Page 7 of 46
PH8.3 | PH8.3 | Antibacterial Drug Classes — SDL Guide — SDL Guide (Part 3)
Newer Antibacterials and Resistance-Breakers
As resistance to established classes has grown, a new generation of antibacterials has been introduced to cover organisms that older drugs can no longer treat. Understanding their mechanisms and stewardship context is essential for a modern prescriber.
Linezolid (oxazolidinone class) binds the 23S rRNA of the 50S ribosomal subunit at a site that overlaps with both chloramphenicol and lincosamide binding sites, but uniquely, it blocks the initiation complex (prevents formation of the 70S initiation complex) rather than elongation. This novel mechanism means there is no pre-existing cross-resistance from macrolide-lincosamide-streptogramin B (MLSB) resistance. Linezolid is bacteriostatic against Staphylococcus and Enterococcus (potentially bactericidal against Streptococcus). Key uses: MRSA infections, vancomycin-resistant enterococcal (VRE) infections, MDR-TB (as part of combination regimens — oral bioavailability 100%). ADRs: reversible myelosuppression (especially thrombocytopaenia with prolonged use — monitor CBC weekly); serotonin syndrome risk (weak MAO inhibitor — avoid with SSRIs/SNRIs/pethidine); optic and peripheral neuropathy with long-term use.
Daptomycin (cyclic lipopeptide) inserts its lipid tail into the bacterial cell membrane in a calcium-dependent manner, causing rapid membrane depolarisation, potassium efflux, and irreversible loss of membrane potential → bactericidal. Active only against gram-positive organisms (the outer membrane of gram-negatives prevents daptomycin from reaching the inner membrane). Key use: MRSA bacteraemia and endocarditis; VRE infections. Critical exception: daptomycin is inactivated by pulmonary surfactant — do NOT use for pneumonia (the daptomycin-for-MRSA-pneumonia question is a classic clinical trap; use linezolid or vancomycin for MRSA pneumonia). ADRs: myopathy and rhabdomyolysis — check CK weekly, avoid/use cautiously with statins.
Colistin (polymyxin E) and polymyxin B: last-resort agents for carbapenem-resistant gram-negative organisms (Acinetobacter baumannii, KPC-producing Klebsiella, Pseudomonas). Mechanism: cationic peptide disrupts the outer membrane of gram-negatives by displacing divalent cations (Mg²⁺, Ca²⁺) from lipopolysaccharide phosphate groups, increasing membrane permeability → bactericidal. ADRs: significant nephrotoxicity (dose-limiting; colistin methanesulfonate is the prodrug — renal excretion; dose-adjust in renal impairment); neurotoxicity (paraesthesia, neuromuscular blockade). Despite toxicity, colistin is often the only option for XDR (extensively drug-resistant) gram-negative infections.
Ceftazidime-avibactam: novel combination of a 3rd-generation cephalosporin (ceftazidime) with avibactam, a non-β-lactam β-lactamase inhibitor that inhibits KPC, OXA-48, and AmpC carbapenemases (but NOT metallo-β-lactamases like NDM, VIM, IMP). Used for KPC-producing carbapenem-resistant Enterobacteriaceae (CRE) and carbapenem-resistant Pseudomonas. Ceftazidime-avibactam does NOT cover Acinetobacter (avibactam does not inhibit OXA-23, the predominant Acinetobacter carbapenemase in India).
SELF-CHECK
A patient with MRSA bacteraemia develops MRSA pneumonia simultaneously. The ID team considers daptomycin, linezolid, or vancomycin. Which agent should be AVOIDED specifically for the MRSA pneumonia component and why?
A. Vancomycin — poor lung penetration makes it ineffective for pneumonia
B. Linezolid — causes severe pulmonary toxicity in MRSA pneumonia
C. Daptomycin — inactivated by pulmonary surfactant and should not be used for pneumonia
D. All three are equally effective for MRSA pneumonia
Reveal Answer
Answer: C. Daptomycin — inactivated by pulmonary surfactant and should not be used for pneumonia
Daptomycin must not be used for pneumonia because it is inactivated by pulmonary surfactant — the surfactant binds daptomycin and prevents it from reaching and disrupting bacterial membranes in the lung. Clinical trials confirm inferior outcomes with daptomycin vs vancomycin for MRSA pneumonia. Linezolid (bacteriostatic, excellent lung penetration) or vancomycin (IV) are appropriate choices; the ZEPHyR trial showed linezolid superior to vancomycin for nosocomial MRSA pneumonia (higher tissue penetration, 100% oral bioavailability). Daptomycin remains appropriate for this patient's bacteraemia component.
Clinical Decision-Making: Which Antibacterial When?
