Page 10 of 46
PH8.4 | PH8.4 | Syndromic Antibacterial Treatment Plans — SDL Guide — SDL Guide (Part 2)
STD Treatment Plans: Gonorrhoea, Chlamydia, Syphilis, PID
Syndromic STD management in India follows WHO guidelines adapted to the national resistance surveillance data. Because microbiological testing (culture, NAAT) is often unavailable or delayed, empiric syndromic treatment is standard practice for STD syndromes (urethral/vaginal discharge, genital ulcer, inguinal bubo, PID).
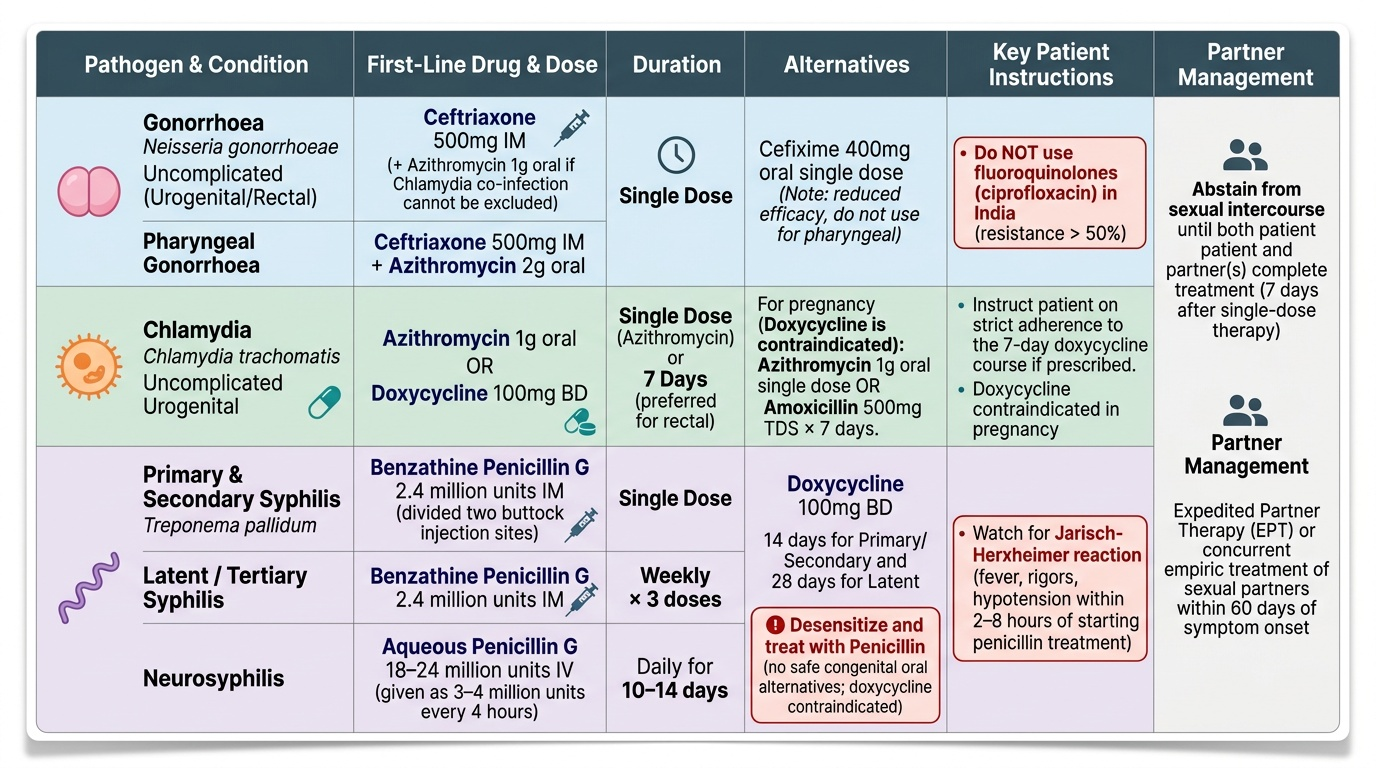
Gonorrhoea (uncomplicated urogenital/rectal/pharyngeal):
Agent: Ceftriaxone 500mg IM single dose (WHO 2022 guidance — the dose was increased from 250mg due to reports of treatment failure and rising ceftriaxone MICs globally, particularly in Japan and Europe). Pharyngeal gonorrhoea requires ceftriaxone 500mg IM + azithromycin 2g orally (for enhanced cure rate). If injectable not available: cefixime 400mg oral single dose (reduced efficacy — not preferred for pharyngeal). Do NOT use fluoroquinolones (ciprofloxacin) for gonorrhoea in India — fluoroquinolone resistance in N. gonorrhoeae exceeds 50% nationally. Dual therapy with azithromycin 1g orally is added when chlamydia co-infection cannot be excluded (common practice — covering both in a single visit).
