Page 6 of 46
PH8.3 | PH8.3 | Antibacterial Drug Classes — SDL Guide — SDL Guide (Part 2)
Cell-Wall Inhibitors: Beta-Lactams and Glycopeptides
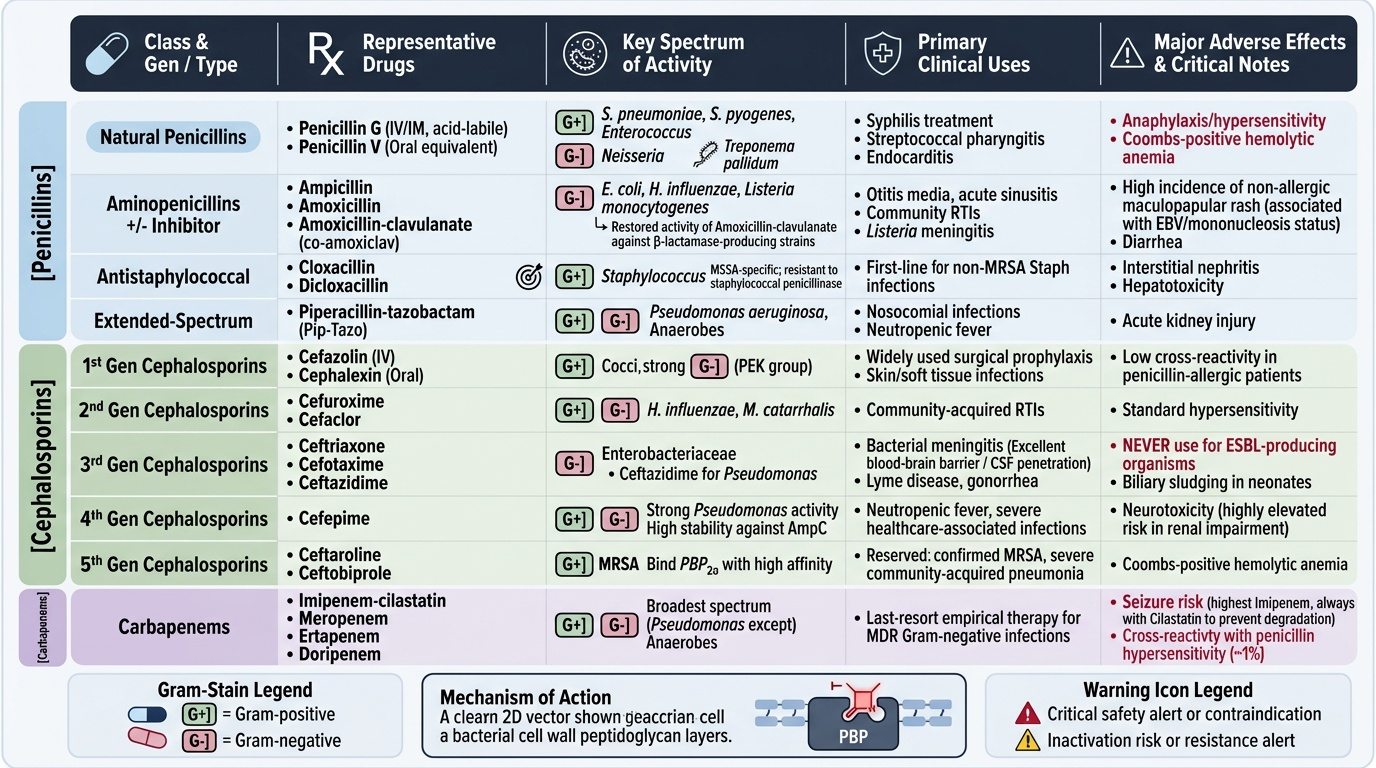
Beta-lactam antibiotics are the most widely used antibacterial class globally, sharing the β-lactam ring that binds and inactivates penicillin-binding proteins (PBPs) — the transpeptidase enzymes responsible for the final cross-linking step in peptidoglycan biosynthesis. Inhibition of PBPs leads to accumulation of peptidoglycan precursors, activation of autolysins, and bacterial cell lysis. Because peptidoglycan is absent in mammalian cells, β-lactams have an exceptionally wide therapeutic index in patients without hypersensitivity.
