Page 14 of 46
PH8.5 | PH8.5 | Tuberculosis Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
HRZE Pharmacokinetics, Adverse Effects, and Monitoring
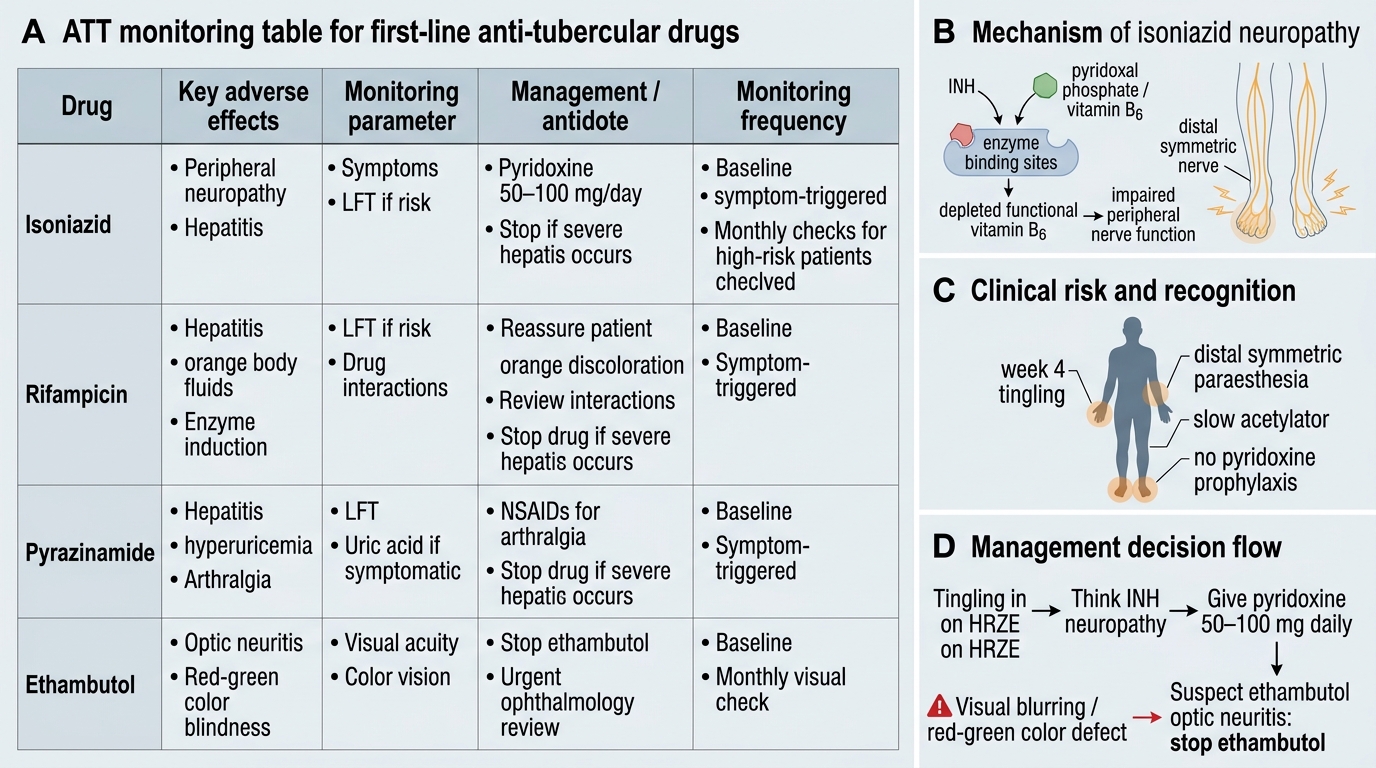
Each first-line ATT drug has a distinctive pharmacokinetic profile and a clinically important toxicity pattern. The prescriber must monitor for these proactively — not wait for the patient to report symptoms, because several toxicities (ethambutol optic neuritis, INH peripheral neuropathy) can become irreversible if not detected early.
