Page 33 of 46
PH8.10 | PH8.10 | Antiviral Drugs Including HIV Therapy — SDL Guide — SDL Guide (Part 2)
Anti-Herpetic and Anti-Influenza Drugs
Aciclovir — the selective antiherpetic archetype:
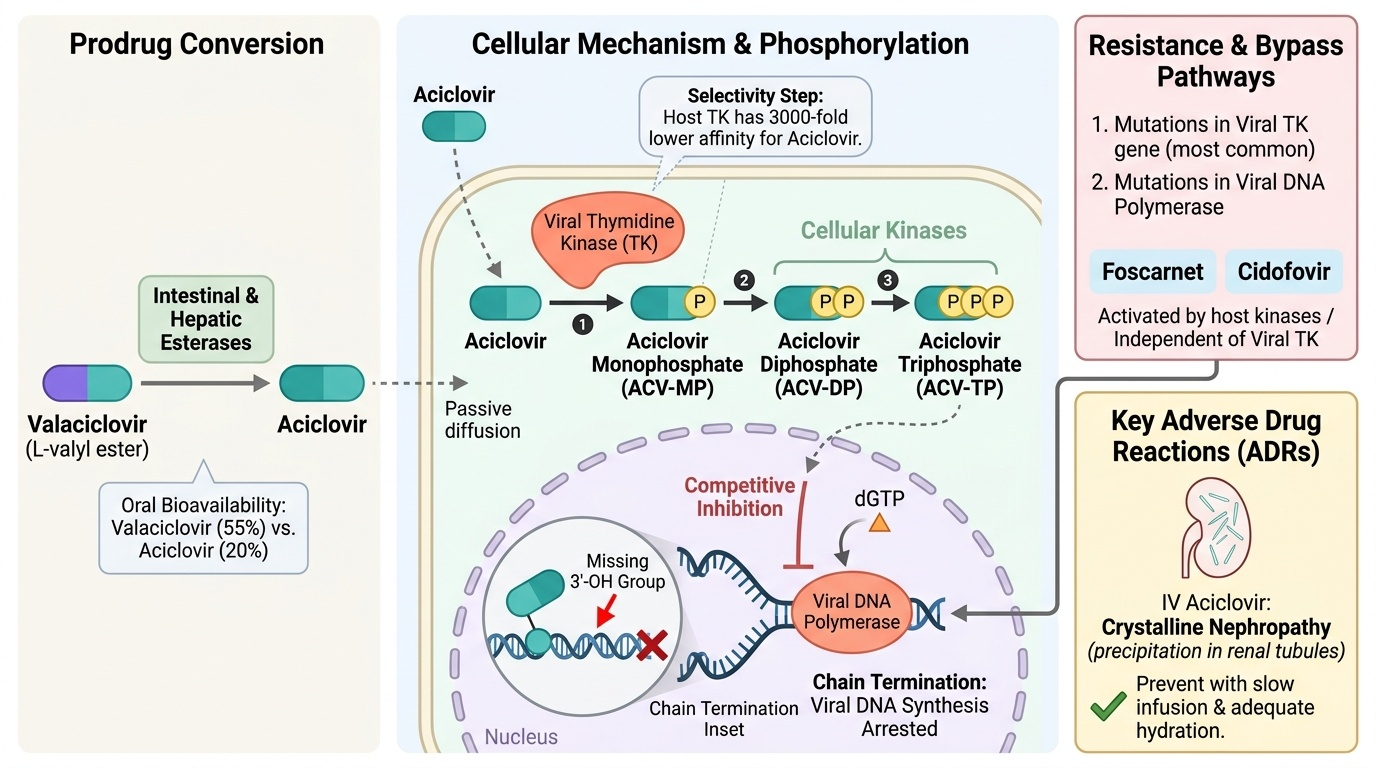
- Mechanism of selectivity: Aciclovir is a synthetic purine nucleoside analogue (guanosine analogue with an acyclic sugar). It is a prodrug activated in a 3-step phosphorylation process:
- Step 1: Viral thymidine kinase (TK) phosphorylates aciclovir → aciclovir monophosphate (ACV-MP). This is the selectivity step — host cell TK has 3000-fold lower affinity for aciclovir vs viral TK; therefore, ACV-MP accumulates almost exclusively in virus-infected cells.