Penicillins: Penicillin G (benzylpenicillin) — the prototype; active against gram-positive cocci (S. pneumoniae, S. pyogenes, Enterococcus), Neisseria, Treponema pallidum; given IV/IM (acid-labile). Penicillin V — oral equivalent. Ampicillin/amoxicillin — extended spectrum including gram-negatives (E. coli, H. influenzae, Listeria) but susceptible to β-lactamases; amoxicillin-clavulanate (co-amoxiclav) restores activity against β-lactamase-producing organisms. Cloxacillin/dicloxacillin — penicillinase-resistant penicillins; first-line for non-MRSA Staphylococcus. Piperacillin-tazobactam — broad-spectrum including Pseudomonas and anaerobes.
Cephalosporins (PBP inhibitors with a different ring structure conferring greater resistance to many β-lactamases):
- 1st generation (cephalexin, cefazolin): gram-positive cocci, limited gram-negative; cefazolin used for surgical prophylaxis
- 2nd generation (cefuroxime, cefaclor): extended gram-negative (H. influenzae, Moraxella); cefuroxime for community RTIs
- 3rd generation (ceftriaxone, cefotaxime, ceftazidime): expanded gram-negative including Enterobacteriaceae; ceftriaxone/cefotaxime for meningitis (excellent CSF penetration); ceftazidime for Pseudomonas. Note: ceftriaxone/cefotaxime are inactivated by ESBLs — NEVER use for ESBL organisms even if in vitro 'sensitive' (inoculum effect; clinical failure documented).
- 4th generation (cefepime): similar to 3rd but more stable against AmpC β-lactamases; Pseudomonas activity
- 5th generation (ceftaroline, ceftobiprole): MRSA activity (binds PBP2a); reserved for MRSA infections
Carbapenems (imipenem-cilastatin, meropenem, ertapenem, doripenem): broadest-spectrum β-lactams; stable against most ESBLs and AmpC; last-resort for multidrug-resistant gram-negatives. Imipenem hydrolysed in kidney → cilastatin co-administered as dehydropeptidase inhibitor. Meropenem preferred for CNS (imipenem pro-convulsant at high doses). Ertapenem does NOT cover Pseudomonas or Acinetobacter.
Monobactams (aztreonam): narrow spectrum limited to aerobic gram-negatives; no activity vs gram-positives or anaerobes; minimal cross-allergenicity with penicillins (safe in most penicillin-allergic patients — except ceftazidime allergy).
Beta-lactamase inhibitors (clavulanate, sulbactam, tazobactam, avibactam) are β-lactam compounds that suicide-inhibit β-lactamases, restoring activity of the partner drug. Avibactam (non-β-lactam) inhibits KPC and OXA carbapenemases — used in ceftazidime-avibactam for carbapenem-resistant organisms.
Key β-lactam ADRs: Hypersensitivity (penicillin — IgE: anaphylaxis, urticaria; serum sickness; maculopapular rash especially with ampicillin in EBV). Cross-allergy: < 2% cross-reactivity between penicillins and cephalosporins (shared R1 side-chain — true cross-reactivity is lower than historically taught). Imipenem: seizures at high doses. Ceftriaxone: biliary sludging/pseudolithiasis (avoid in neonates and with concurrent calcium IV).
Vancomycin — glycopeptide; binds D-Ala-D-Ala terminus of peptidoglycan precursor, blocking transglycosylation and transpeptidation. Bactericidal for gram-positive organisms. Key uses: MRSA (IV), severe Clostridioides difficile colitis (oral vancomycin — not absorbed, acts luminally). ADRs: Red Man Syndrome (flushing, erythema of neck/face — due to histamine release from mast cells, NOT an allergy; prevented by slowing infusion rate); nephrotoxicity (enhanced by aminoglycosides); ototoxicity. Requires therapeutic drug monitoring (AUC/MIC 400–600).
Provided image
SELF-CHECK
A patient on amoxicillin-clavulanate for a dental infection develops a diffuse, non-pruritic maculopapular rash on day 5, with no angioedema or bronchospasm. He has been told he has a 'penicillin allergy' since childhood. What is the most appropriate interpretation?