Isoniazid (INH):
- PK: well-absorbed orally (bioavailability ~90%); widely distributed including CNS and caseous lesions; hepatic acetylation by N-acetyltransferase 2 (NAT2). Slow acetylators (genetically determined; more common in Caucasians and Middle Easterners; ~50% Indian population) accumulate INH → higher plasma levels → more prone to neuropathy. Fast acetylators clear INH rapidly and may have reduced efficacy on intermittent regimens.
- Peripheral neuropathy (most common serious ADR): INH depletes pyridoxine (vitamin B6) by competing for pyridoxal phosphate — causing tingling, numbness, paraesthesia in hands/feet. Prevention: pyridoxine 10–25mg daily co-administered with INH (mandatory in malnourished, diabetics, HIV+, pregnant, slow acetylators, alcoholics). Treatment of established neuropathy: higher doses of pyridoxine (50–100mg daily).
- Hepatotoxicity: INH → toxic acetylhydrazine metabolite via NAT2 and CYP2E1; risk increased: age >35, alcohol, pre-existing liver disease, slow acetylator genotype, rifampicin co-administration. Monitor LFTs; stop if ALT >3× ULN with symptoms OR >5× ULN asymptomatic.
- Drug interaction: INH inhibits CYP2C19 → elevated phenytoin levels (phenytoin toxicity — ataxia, nystagmus); also inhibits MAO → tyramine interaction (mild), serotonin-related risks.
Rifampicin (RIF):
- PK: well-absorbed (better fasting); hepatic metabolism + biliary excretion (entero-hepatic cycle); induces its own metabolism (autoinduction over 2 weeks).
- Orange discolouration of urine, sweat, tears, and sputum — harmless. MUST warn patient in advance; if not warned, many patients stop treatment thinking they are bleeding internally.
- Hepatotoxicity: rifampicin + INH combination increases hepatotoxicity risk (rifampicin induces CYP2E1 → increased INH toxic metabolite formation). Most hepatotoxicity attributed to INH, but the combination is more hepatotoxic than either drug alone.
- Drug interactions (CYP inducer — as detailed above): OCP failure, warfarin, antiretrovirals, steroids, azoles, methadone, ciclosporin.
- 'Flu syndrome': with intermittent high-dose rifampicin — fever, chills, myalgia; immune-mediated. Managed by switching to daily administration.
- Thrombocytopaenia (rare, immune-mediated — stop rifampicin).
Pyrazinamide (PZA):
- PK: well-absorbed orally; widely distributed including CSF; hepatic metabolism.
- Hyperuricaemia: PZA inhibits renal tubular secretion of urate → elevated serum uric acid (in most patients — nearly universal). Usually asymptomatic; symptomatic gout is an indication to stop PZA. Do NOT use allopurinol during PZA treatment (allopurinol inhibits xanthine oxidase but cannot reverse tubular secretion block; ineffective).
- Hepatotoxicity: dose-related; most hepatotoxic of the first-line drugs in high doses; modern standard doses have lower risk. Check LFTs at baseline and monthly.
- Arthralgia (non-gouty) — common; managed with NSAIDs.
Ethambutol (EMB):
- PK: renally excreted (60% unchanged); dose adjustment required in renal impairment (eGFR < 30 — accumulation → increased optic toxicity). Bacteriostatic.
- Optic neuritis (most feared ADR): dose-dependent, affecting central vision (decreased acuity) AND colour vision (especially red-green). Reversible if detected early; IRREVERSIBLE if treatment continues. Onset: typically after 2 months at standard doses (15 mg/kg). Monitoring: baseline visual acuity + colour vision (Ishihara plates); monthly testing during intensive phase. Ask the patient monthly: 'Have you noticed any blurring, difficulty reading, or trouble distinguishing colours?' STOP EMB immediately if visual changes are noted. Optic neuritis is rare at standard doses (15 mg/kg) and almost exclusively occurs with higher doses (25 mg/kg, used historically) or in renal impairment. Do NOT prescribe standard doses in eGFR <30.
- Contraindicated in children under 6 years (inability to reliably report visual symptoms).
ATT Adverse Effects and Monitoring
SELF-CHECK
A patient on HRZE develops tingling in both feet at week 4. He is a known slow acetylator of INH. He was not given pyridoxine. What is the mechanism of this adverse effect and the management?
