Page 9 of 46
PH8.4 | PH8.4 | Syndromic Antibacterial Treatment Plans — SDL Guide — SDL Guide
Learning Objectives
- Devise a pharmacotherapeutic plan for UTI (uncomplicated, complicated, pyelonephritis) with appropriate drug, dose, and duration
- Devise a pharmacotherapeutic plan for common STDs (gonorrhoea, chlamydia, syphilis, PID)
- Explain patient instructions for adherence and partner notification
- Apply Indian resistance data to empiric antibiotic selection for UTI and STD
INSTRUCTIONS
Pharmacotherapeutic planning translates drug-class knowledge into patient-specific prescriptions. For UTI and STDs — the two syndromic groups in PH8.4 — the plan must include the right drug, the right dose, the right duration, AND the instructions you give the patient. In India, rising fluoroquinolone resistance in both UTI pathogens and Neisseria gonorrhoeae has changed first-line choices in the last decade. This SDL builds practical prescribing skills.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 58, 63 (textbook)
- WHO Guidelines for the Treatment of Gonorrhoea, Chlamydial Infections, Syphilis, 2016 updated 2022 (guideline)
- IDSA Guidelines: UTI in Women 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 23-year-old woman presents to the outpatient clinic with dysuria, frequency, and suprapubic discomfort for 2 days. She has no fever, no flank pain. Urine dipstick shows nitrites positive and leucocytes 3+. On detailed questioning, she mentions her partner was recently treated for a urethral discharge at a government clinic. The attending prescribes ciprofloxacin 500mg BD for 7 days. Is this the right drug, dose, and duration? Would the management change if she were pregnant? And how do you incorporate the possibility of a concurrent STD into the plan? This case — common in any outpatient clinic in India — illustrates why syndromic treatment planning requires integrating microbiology, resistance patterns, comorbidities, and patient counselling.
WHY THIS MATTERS
Urinary tract infections are the second most common bacterial infection requiring antibiotic therapy worldwide, and the most common reason antibiotics are prescribed to young women in India. Sexually transmitted infections — gonorrhoea, chlamydia, syphilis — are rising in prevalence nationally, with significant consequences including pelvic inflammatory disease (a leading cause of tubal infertility), congenital syphilis, and HIV risk amplification. The competency PH8.4 specifically requires you to 'devise a pharmacotherapeutic plan AND explain to the patient the instructions and adherence to treatment' — the patient counselling component is not optional. A prescription without clear patient instructions for these conditions leads to treatment failure, reinfection, and ongoing transmission.
RECALL
From the antibacterial classes SDL: nitrofurantoin — works only in urine (not for pyelonephritis, not for eGFR <30); fluoroquinolones (ciprofloxacin, levofloxacin) — broad gram-negative activity, concentration-dependent; tetracyclines (doxycycline) — broad-spectrum including Chlamydia, Treponema, Mycoplasma; avoid in pregnancy (<8 yrs); β-lactams (ceftriaxone, amoxicillin-clavulanate) — cell-wall inhibitors; macrolides (azithromycin) — gram-positives + atypicals including Chlamydia. From microbiology: Neisseria gonorrhoeae — gram-negative diplococcus, intracellular; Chlamydia trachomatis — obligate intracellular organism (needs intracellular-penetrating drugs); Treponema pallidum — spirochaete, not culturable on standard media.
Pathophysiology of UTI and STD: Why Syndrome-Based Planning Matters
Urinary tract infections (UTIs) result from ascending colonisation of the urinary tract, predominantly by enteric gram-negative bacteria. Escherichia coli accounts for 70–85% of community-acquired UTIs in India; other pathogens include Klebsiella pneumoniae (10–15%), Staphylococcus saprophyticus (young women, 5–10%), Enterococcus faecalis, and Proteus mirabilis. The ascending route (urethra → bladder → ureter → kidney) explains why UTI is more frequent in women (shorter urethra, proximity to rectal flora), sexually active patients, those with structural abnormalities (vesicoureteral reflux, stones, obstruction), catheterised patients, and those with diabetes (glycosuria promotes bacterial growth).