A. This confirms a true IgE-mediated penicillin allergy — avoid all β-lactams permanently
B. This is likely a non-allergic drug rash (not IgE-mediated); formal allergy evaluation is needed before labelling as penicillin allergic
C. Switch to a carbapenem immediately to avoid all cross-reactive β-lactams
D. This reaction indicates Clostridioides difficile infection — stop antibiotics and test
Reveal Answer
Answer: B. This is likely a non-allergic drug rash (not IgE-mediated); formal allergy evaluation is needed before labelling as penicillin allergic
A maculopapular (non-urticarial, non-anaphylactic) rash without systemic features is typically a non-IgE-mediated drug reaction, not a true penicillin allergy. True IgE-mediated allergy (anaphylaxis, urticaria, angioedema) is far less common than the prevalence of 'penicillin allergy' labels suggests — studies show 80–95% of patients labelled penicillin-allergic tolerate penicillin on formal challenge. A childhood rash should not permanently bar a patient from β-lactams without formal allergy evaluation. Reflexively switching to carbapenems drives resistance and is not indicated here.
Protein Synthesis Inhibitors: Aminoglycosides, Macrolides, Tetracyclines
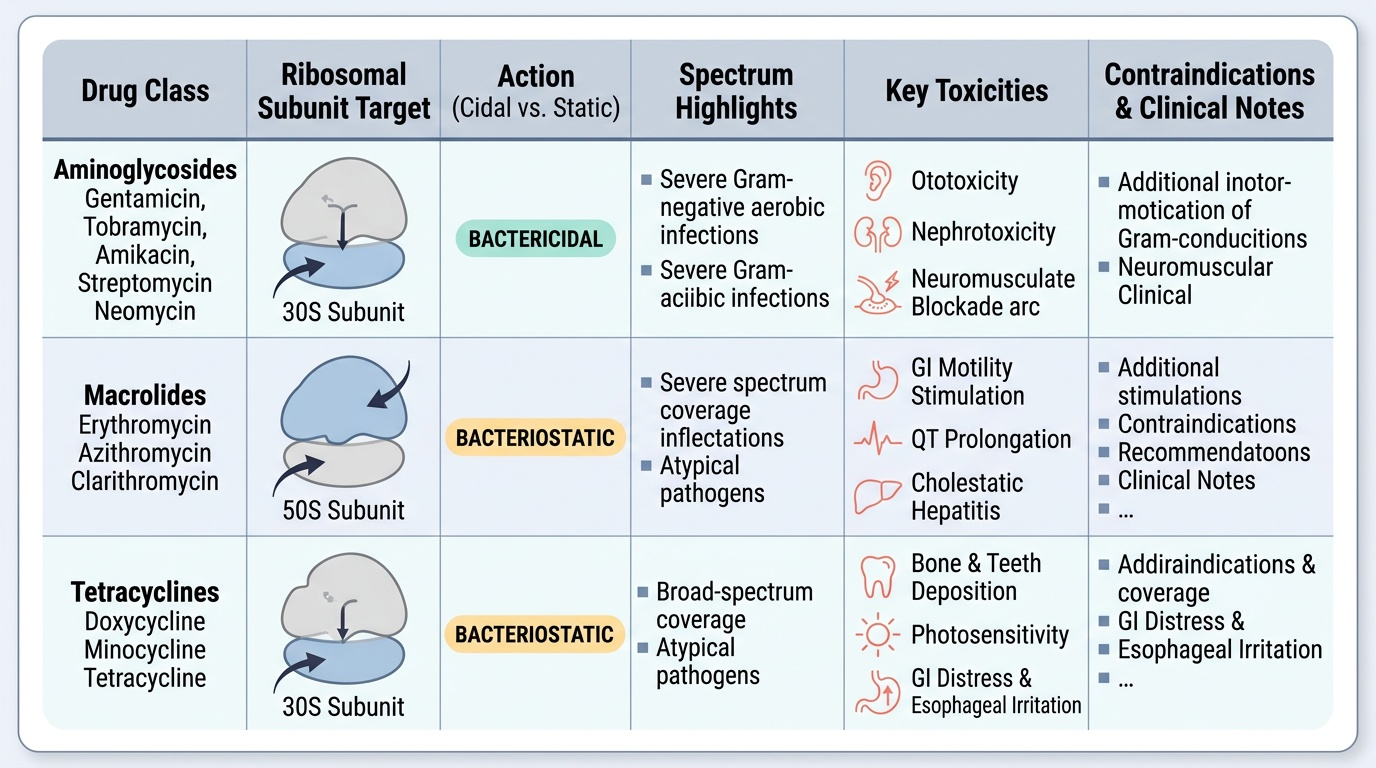
Aminoglycosides (gentamicin, tobramycin, amikacin, streptomycin, neomycin) are bactericidal protein synthesis inhibitors — the major exception to the rule that protein-synthesis inhibitors are bacteriostatic. Mechanism: aminoglycosides enter the bacterial cell via an oxygen-dependent active transport system (explaining their lack of activity against strict anaerobes — no O2-dependent uptake), bind irreversibly to the 16S rRNA of the 30S subunit, cause codon misreading, and generate aberrant proteins that insert into the bacterial membrane, causing membrane disruption and cell death. The killing is concentration-dependent with prolonged post-antibiotic effect (PAE), making once-daily extended-interval dosing optimal.