A. Ethambutol optic neuritis — stop ethambutol and monitor visual acuity
B. Isoniazid-induced peripheral neuropathy due to pyridoxine depletion — give pyridoxine 50–100mg daily and continue ATT
C. Rifampicin drug-induced neuropathy — switch to ethambutol monotherapy
D. Pyrazinamide-induced arthralgia — give NSAIDs and continue HRZE without modification
Reveal Answer
Answer: B. Isoniazid-induced peripheral neuropathy due to pyridoxine depletion — give pyridoxine 50–100mg daily and continue ATT
Isoniazid competes with pyridoxal phosphate (active vitamin B6) for enzyme binding, depleting functional pyridoxine and causing peripheral neuropathy (tingling, numbness, paraesthesia — predominantly distal, symmetric). Slow acetylators of INH (common in South Asian populations) accumulate higher INH plasma levels and are at higher risk. Management: add pyridoxine 50–100mg daily (higher therapeutic dose to overcome the competitive depletion) — do not stop INH (central to the regimen). Prophylaxis with pyridoxine 10–25mg/day is mandatory for high-risk patients. The tingling is in the feet, not visual — ethambutol optic neuritis affects vision. Rifampicin does not cause peripheral neuropathy. Pyrazinamide causes hyperuricaemia and arthralgia, not tingling.
Treatment Regimens: Categories and Drug-Resistant TB
The RNTCP (Revised National Tuberculosis Control Programme) and its successor programme TB Mukt Bharat (NSP 2017–2025) use standardised treatment categories based on the patient's prior treatment history:
Category I (new patients): First episode of TB, or previously treated patients without documented drug-resistance.
- Standard regimen: 2HRZE / 4HR (notation: number = months; letters = drugs)
- Intensive phase (2 months): HRZE daily — rapid killing of actively dividing bacilli, sputum smear conversion
- Continuation phase (4 months): HR daily — sterilisation of residual dormant bacilli
- Total duration: 6 months
- Drugs are given as Fixed-Dose Combinations (FDCs) under DOTS to improve adherence and prevent selective non-compliance (patient cannot selectively stop one drug from a combined tablet)
- Sputum smear at 2 months (end of intensive phase) — if still positive → extend intensive phase by 1 month, re-evaluate for MDR-TB
Previously treated patients (Category II — historical; now Category I with upfront DST): The previous Category II regimen (2HRZES/1HRZE/5HRE) has been largely superseded. Current WHO/RNTCP guidelines require drug-susceptibility testing (DST) before retreatment — empiric Category II regimen risks treating MDR-TB with inadequate regimens and amplifying resistance.
MDR-TB (multidrug-resistant TB): Defined as resistance to both isoniazid AND rifampicin (with or without other drug resistance). Critically, an organism resistant to rifampicin is treated as MDR-TB for practical purposes (because simultaneous rpoB mutation almost always implies INH resistance is either present or will emerge). MDR-TB treatment regimens are complex, individualised, and supervised by specialist TB centres.
WHO 2022 MDR-TB drug groups for regimen construction:
- Group A (use all three if possible): Levofloxacin or moxifloxacin; Bedaquiline (mycobacterial ATP synthase F1Fo inhibitor — bactericidal, prolonged half-life of ~5.5 months; QT prolongation risk); Linezolid (50S ribosome inhibitor; myelosuppression risk; 9–12-month regimens)
- Group B: Clofazimine; Cycloserine (or terizidone)
- Group C: Remaining reserve drugs: ethionamide/prothionamide; amikacin/streptomycin; PAS; imipenem-cilastatin + amoxicillin-clavulanate; thiacetazone (only if HIV negative — fatal skin reactions in HIV+)
XDR-TB (extensively drug-resistant TB): WHO 2022 definition — MDR-TB plus resistance to any fluoroquinolone AND to bedaquiline or linezolid. XDR-TB has very limited treatment options and high mortality.
The DOTS (Directly Observed Treatment Short-course) strategy — where a health worker or trained observer watches the patient swallow every dose — dramatically reduces treatment failure and drug resistance by ensuring adherence.
SELF-CHECK
A 35-year-old man on HRZE for 6 months develops nausea, vomiting, jaundice, and ALT 8× upper limit of normal. All four ATT drugs are stopped. After 2 weeks, LFTs return to normal. How do you re-introduce ATT?