- Steps 2 & 3: Cellular kinases convert ACV-MP → aciclovir diphosphate → aciclovir triphosphate (ACV-TP) (active form).
- ACV-TP acts as a competitive inhibitor of viral DNA polymerase AND as a chain terminator — when incorporated into nascent viral DNA (instead of deoxyGTP), it lacks the 3'-OH group needed for the next phosphodiester bond formation → viral DNA synthesis arrests permanently.
- Spectrum: HSV-1, HSV-2, VZV. Limited activity vs Epstein-Barr virus (EBV — has different TK). NO activity vs CMV — CMV does not encode TK (uses a different kinase, UL97); aciclovir is not efficiently phosphorylated by UL97.
- Clinical uses: HSV encephalitis (IV aciclovir 10mg/kg TDS × 14–21 days — urgent); genital herpes (episodic: 400mg TDS × 5 days; suppressive: 400mg BD daily); herpes labialis (cold sore); herpes zoster/VZV (800mg 5× daily × 7 days); VZV in immunocompromised (IV aciclovir).
- ADRs: IV aciclovir — nephrotoxicity (crystalline nephropathy from aciclovir precipitation in renal tubules — prevent by adequate hydration; infuse slowly over 1 hour; dose adjust for renal impairment). Thrombophlebitis at IV site. CNS toxicity (tremors, confusion) at high doses. Oral aciclovir — well-tolerated; GI.
- Resistance: Mutations in viral TK gene (reduces or abrogates aciclovir activation) — most common; mutations in viral DNA polymerase also occur. Aciclovir-resistant HSV treated with foscarnet or cidofovir (both activated by host kinases, independent of viral TK).
Provided image
Valaciclovir — oral prodrug of aciclovir:
- L-valyl ester of aciclovir; intestinal and hepatic esterases cleave to release aciclovir → bioavailability 55% (vs 20% for aciclovir). Better compliance with fewer daily doses. For genital herpes recurrence suppression: 500mg once daily. For herpes zoster: 1g TDS × 7 days. For VZV — preferred oral agent over aciclovir for adults.
Ganciclovir and valganciclovir — for CMV:
- Mechanism: similar to aciclovir but activated by CMV-encoded phosphotransferase UL97 (not TK) → ganciclovir triphosphate → inhibits CMV DNA polymerase + chain termination. Active vs all herpesviruses but used specifically for CMV because of superior anti-CMV potency.
- Clinical use: CMV retinitis (in AIDS), CMV colitis/pneumonitis (in transplant recipients). Valganciclovir (oral prodrug — 60% bioavailability) is preferred for maintenance therapy.
- ADRs: Myelosuppression (leukopenia, thrombocytopenia, anaemia) — most important; monitor CBC weekly. Nephrotoxicity. Teratogenic and mutagenic — avoid in pregnancy. Males: spermatogenesis suppression → contraception required during and for 90 days after.
Oseltamivir (Tamiflu) — influenza neuraminidase inhibitor:
- Mechanism: competitive inhibitor of influenza neuraminidase (NA) enzyme. NA cleaves sialic acid (neuraminic acid) residues on the surface of infected cells and mucus — allowing newly assembled influenza virions to detach from the infected cell and spread to new cells. Without NA activity, newly formed virions remain stuck to the infected cell surface and to mucus → self-limited viral spread.
- Spectrum: Influenza A (including H1N1 pandemic strains, avian H5N1 when dose-adjusted) and Influenza B. Does NOT cover SARS-CoV-2 (COVID-19 — different enzyme targets).
- Timing: Must be started within 48 hours of symptom onset for meaningful clinical benefit (reduces illness duration by ~1 day, severity, and risk of hospitalisation in at-risk patients). After 48 hours: benefit diminishes but still given for severe influenza requiring hospitalisation or in immunocompromised.
- Dose: 75mg BD × 5 days (treatment); 75mg once daily × 10 days (prophylaxis post-exposure).
- ADRs: nausea/vomiting (take with food); transient neuropsychiatric events reported in children (confusion, self-harm — not definitively drug-related; monitor).
SELF-CHECK
An immunocompromised patient with AIDS (CD4 count 30 cells/μL) develops blurring of vision in the right eye. Ophthalmoscopy reveals CMV retinitis. Which antiviral is most appropriate and why can aciclovir NOT be used?