Clinical uses: gram-negative aerobic infections (including Pseudomonas), in combination with β-lactams; streptomycin for TB (first-line in certain regimens) and plague; neomycin (oral) for bowel decontamination (not absorbed systemically).
ADRs — the two major organ toxicities are dose- and duration-related:
- Nephrotoxicity: proximal tubular damage via free-radical generation; risk factors: prolonged therapy, pre-existing renal disease, volume depletion, concurrent NSAIDs/vancomycin/ciclosporin. Drug-free troughs (extended-interval dosing) allow tubular recovery and reduce accumulation.
- Ototoxicity (irreversible): cochlear damage (high-frequency hearing loss, then tinnitus) and vestibular damage (disequilibrium, nystagmus); irreversible because cochlear hair cells do not regenerate. Streptomycin predominantly vestibular; amikacin and gentamicin predominantly cochlear.
- Neuromuscular blockade: at very high doses, aminoglycosides inhibit presynaptic acetylcholine release; dangerous in patients with myasthenia gravis.
Amikacin is the aminoglycoside least susceptible to aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases, nucleotidyltransferases) — used when resistance to gentamicin/tobramycin is suspected.
Macrolides (erythromycin, azithromycin, clarithromycin) bind to the 50S ribosomal subunit (23S rRNA of the 50S), blocking the tunnel through which the growing peptide exits, inhibiting peptide translocation. They are bacteriostatic (bactericidal at high concentrations vs highly susceptible organisms). Spectrum: gram-positive cocci (S. pneumoniae, S. pyogenes, S. aureus) and atypical organisms (Mycoplasma pneumoniae, Chlamydia, Legionella, Bordetella pertussis) — making them first-line for community-acquired pneumonia with atypical coverage, and whooping cough. Azithromycin has extended activity against H. influenzae and some gram-negatives. Macrolides do NOT cover gram-negative enteric organisms.
ADRs: erythromycin — GI intolerance (stimulates motilin receptors — prokinetic effect, nausea/diarrhoea), QT prolongation (risk of torsades de pointes — avoid in hypokalaemia, with other QT-prolonging drugs), CYP3A4 inhibitor (erythromycin > clarithromycin > azithromycin — drug interactions with statins, warfarin, carbamazepine). Azithromycin has fewer GI effects and fewer drug interactions; once-daily dosing with tissue accumulation and long half-life (tissue half-life ~68 hours — 5-day course achieves 10-day tissue levels).
Tetracyclines (tetracycline, doxycycline, minocycline) and tigecycline (glycylcycline): reversibly bind the 30S subunit, blocking aminoacyl-tRNA attachment to the A site → bacteriostatic. Broad spectrum: gram-positives, gram-negatives, atypicals (Chlamydia, Mycoplasma, Rickettsia, Brucella), spirochaetes. Key uses: Rickettsia (drug of choice — drug of choice for scrub typhus/Rocky Mountain spotted fever), Chlamydia (urogenital), brucellosis (doxycycline + rifampicin), acne (doxycycline), malaria prophylaxis (doxycycline), cholera (doxycycline).
ADRs: Avoid in children <8 years and pregnancy — tetracyclines chelate calcium ions, depositing in bones (stunted growth) and teeth (yellow discolouration, enamel dysplasia — permanent). GI irritation (oesophageal ulcers — take with water, remain upright). Photosensitivity (doxycycline > tetracycline). Hepatotoxicity at high doses (especially in pregnant women — IV administration). Superinfection with oral/vaginal candida. Milk/antacids/iron reduce absorption (chelation — take tetracyclines 2 hours before or after calcium-containing products).
Provided image
SELF-CHECK
A 30-year-old woman presents with fever, headache, and a diffuse macular rash 10 days after returning from a trek in Uttarakhand. Rickettsia prowazekii (epidemic typhus) is suspected. She is 6 weeks pregnant. Which antibiotic management is most appropriate?