Chlamydia (uncomplicated urogenital):
- Azithromycin 1g orally single dose (preferred for compliance — one dose observed therapy; pharmacokinetic advantage of high tissue accumulation, extended half-life)
- Doxycycline 100mg BD × 7 days (equally effective for genital chlamydia; preferred for rectal chlamydia based on NAAT-based trials showing higher cure rates)
- Contraindicated in pregnancy: doxycycline → azithromycin 1g single dose OR amoxicillin 500mg TDS × 7 days (pregnancy-safe alternatives).
Syphilis (Treponema pallidum):
- Primary/secondary syphilis: benzathine penicillin G 2.4 million units IM single dose (half into each buttock)
- Latent syphilis (duration unknown or >1 year) / Tertiary syphilis: benzathine penicillin G 2.4 million units IM weekly × 3 doses
- Neurosyphilis: aqueous penicillin G 18–24 million units IV per day (as 3–4 million units every 4 hours) × 10–14 days
- Penicillin allergy (non-pregnant): doxycycline 100mg BD × 14 days (primary/secondary); 28 days (latent). Penicillin allergy in pregnancy: desensitise and give penicillin — there is NO safe oral alternative for congenital syphilis prevention; doxycycline must not be used in pregnancy.
- Jarisch-Herxheimer reaction: fever, rigors, hypotension within 2–8 hours of first penicillin dose for syphilis (due to release of Treponema endotoxin from killed organisms); managed with paracetamol; warn patient in advance. NOT an allergy — do NOT withhold subsequent doses.
Pelvic Inflammatory Disease (PID): Polymicrobial (N. gonorrhoeae, C. trachomatis, anaerobes, gram-negative enteric organisms). Covers all likely pathogens:
- Outpatient (mild): ceftriaxone 500mg IM single dose PLUS doxycycline 100mg BD PLUS metronidazole 400–500mg BD × 14 days
- Inpatient (severe, tubo-ovarian abscess, failure of oral therapy): IV ceftriaxone (or cefoxitin) + doxycycline + metronidazole until 24 hours of clinical improvement, then complete 14-day total with oral regimen
- Duration: 14 days total (minimum for clearing upper genital tract infection and preventing tubal damage)
Provided image
Non-Gonococcal Urethritis (NGU): Predominantly C. trachomatis + Ureaplasma urealyticum + Mycoplasma genitalium. Treatment: azithromycin 1g single dose OR doxycycline 100mg BD × 7 days. Note: Mycoplasma genitalium is resistant to azithromycin in 30–50% of cases — moxifloxacin is used for azithromycin-resistant M. genitalium (specialist input required).
SELF-CHECK
A 22-year-old man presents with urethral discharge and dysuria for 3 days. He had unprotected intercourse 1 week ago. Gram stain shows gram-negative diplococci within neutrophils. He claims allergy to penicillin (childhood rash). The clinic has no microbiological testing available. What is the most appropriate management?
A. Ciprofloxacin 500mg single dose — reserve ceftriaxone for penicillin-allergic patients
B. Azithromycin 1g orally — covers both gonorrhoea and chlamydia in a penicillin-allergic patient
C. Ceftriaxone 500mg IM + azithromycin 1g orally — ceftriaxone is safe despite penicillin allergy in >95% of patients
D. Doxycycline 100mg BD × 7 days — the safest option for urethral discharge
Reveal Answer
Answer: C. Ceftriaxone 500mg IM + azithromycin 1g orally — ceftriaxone is safe despite penicillin allergy in >95% of patients
Ceftriaxone 500mg IM is the first-line treatment for gonorrhoea. Fluoroquinolone resistance in N. gonorrhoeae exceeds 50% in India — ciprofloxacin is NOT appropriate. The childhood penicillin 'allergy' (maculopapular rash) is almost certainly not an IgE-mediated allergy, and cross-reactivity between penicillin and cephalosporins is <2% — ceftriaxone is safe in >95% of penicillin-allergic patients. Azithromycin 1g is added to cover likely concurrent chlamydia co-infection (syndromic dual therapy). Doxycycline alone does not reliably cover gonorrhoea. Azithromycin alone as a single 1g dose is suboptimal monotherapy for gonorrhoea (increasing resistance; not WHO-recommended for gonorrhoea monotherapy).
