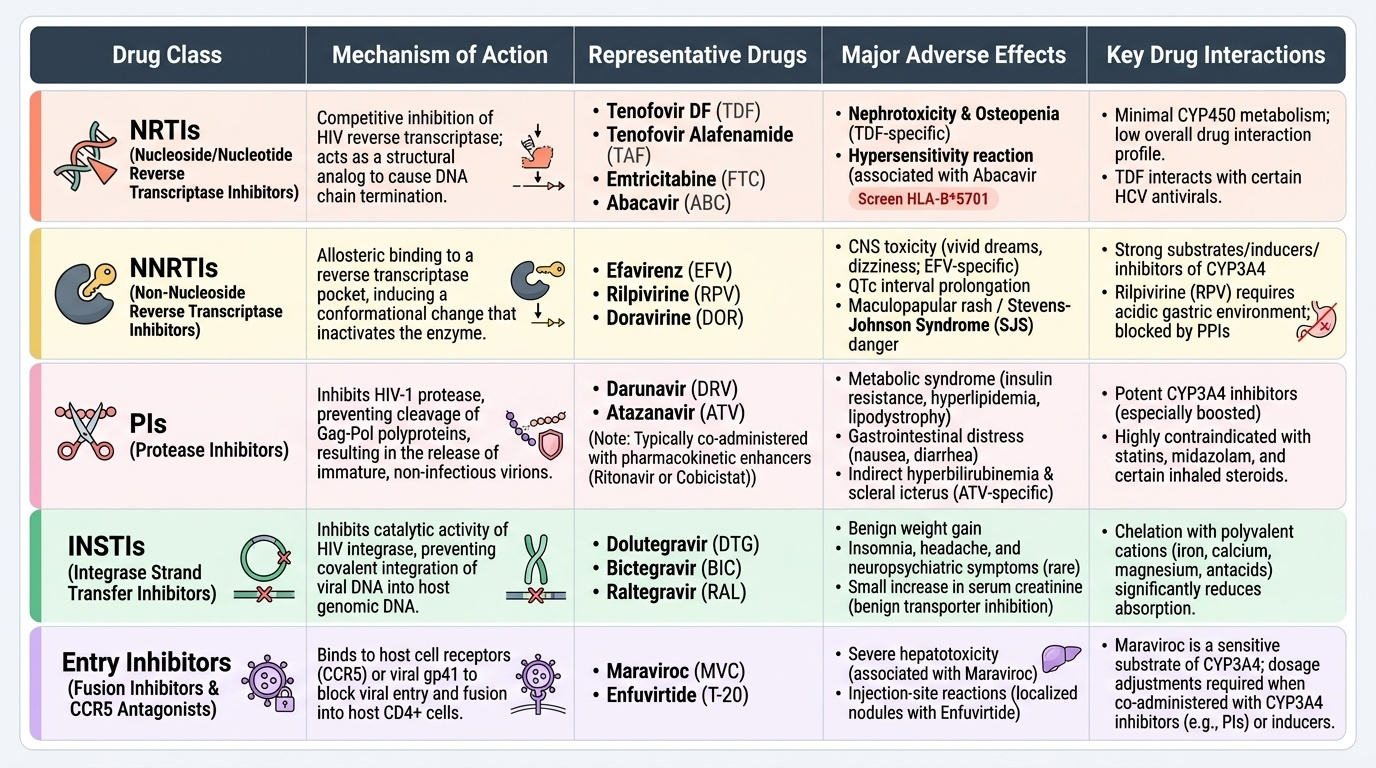
Antiretrovirals for HIV:
- NRTIs, NNRTIs, PIs, INSTIs, entry/fusion inhibitors (see below)
Provided image