A. Doxycycline — drug of choice for rickettsial infections despite pregnancy
B. Azithromycin — safer in pregnancy, adequate rickettsia coverage
C. Ciprofloxacin — broad-spectrum, safe in pregnancy for severe infections
D. Amoxicillin — safe in pregnancy and covers Rickettsia
Reveal Answer
Answer: A. Doxycycline — drug of choice for rickettsial infections despite pregnancy
Doxycycline is the drug of choice for rickettsial infections (Rickettsia, scrub typhus) even in pregnancy, because the risk of untreated rickettsial disease (mortality up to 30% without treatment) outweighs the risk of the drug. In the context of a potentially fatal rickettsial infection, doxycycline is used despite the general caution against tetracyclines in pregnancy — this is a critical clinical judgement. Azithromycin is sometimes used for mild scrub typhus but evidence is weaker; for serious rickettsial disease, doxycycline is preferred. Amoxicillin has no activity against Rickettsia. Fluoroquinolones are generally avoided in pregnancy.
DNA/Metabolic Pathway Inhibitors: Fluoroquinolones and Sulfonamides
Fluoroquinolones target bacterial DNA gyrase (a type II topoisomerase that introduces negative supercoils, required for DNA replication and transcription) and topoisomerase IV (required for chromosome segregation after replication). In gram-negative bacteria, GyrA is the primary target; in gram-positives, ParC (topoisomerase IV subunit) is the primary target. Fluoroquinolones stabilise the enzyme-DNA 'cleavage complex', preventing re-ligation of the cut DNA strand — creating double-strand DNA breaks → bactericidal, concentration-dependent (AUC/MIC and Cmax/MIC driven).
Provided image
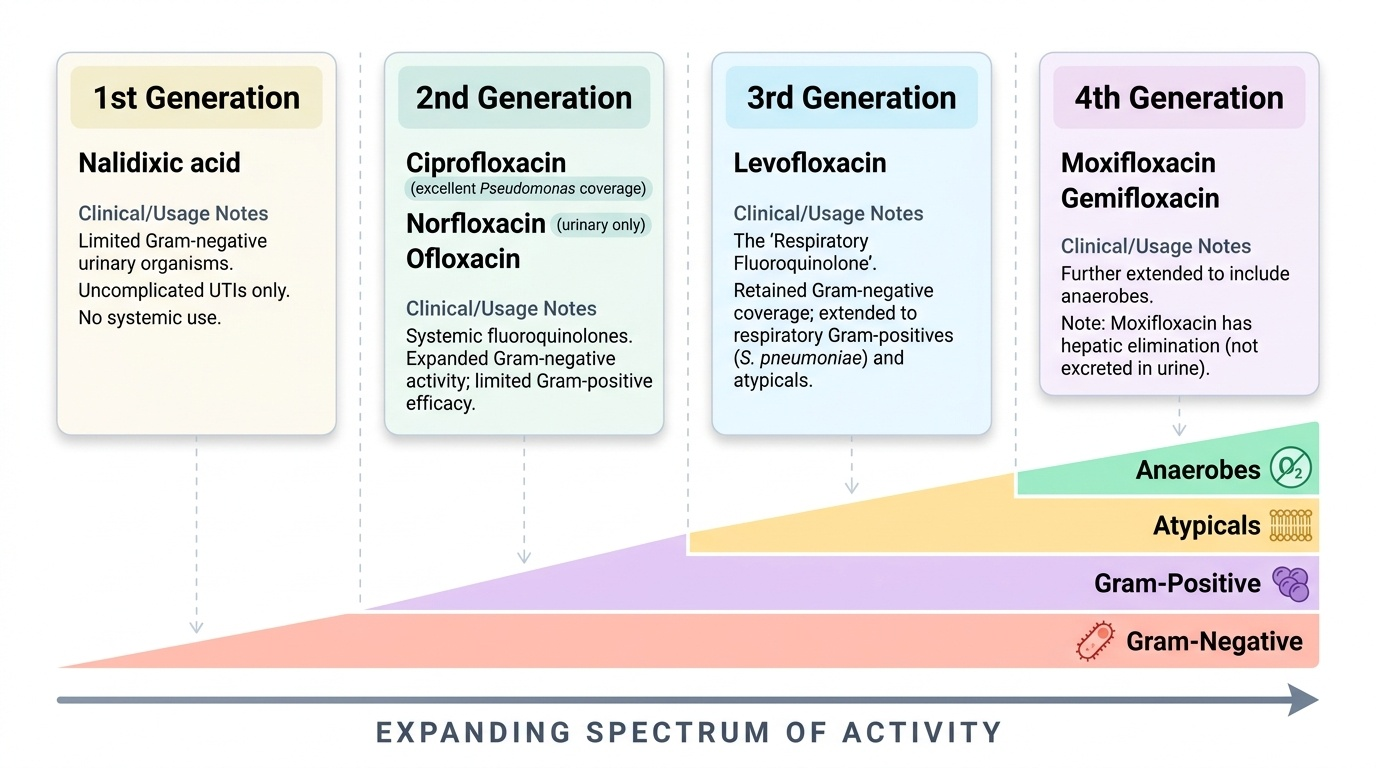
Generations of fluoroquinolones (noting that the 'generation' system is less standardised than for cephalosporins — some sources use 3, some 4 generations):
- 1st generation — nalidixic acid: limited gram-negative urinary organisms; only for uncomplicated UTI; no systemic use; rarely prescribed now.