Pathogens causing UTI express virulence factors that facilitate adherence and ascent: P fimbriae (type 1 and P pili in uropathogenic E. coli) mediate urothelial adhesion; hemolysin damages urothelial cells; siderophores (aerobactin) acquire iron for growth. Understanding these pathogenesis factors contextualises why some patients have recurrent UTIs (residual fimbriated E. coli in urothelial cells) and why simple hydration and voiding behaviour are non-pharmacological first-line strategies.
Sexually transmitted infections follow a different epidemiology: transmission is by direct contact of mucous membranes or skin. Neisseria gonorrhoeae infects columnar epithelium — urogenital, rectal, pharyngeal. It is an obligate human pathogen with efficient immune-evasion mechanisms (IgA protease, antigenic variation of pili and outer-membrane proteins). Critically, N. gonorrhoeae has developed resistance sequentially to sulfonamides → penicillin → tetracyclines → fluoroquinolones → now extended-spectrum cephalosporins (rare but reported). This resistance history is why each successive WHO gonorrhoea treatment guideline has escalated to a more powerful last-resort drug.
Chlamydia trachomatis (serovars D–K for urogenital) is an obligate intracellular organism that resides within host-cell vacuoles (inclusions), making it invisible to β-lactam antibiotics (which cannot penetrate cells). Only intracellularly-active drugs — doxycycline, azithromycin, fluoroquinolones — are effective. This explains why treating chlamydial cervicitis with amoxicillin fails completely. Treatment of chlamydia is further complicated by frequent asymptomatic carriage (up to 70% of women, 50% of men infected) — underscoring the importance of partner treatment.
Goal of Syndromic Treatment: Cure, Prevent Complications, Stop Transmission
The pharmacotherapeutic plan for UTI and STDs has three simultaneous objectives, all of which must be addressed in the prescription and patient counselling:
Provided image
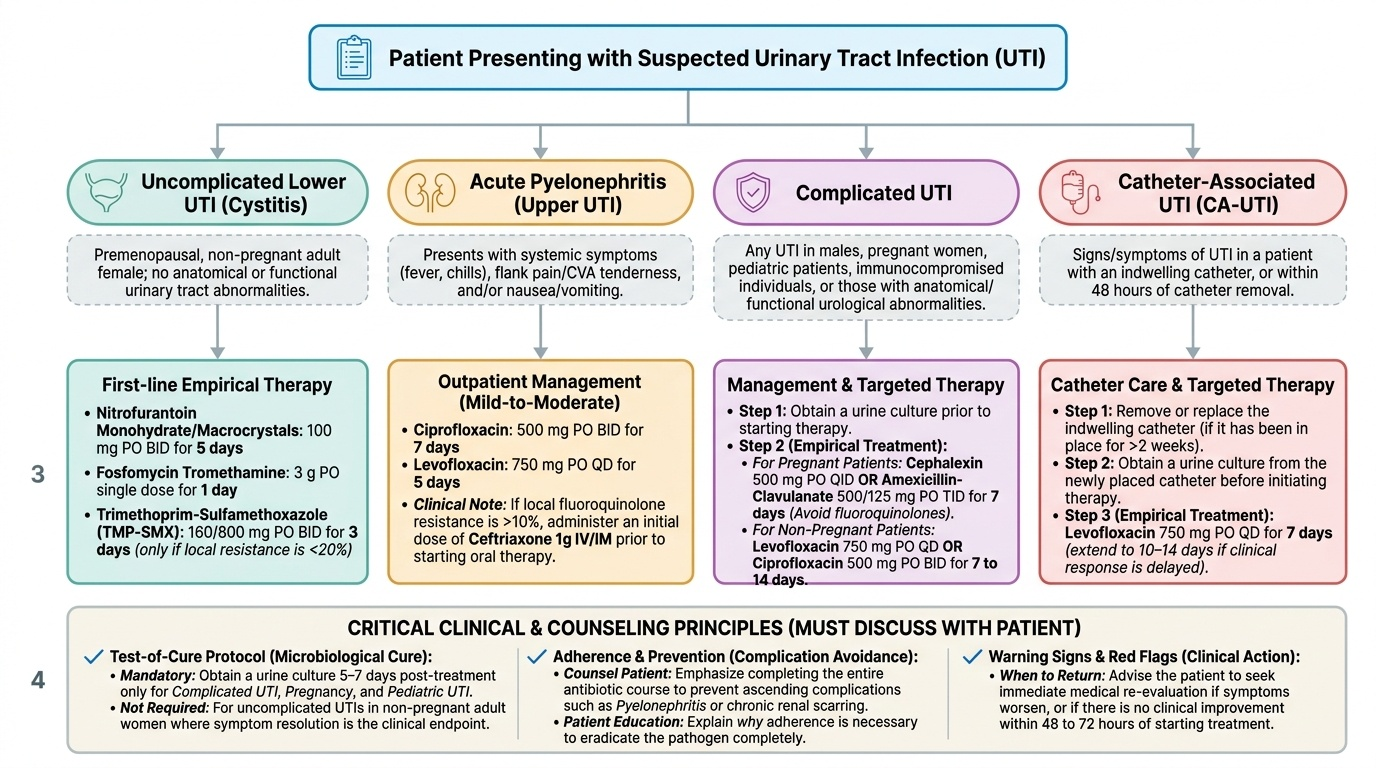
1. Microbiological cure — eradication of the causative organism from the infection site. For UTI, this is confirmed by test-of-cure urine culture 5–7 days after treatment (mandatory only in complicated UTI, pregnancy, and paediatric UTI; not required for uncomplicated UTI in non-pregnant adult women where symptom resolution is the endpoint). For STD, test-of-cure culture or NAAT (nucleic acid amplification test) 2–4 weeks after treatment detects treatment failure.