A. Restart the full HRZE regimen together once LFTs normalise — all four drugs are equally likely to have caused the reaction
B. Permanently discontinue rifampicin — it is the most hepatotoxic drug in the regimen
C. Re-introduce drugs sequentially: rifampicin first (least hepatotoxic), then isoniazid, then ethambutol; monitor LFTs after each addition; pyrazinamide may be omitted if hepatotoxicity recurs
D. Switch to second-line MDR-TB drugs — first-line ATT is contraindicated after hepatotoxicity
Reveal Answer
Answer: C. Re-introduce drugs sequentially: rifampicin first (least hepatotoxic), then isoniazid, then ethambutol; monitor LFTs after each addition; pyrazinamide may be omitted if hepatotoxicity recurs
Sequential re-introduction is the standard approach for ATT-induced hepatotoxicity. The protocol: after LFT normalisation, re-introduce one drug at a time with LFT monitoring after each: rifampicin is introduced first (2–3 days), then isoniazid (another 2–3 days), then ethambutol. Pyrazinamide is the most hepatotoxic among the four and is often omitted or introduced last — if it triggers recurrent hepatotoxicity, the regimen continues without PZA (extending continuation phase to compensate for loss of sterilising activity, usually to 9 months total). This sequential approach identifies the offending drug and allows maximal use of first-line agents. Restarting all four simultaneously after hepatotoxicity risks another severe episode without identifying the causative agent.
Clinical Decision-Making: Monitoring and Managing ATT Toxicity
Proactive monitoring and structured management of ATT adverse effects requires knowing which toxicities are time-critical (irreversible if missed) versus manageable without stopping treatment.
Monitoring schedule: At treatment initiation: baseline LFTs, serum uric acid, visual acuity + colour vision (Ishihara plates for ethambutol), renal function (for ethambutol dose adjustment). Monthly: LFTs (especially for INH/PZA hepatotoxicity), visual acuity + colour vision (for EMB). Clinical review at 2 weeks: neuropathy symptoms (INH). Sputum smear/culture: at 2 months and at treatment completion.
Management decision tree for hepatotoxicity:
- ALT <3× ULN, no symptoms → continue ATT, monitor more frequently
- ALT 3–5× ULN with symptoms (nausea, jaundice) OR >5× ULN asymptomatic → stop all hepatotoxic ATT drugs (INH, RIF, PZA). Maintain ETH alone or use non-hepatotoxic regimen (ethambutol + fluoroquinolone + injectable aminoglycoside) to prevent TB treatment gap.
- After LFT normalisation → sequential re-introduction as above.
Rifampicin drug interactions — key clinical decisions:
- HIV-TB co-treatment: rifampicin induces metabolism of most antiretrovirals (especially protease inhibitors reduce by >90%; NNRTI efavirenz is least affected — dose increase to 800mg in fast metabolisers). Preferred approach: use rifampicin + efavirenz 600mg daily; OR switch to rifabutin (less potent CYP inducer) + lopinavir/ritonavir.
- Oral contraceptives: rifampicin renders standard-dose OCP ineffective — switch to barrier methods or injectable/intrauterine contraception during TB treatment.
- Warfarin: INR will fall within days of starting rifampicin; increase warfarin dose accordingly; monitor INR weekly until stable. INR will rebound when rifampicin is stopped — reduce warfarin dose 2 weeks before stopping rifampicin.
- Steroids (used in TB meningitis, pericarditis, pleural effusion): double the steroid dose while on rifampicin.
Special populations:
- Pregnancy: ATT is safe in pregnancy (first-line HRZE). Rifampicin at term → Vitamin K prophylaxis for neonate (rifampicin induces neonatal liver → neonatal haemorrhagic disease). Streptomycin contraindicated (fetal ototoxicity).
- HIV-TB co-infection: start ATT first (prevent immune reconstitution inflammatory syndrome — IRIS — by waiting 2–8 weeks before starting ART); use INH preventive therapy for latent TB in HIV+ patients.
- Renal impairment: adjust ethambutol and pyrazinamide doses; avoid aminoglycosides if possible; standard doses of INH and rifampicin (hepatic clearance).