A. Aciclovir IV — broadest spectrum antiherpetic, covers all herpesviruses including CMV
B. Valganciclovir orally — appropriate first-line; aciclovir cannot be used because CMV lacks viral thymidine kinase to activate it
C. Oseltamivir — effective against CMV retinitis as it targets viral neuraminidase
D. Foscarnet IV — first-line for CMV retinitis; ganciclovir and valganciclovir are too hepatotoxic
Reveal Answer
Answer: B. Valganciclovir orally — appropriate first-line; aciclovir cannot be used because CMV lacks viral thymidine kinase to activate it
Aciclovir cannot be used for CMV because aciclovir's selectivity depends entirely on activation by viral thymidine kinase (TK). CMV does not encode TK — instead, CMV uses a phosphotransferase encoded by the UL97 gene for initial ganciclovir phosphorylation. Ganciclovir (and its oral prodrug valganciclovir) is efficiently phosphorylated by CMV UL97, making it the drug of choice for CMV infections. Valganciclovir 900mg BD × 21 days (induction) followed by 900mg once daily (maintenance) is the standard oral regimen for CMV retinitis. Foscarnet is reserved for ganciclovir-resistant CMV (UL97 or DNA polymerase mutations) or when myelosuppression precludes ganciclovir use. Oseltamivir targets influenza neuraminidase — no anti-CMV activity.
Antiretroviral Therapy: Classes, Mechanisms, and Indian Guidelines
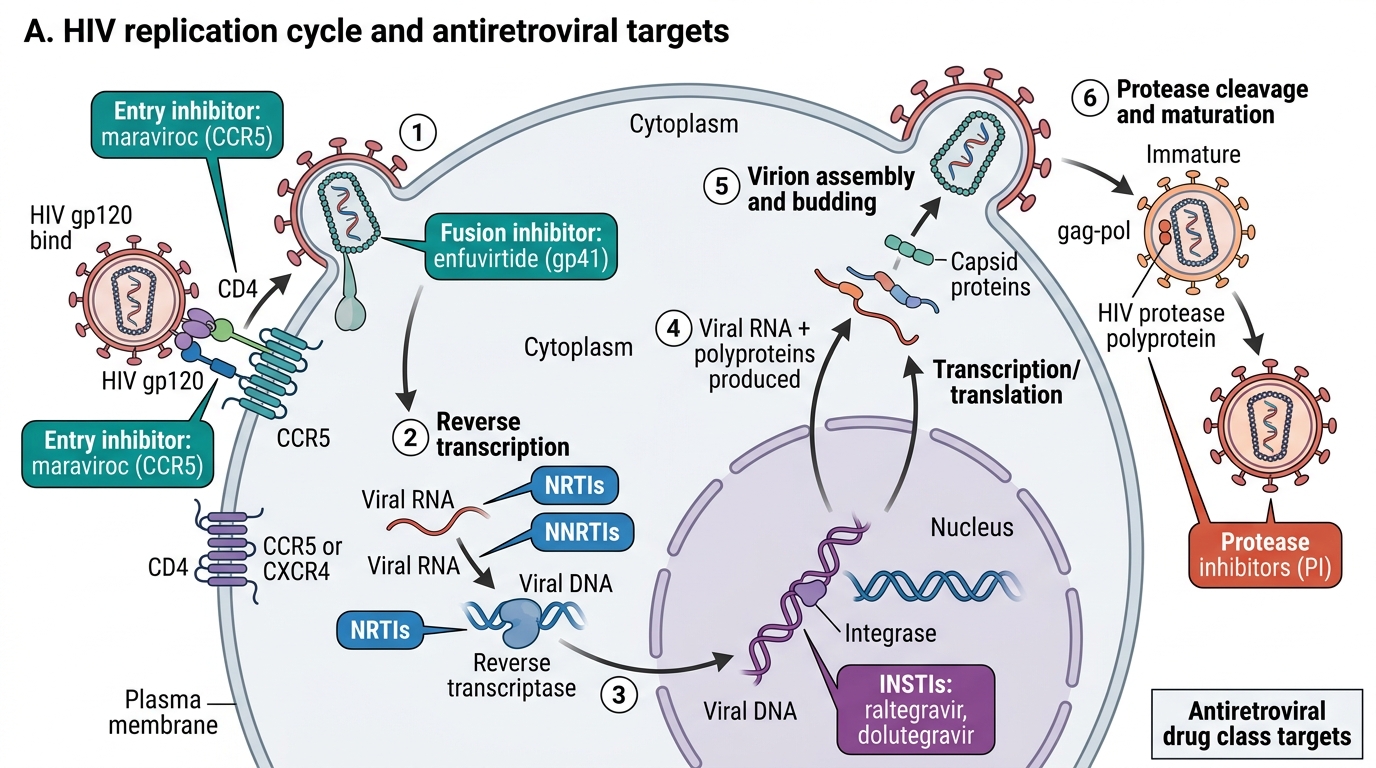
HIV antiretroviral therapy (ART) comprises five drug classes targeting different steps in the HIV lifecycle. Modern first-line regimens combine three drugs (or two drugs in select cases), covering multiple lifecycle stages to maximise viral suppression and prevent resistance emergence.
Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs/NtRTIs):
- Mechanism: analogues of natural nucleosides (adenosine, cytidine, thymidine, guanosine). They are phosphorylated by cellular kinases to their triphosphate forms → competitive inhibitors of viral reverse transcriptase. When incorporated into the growing viral DNA chain, they terminate chain elongation (they lack a 3'-OH group needed for the next nucleotide addition → obligate chain terminator).
- Key drugs: Tenofovir disoproxil fumarate (TDF) — adenosine nucleotide analogue; backbone of modern first-line regimens; active vs HIV AND HBV (both use reverse transcriptase); renal toxicity (Fanconi syndrome — proximal tubular damage; monitor creatinine, phosphate). Tenofovir alafenamide (TAF) — newer prodrug with less renal/bone toxicity, same antiviral activity. Lamivudine (3TC) / Emtricitabine (FTC) — cytidine analogues; excellent tolerability; both active vs HBV; cross-resistance. Abacavir (ABC) — guanosine analogue; hypersensitivity reaction (HLA-B5701-positive patients have 58% risk of severe HSR; screen for HLA-B5701 before starting ABC). Zidovudine (AZT/ZDV) — thymidine analogue; historical first antiretroviral; used in PMTCT (prevention of mother-to-child transmission); bone marrow suppression (anaemia, neutropenia).
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs):
- Mechanism: bind a hydrophobic allosteric pocket in HIV reverse transcriptase near but not at the catalytic site → conformational change → reduced enzyme activity (non-competitive inhibition). They do NOT need intracellular activation (not prodrugs).
- Key drugs: Efavirenz (EFV) — historically most widely used NNRTI globally; once daily (long half-life); CNS adverse effects (vivid dreams, dizziness, depression — especially in first 2–4 weeks; improve over time; avoid in patients with psychiatric history); teratogenic in primates — avoid in first trimester if possible; CYP3A4 inducer — reduces levels of PIs and other co-administered CYP3A4 substrates. Nevirapine (NVP) — older; significant hepatotoxicity risk in women with CD4 >250 and men with CD4 >400 at initiation; hypersensitivity rash (Stevens-Johnson syndrome rare but serious). Rilpivirine — newer; fewer CNS effects; NOT for VL >100,000 copies/mL (lower genetic barrier than dolutegravir). NNRTI resistance: single-point mutation in the allosteric pocket can cause high-level resistance to all NNRTIs (low genetic barrier).
Protease Inhibitors (PIs):
- Mechanism: competitively inhibit HIV aspartyl protease — an enzyme that cleaves the viral polyprotein precursor (gag-pol polyprotein) into individual structural proteins (MA, CA, NC) and enzymes (PR, RT, IN) during virion maturation. Without protease cleavage → immature, non-infectious viral particles formed and released but unable to infect new cells.
- Key drugs: Lopinavir/ritonavir (LPV/r) — lopinavir boosted by low-dose ritonavir (pharmacokinetic booster — ritonavir inhibits CYP3A4 → dramatically raises lopinavir levels); Darunavir/ritonavir (DRV/r) — higher genetic barrier, fewer metabolic side effects. PIs are potent CYP3A4 inhibitors → raise levels of statins, rifampicin (rifampicin reduces PI levels >90% — do NOT use rifampicin with most PIs; use rifabutin instead). Metabolic ADRs: dyslipidaemia (high triglycerides/LDL), insulin resistance, lipodystrophy (subcutaneous fat redistribution).
