Page 13 of 46
PH8.5 | PH8.5 | Tuberculosis Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Explain the types, kinetics, dynamics, therapeutic uses, and adverse effects of drugs used in tuberculosis
- Devise a management plan for tuberculosis treatment in new cases, previously treated cases, and drug-resistant TB
- Monitor and manage major adverse effects of first-line anti-tuberculosis therapy
INSTRUCTIONS
India has the world's largest tuberculosis burden — an estimated 2.8 million new cases annually and approximately 480,000 deaths. As a clinician, you will diagnose and manage TB in every specialty. The pharmacological rationale behind the HRZE regimen is not arbitrary — each drug targets a distinct mycobacterial population, and understanding why makes you a better clinician when patients develop side effects or treatment fails.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 56 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 58 (textbook)
- WHO TB Treatment Guidelines 2022; RNTCP (Revised National TB Control Programme) India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old man is diagnosed with smear-positive pulmonary tuberculosis. He is started on HRZE (isoniazid + rifampicin + pyrazinamide + ethambutol) under DOTS. At week 6, he reports progressive blurring of vision and difficulty distinguishing red from green. His attending dismisses this as 'adjustment to treatment.' Two weeks later, he is functionally blind in one eye. This is a preventable ethambutol-related optic neuritis — one of the most serious and irreversible adverse effects of anti-tuberculosis therapy. Could it have been detected earlier? How do you monitor for it, and what would you have done at week 6? Understanding the pharmacology of ATT — not just the acronym HRZE — would have saved this patient's vision.
WHY THIS MATTERS
Tuberculosis is the second leading infectious cause of death globally after COVID-19, and India accounts for approximately 26% of the global burden. The 6-month HRZE regimen, when completed correctly, is one of the most effective and cost-effective medical interventions in history — but adherence is challenging, adverse effects are common, and drug-resistant TB is an growing catastrophe. The DOTS (Directly Observed Treatment Short-course) programme has saved millions of lives. As a clinician in India, you will encounter TB daily — in medicine, paediatrics, surgery, gynaecology, orthopaedics, and neurology. The pharmacological knowledge in this SDL is directly and immediately applicable.
RECALL
From the antibacterials SDL: rifampicin inhibits bacterial RNA polymerase (beta subunit) — bactericidal; is a potent CYP450 inducer — reduces levels of dozens of co-administered drugs; must never be used as monotherapy (single-step rpoB mutation causes high-level resistance). Isoniazid (INH) is a prodrug activated by mycobacterial catalase-peroxidase (KatG). Pyrazinamide (PZA) is effective only at acidic pH. Ethambutol (EMB) targets cell-wall arabinogalactan synthesis.
From the principles SDL: bacteriostatic vs bactericidal distinction matters — in TB, we need BOTH bactericidal activity (to reduce the viable count rapidly and prevent transmission) AND sterilising activity (to kill dormant bacilli and prevent relapse). No single drug achieves both; the combination does.
Tuberculosis Pathobiology: Why TB is Hard to Treat
Mycobacterium tuberculosis is an extraordinarily successful human pathogen, and its distinctive biology directly determines why treatment requires at least 6 months of multi-drug therapy rather than the 5–14 days sufficient for most bacterial infections.
Three pathobiological features create the pharmacological challenge:
1. Slow replication: M. tuberculosis divides every 15–20 hours — compared to 20 minutes for E. coli. Most antibiotics kill only actively dividing bacteria (they target processes of cell division: cell-wall synthesis, protein synthesis); slow division dramatically reduces the rate of drug-mediated killing. This explains why 6 months of treatment — far longer than any other common bacterial infection — is required.
2. Multiple bacterial populations in different physiological states: In a single patient with pulmonary TB, M. tuberculosis exists in at least four distinct populations, each requiring a different drug to kill it:
- Rapidly dividing, aerobic bacilli (lung cavity walls, high O2): targeted by INH and rifampicin (both highly bactericidal against this population)
- Slowly dividing, semi-dormant bacilli in caseous material (low pH, anaerobic): targeted by pyrazinamide (uniquely active at low pH — activated by mycobacterial pyrazinamidase to pyrazinoic acid)
- Dormant, intracellular bacilli within macrophages (low pH, low O2): targeted by rifampicin and pyrazinamide
- Truly dormant bacilli (metabolically inactive, not killed by any current drug): persist through 6-month treatment and can reactivate years later — the basis of latent TB infection and post-treatment relapse
3. Natural resistance variants in large populations: A cavity containing 10⁸–10⁹ bacilli will statistically contain spontaneous mutants resistant to any single drug. Using a single drug would select for these mutants, leading to acquired drug resistance within weeks. Using three or four drugs simultaneously makes it statistically impossible for a bacillus to harbour simultaneous mutations to all drugs. This is the entire basis of multi-drug therapy for TB — not synergy in the usual sense, but resistance prevention by combinatorial probability.