Translating drug-class knowledge into prescribing decisions requires a structured approach that integrates syndrome, likely pathogen, host factors, and local resistance patterns. The following framework organises antibacterial selection for the most common clinical scenarios encountered in Year-2 training and clinical practice.
Community-acquired pneumonia (CAP): Likely pathogens — S. pneumoniae (most common), Mycoplasma, Chlamydophila pneumoniae, H. influenzae. First-line (mild-moderate outpatient): amoxicillin 500mg TDS (for typical organisms) ± azithromycin/doxycycline (for atypicals); OR levofloxacin monotherapy (if atypical cannot be excluded and β-lactam allergy). Hospitalised: IV amoxicillin-clavulanate + azithromycin/doxycycline; or ceftriaxone + azithromycin; or levofloxacin monotherapy. Severe CAP/ICU: ceftriaxone + azithromycin; add vancomycin or linezolid if MRSA risk factors.
Urinary tract infection (UTI): Uncomplicated (young women): nitrofurantoin 100mg MR BD × 5 days (preferred — low systemic effects); TMP-SMX 960mg BD × 3–5 days (if local resistance <20%); fosfomycin 3g single dose. Complicated/pyelonephritis: ceftriaxone IV then oral cefixime/ciprofloxacin based on culture. ESBL UTI/sepsis: meropenem (oral ertapenem available for outpatient step-down).
Skin and soft tissue infections (SSTI): Non-purulent (streptococcal): amoxicillin or penicillin V; cephalexin. Purulent (staphylococcal): cloxacillin (non-MRSA); TMP-SMX or doxycycline (community MRSA — if sensitive); vancomycin (hospital MRSA).
Bacterial meningitis (adults): Empiric: ceftriaxone 2g IV BD + dexamethasone; add ampicillin if age >50 years or immunocompromised (Listeria coverage). Cover S. pneumoniae, N. meningitidis; penicillin allergy: chloramphenicol (if not available) or meropenem.
Host factors: Penicillin allergy (true IgE): use cephalosporins (< 2% cross-reactivity) cautiously, or azithromycin/clindamycin for gram-positives, aztreonam for gram-negatives. Renal impairment: reduce dose/extend interval of aminoglycosides, vancomycin, β-lactams (renally excreted). Pregnancy: safe — amoxicillin, cephalosporins, azithromycin, clindamycin, nitrofurantoin (but avoid near term — neonatal haemolysis). AVOID in pregnancy: fluoroquinolones (theoretical teratogenicity, cartilage), tetracyclines (bones/teeth), aminoglycosides (fetal VIII nerve), TMP-SMX near term (kernicterus).
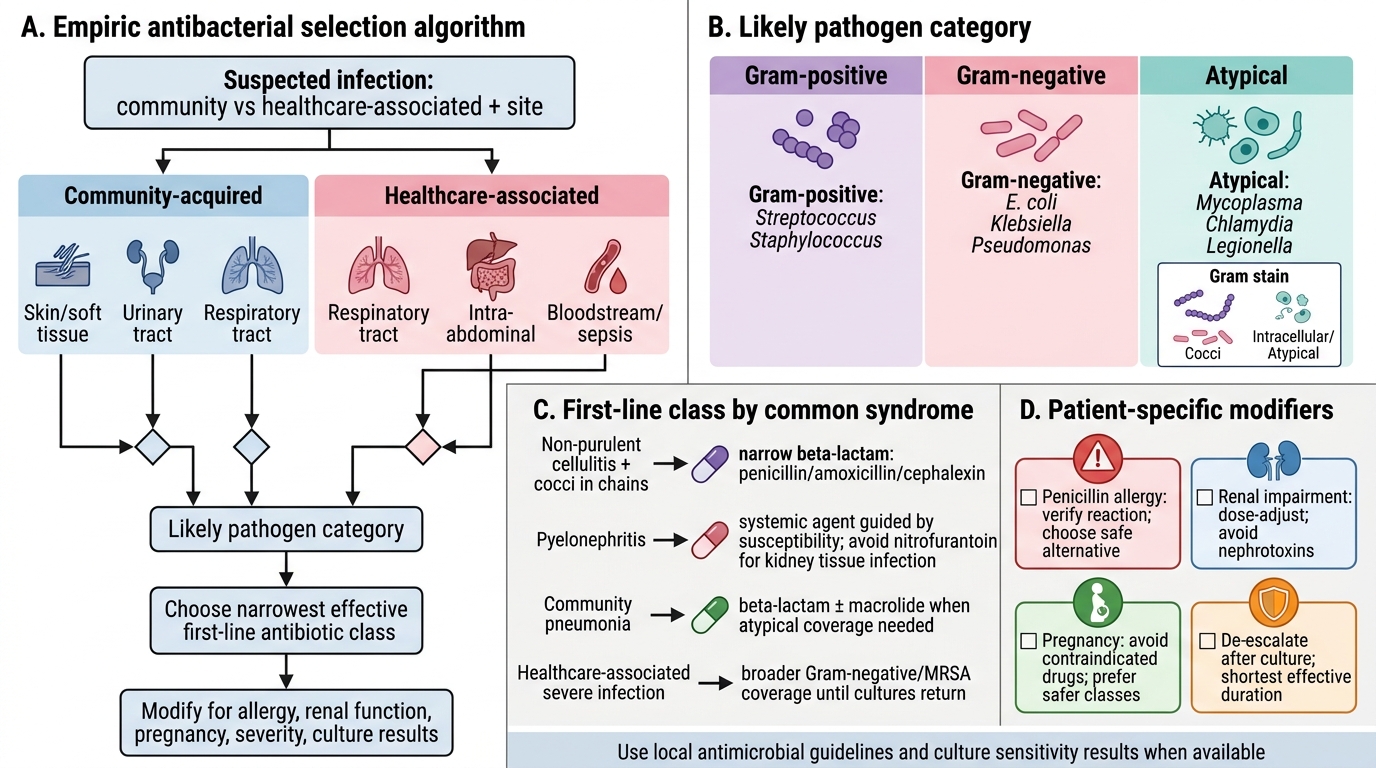
Algorithm for Empiric Antibacterial Drug Selection
Self-Assessment: Antibacterial Drug Selection
Review these clinical scenarios before looking at the discussion:
Scenario A: A 45-year-old man presents with right leg erythema, warmth, and tenderness consistent with non-purulent cellulitis. No fever. No recent hospitalisation. Gram stain from an aspirate shows gram-positive cocci in chains. What is your antibiotic choice and why?