Patient Instructions and Adherence
The NMC competency PH8.4 explicitly requires the prescriber to 'explain to the patient the instructions and adherence to treatment.' Patient counselling is not an afterthought — in UTI and STD management, patient behaviour after prescribing determines treatment success. Key instructions per drug and syndrome:
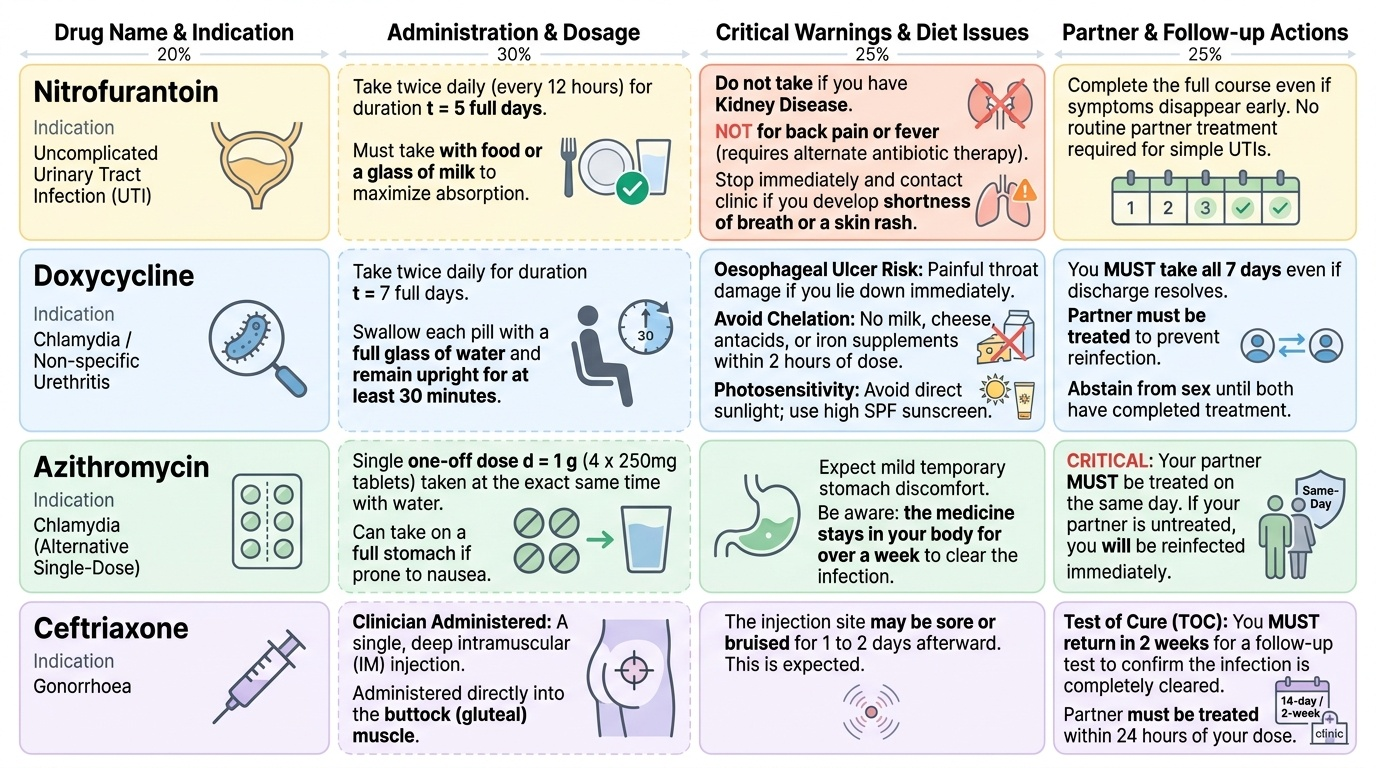
Nitrofurantoin (UTI): 'Take this tablet with food or a glass of milk — it is better absorbed and causes less stomach upset that way. Take it twice a day for 5 full days, even if you feel better sooner. If you develop shortness of breath or a rash, stop and come back. Do not take it if you have kidney disease. Do not use it for back pain or fever — those need a different antibiotic.'
Doxycycline (chlamydia, STD treatment): 'Take this twice daily for 7 days. Swallow each tablet with a full glass of water and stay upright for at least 30 minutes — it can cause painful oesophageal ulcers if you lie down immediately. Do not take it with milk, cheese, antacids, or iron tablets — these prevent the drug from being absorbed (chelation). Avoid direct sunlight during treatment (photosensitivity — use sunscreen). You MUST take all 7 days even if discharge resolves.'
Azithromycin single dose (chlamydia): 'This is a single 4-tablet dose (4 × 250mg). Take all 4 tablets at once with a glass of water. You may have some stomach discomfort — take on a full stomach if needed. Although this is one dose, the drug stays in your system for over a week. Your partner must also be treated today — if your partner is not treated, you will be reinfected.'