Therapeutic Goals: Bactericidal, Sterilising, and Resistance Prevention
The pharmacotherapeutic goals of TB treatment define why the regimen is designed as it is. Three actions must occur simultaneously, and different drugs contribute to each:
1. Bactericidal activity (early killing): Rapid reduction of the viable bacillary load within the first 2 months — preventing ongoing transmission and achieving clinical improvement (defervescence, weight gain, sputum smear conversion). Isoniazid is the most potent early bactericidal agent — it has the greatest activity against rapidly dividing aerobic bacilli and achieves the fastest early bacterial kill (early bactericidal activity, EBA). Rifampicin also contributes early bactericidal activity. EBA in the first 2 days of treatment is primarily due to INH.
2. Sterilising activity (late killing): Eradication of semi-dormant and slowly metabolising bacilli — the population responsible for relapse after treatment completion. Rifampicin is the most important sterilising agent; its removal from the regimen mandates 12 months of treatment instead of 6. Pyrazinamide (PZA) uniquely targets slowly metabolising bacilli in acidic environments (caseous lesions, macrophage phagolysosomes) and dramatically shortened TB treatment duration from 12–18 months to 6 months when it was added to the INH+RIF backbone. PZA has virtually no antibacterial activity at neutral pH — it is only active in the acidic environments generated by mycobacterial metabolism.
3. Resistance prevention: As explained above, the combination ensures that natural single-drug-resistant mutants (always present in large bacterial populations) are killed by other drugs before they can multiply and dominate. Ethambutol is added to the HRZE regimen primarily as a resistance-preventing companion — particularly for rifampicin (the drug most critical to shorten treatment; losing it to resistance is catastrophic). Ethambutol is removed in the continuation phase when the bacterial load has been dramatically reduced and resistance-prevention is less critical.
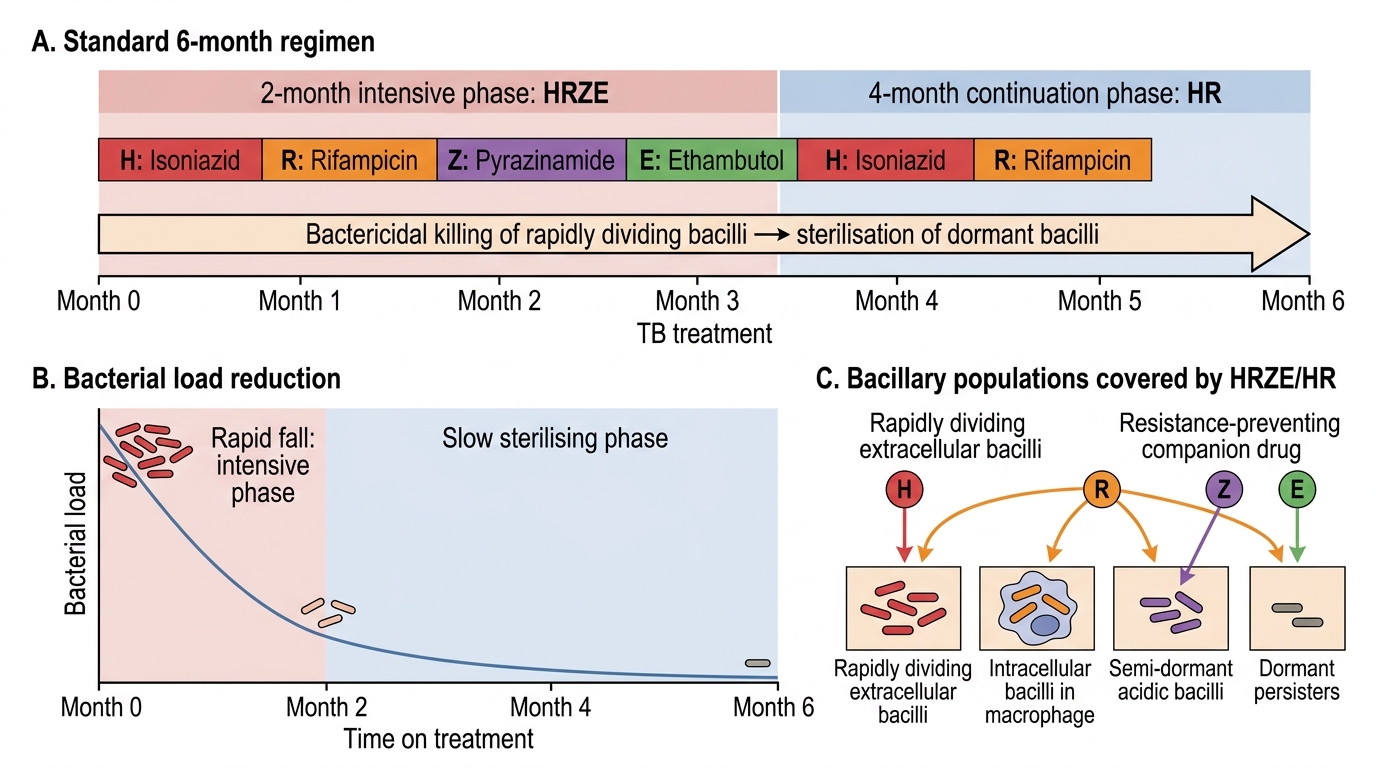
Tuberculosis Treatment Phases and Bacillary Load Reduction
First-Line Anti-Tuberculosis Drugs: HRZE
The four first-line drugs each target a distinct mycobacterial structure or process, and their combination covers all four mycobacterial populations:
Isoniazid (INH, H): The most important ATT drug. Mechanism: INH is a prodrug — mycobacterial catalase-peroxidase (encoded by KatG) activates it to a reactive isonicotinoyl radical, which forms a covalent adduct with NADH. This adduct binds and inhibits InhA (enoyl-ACP reductase), a key enzyme in mycobacterial mycolic acid synthesis. Mycolic acids are long-chain fatty acids essential for the mycobacterial cell wall; INH's inhibition leads to loss of membrane integrity and cell death. INH is bactericidal against actively dividing M. tuberculosis; bacteriostatic against dormant organisms. Resistance: KatG mutation (reduces prodrug activation) is the most common mechanism; InhA promoter mutation (overexpresses the target) also occurs.
Rifampicin (RIF, R): Mechanism: binds the beta subunit of mycobacterial DNA-dependent RNA polymerase — the same target as in other bacteria. Inhibits the initiation of RNA transcription → bactericidal. Active against all TB populations (actively dividing, semi-dormant, intracellular). The most important sterilising agent. Resistance: single-step mutation in rpoB (beta subunit) → high-level rifampicin resistance; this is why rifampicin is NEVER used alone and why detecting rpoB mutation = MDR-TB surrogate (by WHO algorithm, rpoB mutation = assumed MDR-TB for treatment purposes). Important drug interactions: rifampicin is a potent inducer of CYP1A2, CYP2B6, CYP2C9, CYP2C19, CYP3A4, and P-glycoprotein — reduces plasma levels of: oral contraceptives (OCP failure — use barrier contraception), warfarin (INR falls — increase warfarin dose; monitor closely), methadone (withdrawal symptoms), antiretrovirals (major interaction — may require switching to rifabutin in HIV-TB co-treatment), azole antifungals, steroids (double steroid dose during rifampicin).
Pyrazinamide (PZA, Z): Mechanism: PZA is a prodrug — mycobacterial pyrazinamidase (pncA gene product) hydrolyses PZA to pyrazinoic acid (POA). POA is active only in acidic environments (pH < 6.0) — it accumulates in acidic foci (caseous necrosis, macrophage phagolysosomes), disrupts the mycobacterial membrane potential and mycolic acid biosynthesis. PZA has virtually no antibacterial activity at neutral pH and no activity against Mycobacterium bovis (BCG) — which lacks pncA (intrinsically resistant). Essential for shortening treatment from 12 to 6 months; included only in the 2-month intensive phase (acidic environment resolves as lesions heal; no benefit beyond 2 months).