Discussion: Non-purulent cellulitis in a community patient with gram-positive cocci in chains is streptococcal (S. pyogenes — Group A Strep). First-line: oral penicillin V (if available) or amoxicillin 500mg TDS × 5–7 days. Cephalexin is an acceptable alternative. There is no indication for anti-MRSA coverage (non-purulent, community-acquired, gram-positive cocci in chains not clusters). The narrowest effective spectrum — penicillin — is the correct choice.
Scenario B: A 25-year-old woman with no prior kidney disease has fever, right flank pain, and pyuria. Urine culture shows E. coli sensitive to ciprofloxacin (50% local resistance) and nitrofurantoin (90% local sensitivity). She has no drug allergies and is not pregnant. What do you prescribe for pyelonephritis?
Discussion: For pyelonephritis (upper UTI), nitrofurantoin is NOT appropriate — it does not achieve adequate tissue/blood concentrations for parenchymal infection (its activity is limited to urine). Despite 50% local ciprofloxacin resistance, the individual sensitivity result (sensitive) makes ciprofloxacin or levofloxacin appropriate for empiric and directed therapy of pyelonephritis. Oral ciprofloxacin 500mg BD × 7–10 days (with IV initiation if severely unwell). Cefixime (oral 3rd-gen cephalosporin) is an alternative.
Scenario C: During an ICU ward round, you note a patient on meropenem + gentamicin for Pseudomonas VAP. Day 3 — the patient is improving. The microbiologist suggests de-escalating gentamicin. The intensivist says, 'But combination prevents resistance.' Is this claim supported by evidence? What do you recommend?
Discussion: Evidence does NOT support routine combination therapy for prevention of resistance in gram-negative infections. Once clinical improvement is established and the organism is sensitive to meropenem monotherapy, gentamicin can be de-escalated — this reduces nephrotoxicity and ototoxicity risk without compromising outcomes. Combination therapy was indicated for empiric broad coverage pending cultures; it is NOT a resistance-prevention strategy for an identified organism (with the specific exception of Pseudomonas endocarditis and some TB regimens). Recommend gentamicin de-escalation at day 3, continue meropenem for the standard VAP course (8 days for non-Pseudomonas, up to 14 days for Pseudomonas).
CLINICAL PEARL
Nitrofurantoin for UTI — not for pyelonephritis, not for renal impairment. Nitrofurantoin achieves high urinary concentrations but low tissue/serum levels — it is ideal for uncomplicated lower UTI but completely inappropriate for pyelonephritis, bacteraemia, or any infection requiring tissue penetration. Additionally, nitrofurantoin requires renal excretion for its urinary concentration; in eGFR < 30 mL/min it neither achieves adequate urine levels nor is adequately cleared — risk of accumulation and pulmonary toxicity (chronic nitrofurantoin lung). Always check eGFR before prescribing nitrofurantoin.