2. Prevention of ascending complications — the second objective is preventing untreated lower UTI from ascending to pyelonephritis, or untreated urogenital STD from ascending to cause: pelvic inflammatory disease (PID — most serious complication of gonorrhoea/chlamydia in women, causing tubo-ovarian abscess and tubal infertility); epididymo-orchitis in men; haematogenous dissemination (disseminated gonococcal infection — skin pustules, septic arthritis, rare meningitis/endocarditis).
3. Interruption of transmission — treating the patient alone is insufficient for STDs. Partner notification and treatment are integral to the prescription. In India, syndromic management guidelines from the National AIDS Control Programme (NACP) recommend treating sex partners presumptively (without waiting for test results) because: (a) most partners will be culture-positive; (b) waiting for test results leads to reinfection before treatment. 'Expedited partner therapy' (EPT) — prescribing medication for the partner — is evidence-based.
The prescriber must explain all three objectives to the patient. Patients who understand WHY they need to complete the course, WHY their partner needs treatment, and WHEN to return (if symptoms persist or worsen) have significantly better outcomes than those who receive a prescription without explanation.
UTI Classification and Treatment Framework
UTI classification drives treatment choice because the site of infection and host factors determine which drugs will work, which are unnecessary, and what duration is needed.
Uncomplicated lower UTI (acute bacterial cystitis) — young, non-pregnant women with dysuria, frequency, urgency; no fever, no flank pain, no structural urinary abnormality. The diagnosis is clinical + urine dipstick/microscopy; culture is optional (recommended if symptoms persist or recur within 4 weeks).
First-line treatment options (Indian context — 2024):
- Nitrofurantoin 100mg modified-release twice daily × 5 days: preferred — achieves high urinary concentrations, minimal systemic absorption, low resistance rates. Contraindicated: eGFR <30 mL/min (insufficient urinary concentration AND systemic accumulation risk), pyelonephritis (inadequate tissue levels), glucose-6-phosphate dehydrogenase deficiency (haemolysis). Take with food to improve absorption and reduce GI irritation.