Integrase Strand Transfer Inhibitors (INSTIs):
- Mechanism: HIV integrase catalyses two steps: (1) 3'-processing (cleaves 2 nucleotides from each end of viral cDNA); (2) strand transfer (inserts processed viral cDNA ends into host chromosomal DNA). INSTIs specifically inhibit the strand transfer step → viral DNA cannot be integrated → no permanent infection established.
- Key drugs: Raltegravir (RAL) — first approved INSTI; twice daily. Elvitegravir (boosted). Dolutegravir (DTG) — preferred first-line globally (WHO 2019 and NACO 2021); once daily; high genetic barrier to resistance (single mutations in integrase do not confer resistance — requires multiple mutations); minimal CYP3A4 interactions (minor substrate, not inducer/inhibitor). Well-tolerated; minimal long-term metabolic effects. Bictegravir (BIC) — newest INSTI; similar to DTG. INSTI ADRs: generally excellent tolerability; weight gain reported with DTG (metabolic monitoring recommended); neuropsychiatric effects (rare, insomnia, depression).
Entry/Fusion Inhibitors:
- Maraviroc (CCR5 antagonist): blocks CCR5 co-receptor → HIV cannot bind to CCR5-tropic strains. Requires tropism testing first (only 50–60% of untreated HIV patients have pure CCR5-tropic virus — CXCR4-tropic or dual-tropic virus are not inhibited by maraviroc). Reserved for salvage therapy in treatment-experienced patients.
- Enfuvirtide (T-20, Fuzeon): peptide that binds gp41 (HIV envelope protein) → prevents membrane fusion. Subcutaneous injection twice daily — very poor adherence; only for salvage therapy.
Indian first-line ART (NACO 2021 guidelines):
- Preferred: TDF 300mg + 3TC 300mg + DTG 50mg (Tenofovir + Lamivudine + Dolutegravir) — once daily FDC tablet (TLD); available free at NACO ART centres.
- Alternative (if DTG unavailable or contraindicated): TDF + 3TC + EFV (600mg).
- For TB-HIV co-treatment: TDF + 3TC + EFV 600mg (EFV dose unchanged with rifampicin); OR if DTG used with rifampicin — double dose DTG to 50mg twice daily (rifampicin induces DTG metabolism).
HIV Replication Cycle and Antiretroviral Drug Targets
SELF-CHECK
A newly diagnosed HIV-positive patient has a CD4 count of 350 cells/μL and a viral load of 50,000 copies/mL. He is also being treated for pulmonary TB with rifampicin-containing ATT. Which ART regimen is most appropriate?
A. Lopinavir/ritonavir + tenofovir + lamivudine — PIs are most powerful for high viral load
B. Tenofovir + lamivudine + efavirenz 600mg — efavirenz levels are maintained despite rifampicin due to dose compensation
C. Tenofovir + lamivudine + dolutegravir 50mg once daily — standard first-line and rifampicin has no interaction with DTG
D. Delay ART until TB treatment completed — rifampicin makes all ART combinations unsafe
Reveal Answer
Answer: B. Tenofovir + lamivudine + efavirenz 600mg — efavirenz levels are maintained despite rifampicin due to dose compensation
Rifampicin is a potent CYP3A4/PXR inducer that dramatically reduces levels of PIs (>90% reduction for lopinavir → therapeutic failure — lopinavir/r should NOT be used with rifampicin) and reduces NNRTI levels. Efavirenz (NNRTI) has some CYP induction itself and its levels are maintained (or only modestly reduced) at 600mg/day despite rifampicin — this is why TDF+3TC+EFV at standard doses remains appropriate for HIV-TB co-treatment. Dolutegravir is a substrate of CYP3A4 but its levels are reduced ~57% by rifampicin — to compensate, DTG must be dosed 50mg TWICE DAILY (not once daily) if used with rifampicin. Delaying ART is strongly contraindicated — early ART (within 2–8 weeks of TB treatment initiation) reduces AIDS-related mortality significantly.