Ethambutol (EMB, E): Mechanism: inhibits arabinosyl transferases encoded by embB gene — enzymes that polymerise arabinose into arabinogalactan, a crucial cell-wall component. EMB prevents cross-linking of the mycobacterial cell wall, inhibiting growth. Bacteriostatic at standard doses; bactericidal at high doses. Primary role: companion drug for resistance prevention — prevents the emergence of rifampicin resistance in the intensive phase. EMB is discontinued at 2 months (once cultures confirm drug sensitivity) because its major adverse effect (optic neuritis — see below) limits long-term use.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
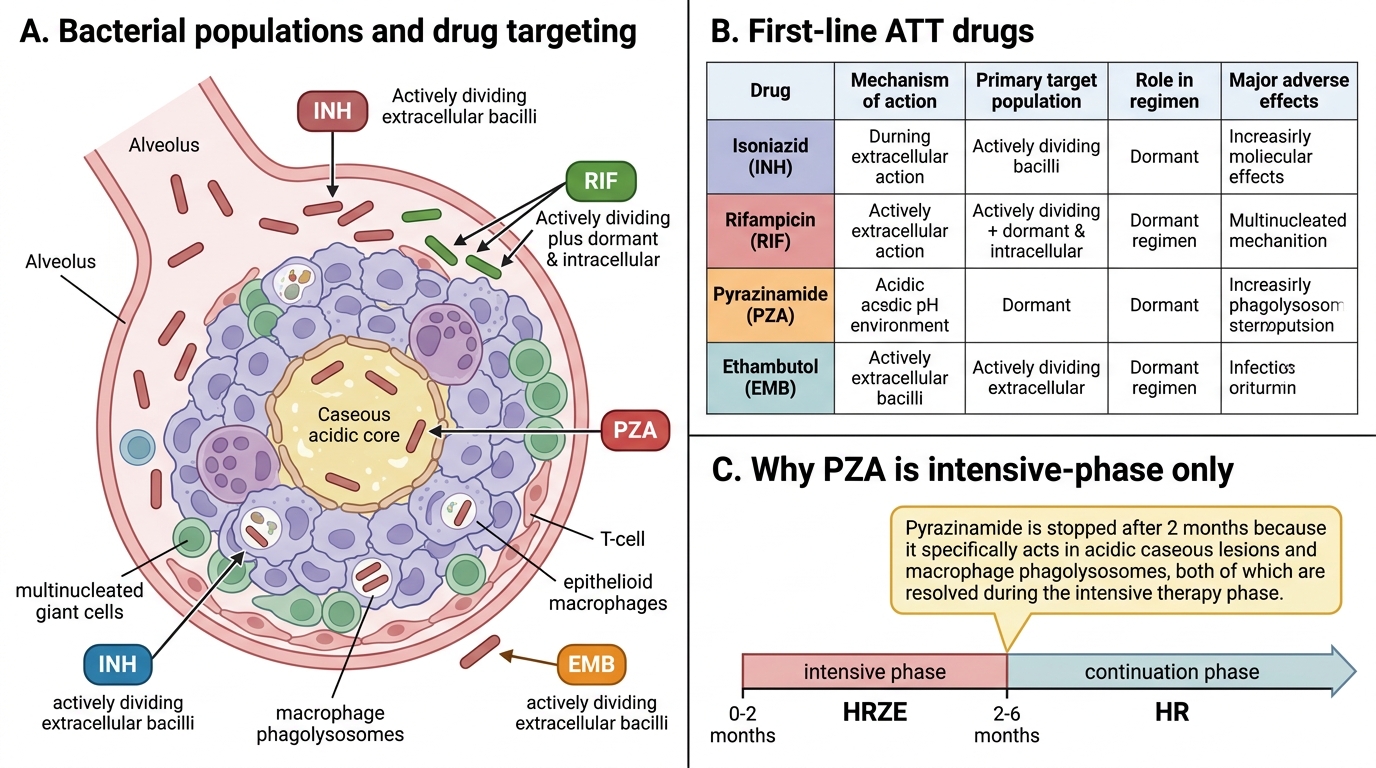
First-Line ATT Drugs and Pyrazinamide Phase-Specific Role
SELF-CHECK
Why is pyrazinamide included only in the intensive (2-month) phase of TB treatment and discontinued in the continuation phase?
A. Pyrazinamide is too toxic for long-term use and must always be stopped at 2 months
B. Pyrazinamide is only active in acidic pH, as found in active caseous lesions; once these resolve (by month 2), it provides no additional benefit
C. Pyrazinamide is an early bactericidal agent equivalent to INH, and INH alone is sufficient after 2 months
D. Pyrazinamide causes drug resistance to rifampicin if used for more than 2 months
Reveal Answer
Answer: B. Pyrazinamide is only active in acidic pH, as found in active caseous lesions; once these resolve (by month 2), it provides no additional benefit
Pyrazinamide (PZA) works by a unique pH-dependent mechanism — its active metabolite (pyrazinoic acid) is generated by mycobacterial pyrazinamidase and is active only in acidic microenvironments (pH <6.0), specifically in caseous lesions and macrophage phagolysosomes where dormant mycobacteria reside. After 2 months of intensive therapy, these acidic foci are largely resolved (healing/sterilisation) and the environment returns toward neutral pH — at which point PZA has no additional antibacterial effect. Continuing it beyond 2 months adds toxicity (hyperuricaemia, hepatotoxicity) without benefit. Toxicity alone is not the reason — the pharmacodynamic rationale is the correct explanation.