- Fosfomycin trometamol 3g single dose (sachet): high urinary levels via concentration in proximal tubule; single dose is an advantage for adherence. Active against most ESBL-producing E. coli — useful when ESBL suspected in uncomplicated UTI.
- TMP-SMX 960mg (1 DS tablet) BD × 3 days: only appropriate if local E. coli resistance is < 20% (check hospital antibiogram — many Indian hospitals now exceed 30–40% resistance).
- Fluoroquinolones (ciprofloxacin, norfloxacin): effective but NOT first-line for uncomplicated UTI due to broad-spectrum nature (drives resistance, C. difficile risk) and rising local resistance in India. Reserve for complicated UTI and pyelonephritis.
Acute uncomplicated pyelonephritis — fever >38°C, flank pain/costovertebral angle tenderness, pyuria. Urine culture MANDATORY (blood cultures if systemically unwell). Oral outpatient therapy appropriate for mild-moderate cases: ciprofloxacin 500mg BD × 7 days OR levofloxacin 750mg once daily × 5 days OR cefixime 400mg BD × 10–14 days (beta-lactam, less efficacious — 14 days). IV therapy (ceftriaxone 1–2g once daily or meropenem for ESBL) for severely ill, vomiting, pregnant women, or failure of oral therapy.
Complicated UTI — any UTI in a patient with structural/functional urinary abnormality (obstruction, stones, vesicoureteral reflux, neurogenic bladder), men (UTI in men is always complex — rule out prostatitis, STD, structural cause), diabetics, immunosuppressed, recent instrumentation. Broader-spectrum therapy (quinolone or cephalosporin) based on culture. Duration 7–14 days. Remove/manage the complicating factor.
Catheter-associated UTI (CAUTI) — treat only if symptomatic (fever, rigors, flank pain, change in mental status in elderly); do NOT treat asymptomatic bacteriuria in catheterised patients — it does not benefit the patient and drives resistance. If treatment is needed: culture-directed; remove catheter and change if possible. Duration: 5–7 days (7–14 days if slow to respond).
Recurrent UTI (≥3 episodes/year in women): investigate for anatomical cause. Prophylactic strategies: low-dose nitrofurantoin 50mg daily × 6–12 months; post-coital single-dose nitrofurantoin; cranberry (modest evidence for PABA/mannose mechanism). Avoid long-term fluoroquinolone prophylaxis (drives resistance).
SELF-CHECK
A 28-year-old non-pregnant woman with uncomplicated lower UTI (dysuria, frequency, no fever) is given a urine dipstick showing nitrites+, leucocytes 3+. The local E. coli resistance to TMP-SMX is 35%. Which of the following is the most appropriate first-line treatment?
A. Ciprofloxacin 500mg BD × 7 days — effective and commonly prescribed
B. TMP-SMX 960mg BD × 3 days — adequate for uncomplicated UTI
C. Nitrofurantoin 100mg MR BD × 5 days — appropriate first-line agent
D. Ceftriaxone 1g IV × 5 days — covers ESBL-producing organisms
Reveal Answer
Answer: C. Nitrofurantoin 100mg MR BD × 5 days — appropriate first-line agent
Nitrofurantoin 100mg modified-release BD × 5 days is the preferred first-line agent for uncomplicated lower UTI in non-pregnant adults. With TMP-SMX local resistance at 35% (well above the IDSA 20% threshold), TMP-SMX is NOT appropriate. Fluoroquinolones (ciprofloxacin) are not first-line for uncomplicated UTI due to their broad-spectrum collateral effects and rising resistance — they are reserved for pyelonephritis and complicated UTI. Ceftriaxone IV is not indicated for uncomplicated lower UTI. Nitrofurantoin is contraindicated in eGFR <30 and pyelonephritis — but this patient has neither.