Clinical Decision-Making in Antiviral Therapy
Several clinical decision points require integrating antiviral pharmacology with broader clinical context:
When to start ART: WHO 2023 guidelines: start ART at any CD4 count, at any stage of disease, and as soon as possible (ideally same-day). Earlier ART = faster viral suppression = slower CD4 decline = reduced AIDS morbidity = eliminated transmission risk. There is NO CD4 threshold below which to withhold ART. One exception: patients with active TB meningitis — start ART 4–8 weeks after starting TB therapy (early ART in TB meningitis may worsen intracranial pressure via IRIS and worsen outcomes per the SAPiT/ACTG 5221 trials for extrapulmonary TB).
IRIS (Immune Reconstitution Inflammatory Syndrome): When ART rapidly improves immune function (rising CD4), the restored immune system mounts an inflammatory response against pre-existing occult opportunistic infections (TB, CMV, cryptococcal) → paradoxical worsening of opportunistic infection signs (fever recurrence, enlarged lymph nodes, worsening infiltrates). Most common with very low pre-ART CD4. Management: continue ART (do NOT stop unless life-threatening); corticosteroids (prednisolone 1–1.5mg/kg × 2–4 weeks) for paradoxical TB-IRIS with severe features.
Prevention of Mother-to-Child Transmission (PMTCT): Every pregnant HIV-positive woman must receive ART — lifelong ART (WHO Option B+). Current preferred regimen in pregnancy: TDF + 3TC + DTG (dolutegravir — WHO reversed the original neural tube defect caution after larger data showed the absolute risk is low: ~0.05%, lower than the risk of untreated HIV to both mother and child). Neonate receives oral NVP or AZT for 6 weeks. With optimal PMTCT, the mother-to-child transmission rate falls to <2%.
Post-Exposure Prophylaxis (PEP): After occupational HIV exposure (needlestick, mucous membrane — with HIV-positive source): start ART within 72 hours (ideally within 1–2 hours; effectiveness falls substantially after 72h). Regimen: TDF + FTC + DTG × 28 days. Monthly HIV tests for 3 months.
Pre-Exposure Prophylaxis (PrEP): Daily TDF + FTC in HIV-negative individuals at high risk → >90% reduction in HIV acquisition. Requires baseline HIV negative test, 3-monthly HIV testing, and STI screening.
HCV Direct-Acting Antivirals (DAAs): Sofosbuvir + velpatasvir (pan-genotypic) × 12 weeks — cure rate >95% across all 6 HCV genotypes. Minimal drug interactions (unlike older interferon regimens). Key interaction: sofosbuvir + NS5A inhibitors — avoid with rifampicin (CYP induction reduces DAA levels → treatment failure). Rifabutin is safer than rifampicin if TB-HCV co-treatment is needed.
Monitoring ART efficacy: Viral load at 3 and 6 months, then 6-monthly once suppressed. Target: viral load <50 copies/mL (undetectable) by 6 months. CD4 count monitoring: less important once virologically suppressed (viral load is the primary treatment monitoring tool). Drug resistance testing: recommended at treatment failure (VL >1000 copies/mL on ART).
SELF-CHECK
A healthcare worker sustains a needlestick injury from a known HIV-positive patient's blood. She reports the incident immediately. What is the appropriate management?
A. Wait for 3 months, then test for HIV — the transmission risk from a single needlestick is too low to warrant treatment
B. Test the source patient immediately; if HIV-positive, start TDF+FTC+DTG PEP within 72 hours (ideally <2 hours); continue for 28 days
C. Give IVIG and start corticosteroids to suppress any viral replication — this is more effective than ART for PEP
D. Start single-drug AZT monotherapy for 28 days — this was the original PEP protocol and remains adequate
Reveal Answer
Answer: B. Test the source patient immediately; if HIV-positive, start TDF+FTC+DTG PEP within 72 hours (ideally <2 hours); continue for 28 days
HIV post-exposure prophylaxis (PEP) must be started within 72 hours of exposure — the earlier the better (ideally within 1–2 hours, when the local inflammatory response has not yet facilitated viral spread to lymph nodes). The currently recommended regimen is TDF 300mg + FTC 200mg + DTG 50mg × 28 days (three-drug combination, consistent with current NACO and WHO PEP guidelines). Single-drug AZT monotherapy (the original 1995 protocol) has been superseded — three-drug regimens have lower treatment failure rates. The source patient should be tested, and if HIV status is confirmed positive, PEP continues to completion. If source patient is HIV-negative, PEP can be stopped. Risk of transmission from a single hollow-bore needlestick is approximately 0.3% — low but non-negligible; PEP reduces this by >80%.