Ceftriaxone IM (gonorrhoea): 'This is an injection that is given now, in a single dose, into the buttock muscle. The injection site may be sore for a day or two. You must return in 2 weeks for a test to confirm the infection has cleared. Your partner must be treated at the same visit or within the next 24 hours — if not, the treatment will fail.'
Benzathine penicillin (syphilis): 'You will receive an injection today. For early syphilis, this is a single injection. For late syphilis, you need one injection per week for 3 weeks. You may feel feverish and have muscle aches within a few hours of the injection — this is a normal reaction called the Jarisch-Herxheimer reaction and is not an allergy. Take paracetamol if needed. Your partner(s) from the last 3 months (primary syphilis) or 1 year (secondary) must also be tested and treated.'
Partner notification: For all STDs, the prescriber must explain that every sexual partner from the relevant exposure window requires testing and presumptive treatment. In India, provider-initiated partner notification is standard — the clinician documents this conversation. Failure to treat the partner is the single most common cause of STD treatment failure and reinfection.
Provided image
SELF-CHECK
A 24-year-old pregnant woman (16 weeks gestation) is diagnosed with chlamydial cervicitis. Which treatment is most appropriate?
A. Doxycycline 100mg BD × 7 days — drug of choice for chlamydia
B. Ciprofloxacin 500mg BD × 7 days — safe in second trimester
C. Azithromycin 1g single dose — safe in pregnancy and effective for chlamydia
D. Metronidazole 400mg BD × 7 days — covers intracellular organisms in pregnancy
Reveal Answer
Answer: C. Azithromycin 1g single dose — safe in pregnancy and effective for chlamydia
Azithromycin 1g single dose is the drug of choice for chlamydia in pregnancy. Doxycycline is contraindicated in pregnancy (deposits in fetal bone and developing teeth, causing enamel dysplasia — the chelation mechanism). Fluoroquinolones are avoided in pregnancy due to theoretical fetal cartilage damage. Metronidazole covers anaerobes and protozoa but has no activity against C. trachomatis (an obligate intracellular organism). Azithromycin is safe in pregnancy and achieves high intracellular concentrations effective against Chlamydia.
Clinical Decision-Making in UTI/STD
Several clinical scenarios require modified decision-making beyond the standard protocols. Recognising these situations prevents common prescribing errors.
UTI in a man: All UTIs in adult men are complicated by definition (structural cause, prostatitis, or STD must be excluded). Investigate with renal ultrasound, urethral swab (rule out STD-related urethritis vs cystitis), and urine culture. Prescribe a fluoroquinolone or broad-spectrum beta-lactam based on culture; treat for 7–14 days. A 'UTI' in a young man presenting with dysuria and urethral discharge should be treated as gonorrhoea + chlamydia until proven otherwise.
UTI in pregnancy: All UTIs in pregnancy (including asymptomatic bacteriuria — unlike in non-pregnant adults) MUST be treated — untreated bacteriuria in pregnancy progresses to pyelonephritis in 25–30% of cases and is associated with preterm labour and low birth weight. Safe antibiotics in pregnancy: nitrofurantoin (avoid near term — risk of neonatal haemolysis in G6PD deficiency), cephalosporins (cephalexin), amoxicillin-clavulanate. Culture-guided therapy mandatory. Duration: 5–7 days. Test-of-cure culture required at 1 week post-treatment and monthly thereafter.
STD in pregnancy: Chlamydia → azithromycin (not doxycycline). Gonorrhoea → ceftriaxone IM (safe in pregnancy). Syphilis in pregnancy → MUST give benzathine penicillin even in penicillin allergy after desensitisation — untreated syphilis causes congenital syphilis (hydrops fetalis, stillbirth, multi-organ damage). HIV co-infection: STDs act as cofactors for HIV transmission; STD treatment is part of HIV prevention.
Recurrent UTI evaluation: Before long-term prophylaxis, investigate: renal/bladder ultrasound (structural abnormality, stones, incomplete emptying); exclude diabetes; review sexual history (post-coital timing); urine culture of each episode (confirm bacteria, not just symptoms). Post-menopausal women benefit from topical vaginal oestrogen (restores Lactobacillus-dominant microbiome, lowers urinary pH) as non-antibiotic prevention.
Drug interactions and special populations: Azithromycin + moxifloxacin + ceftriaxone (used together in severe PID) — all three prolong QT interval; check ECG in at-risk patients. Doxycycline absorption reduced by antacids, milk, iron — always time separately. Metronidazole + alcohol (disulfiram-like reaction): warn patients clearly — avoid alcohol during metronidazole and for 48 hours after completion.