- 2nd generation (systemic fluoroquinolones) — ciprofloxacin, norfloxacin, ofloxacin: excellent gram-negative activity (including Pseudomonas — ciprofloxacin); limited gram-positive (S. pneumoniae resistance common); norfloxacin limited to urinary tract (poor systemic bioavailability).
- 3rd generation — levofloxacin: extended to include respiratory gram-positives (S. pneumoniae) and atypicals — the 'respiratory fluoroquinolone'; retained gram-negative activity.
- 4th generation — moxifloxacin, gemifloxacin: further extended to include anaerobes; moxifloxacin is NOT excreted in urine (hepatic elimination) — do not use for UTI. Highest risk of QT prolongation among quinolones.
Clinical uses: urinary tract infections (ciprofloxacin, levofloxacin); respiratory infections (levofloxacin, moxifloxacin for CAP/LRTI — 'respiratory quinolones'); enteric fever (ciprofloxacin — now with rising resistance in South Asia; azithromycin increasingly used); gonorrhoea (ciprofloxacin — high resistance in India); anthrax prophylaxis (ciprofloxacin); atypical pneumonia (levofloxacin).
ADRs:
- QT prolongation and risk of torsades de pointes — class effect; moxifloxacin > levofloxacin > ciprofloxacin; avoid with other QT-prolonging drugs (macrolides, antipsychotics), hypokalaemia, congenital long-QT
- Tendinopathy and tendon rupture — Achilles tendon most common; risk increased with corticosteroids and older age (Black Box Warning in FDA labelling)
- Cartilage damage in growing children (animal data) → avoid in children <18 years and pregnancy (exception: certain life-threatening infections, cystic fibrosis with Pseudomonas)
- CNS effects: dizziness, headache, insomnia; seizure risk in epilepsy
- Photosensitivity
- Drug interactions: chelation by antacids, iron, calcium — reduce absorption; inhibit CYP1A2 (ciprofloxacin) → elevated theophylline levels
Sulfonamides and trimethoprim exploit the folate biosynthesis pathway — essential in bacteria (which synthesise folate de novo) but not in humans (who acquire folate from diet). Sulfonamides are structural analogues of PABA (para-aminobenzoic acid), competitively inhibiting dihydropteroate synthase — the first step of bacterial folate synthesis. Trimethoprim inhibits dihydrofolate reductase (DHFR) — the second step. Sequential inhibition in the combination TMP-SMX (cotrimoxazole, in a fixed 1:5 ratio) produces a synergistic, bactericidal blockade of the entire folate pathway.
Clinical uses of TMP-SMX: uncomplicated UTI (where local resistance <20%), Pneumocystis jirovecii pneumonia (PCP) prophylaxis and treatment (in HIV/immunocompromised — high-dose), Nocardia, Toxoplasma prophylaxis. Sulfonamides alone: no longer widely used for bacterial infections; sulfadiazine used in toxoplasmosis (with pyrimethamine), silver sulfadiazine in burns (topical).
ADRs of sulfonamides: Kernicterus in neonates (displace bilirubin from albumin — avoid in late pregnancy and neonates); haemolytic anaemia in G6PD deficiency; Stevens-Johnson syndrome (rare, severe); crystalluria (drink plenty of water); bone marrow suppression with cotrimoxazole (folic acid supplementation may help). Sulfonamide allergy is distinct from sulfonylurea or sulfonyl-containing drug allergy (cross-allergy risk is very low).