Page 17 of 46
PH8.6 | PH8.6 | Leprosy Pharmacotherapy — SDL Guide — SDL Guide
Learning Objectives
- Discuss the types, kinetics, and dynamics of drugs used for leprosy
- Describe the WHO Multi-Drug Therapy (MDT) regimens for paucibacillary and multibacillary leprosy
- Outline the management of Type 1 and Type 2 (ENL) lepra reactions
INSTRUCTIONS
India has the highest leprosy burden globally — approximately 60% of new cases worldwide. Despite the WHO declaring elimination of leprosy as a public health problem in 2005 (defined as <1 case per 10,000 population nationally), pockets of high endemicity persist in states such as Bihar, Uttar Pradesh, Madhya Pradesh, and Maharashtra. The WHO MDT regimen has transformed leprosy from an incurable disfiguring disease to one that is curable in 6–12 months. This SDL focuses on the pharmacological basis of MDT and the critical management of lepra reactions.
References
- Tripathi KD. Essentials of Medical Pharmacology, 8th ed., Ch 57 (textbook)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 13th ed., Ch 58 (textbook)
- WHO Guidelines for the diagnosis, treatment and prevention of leprosy, 2018 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old construction worker presents to a district hospital with hypopigmented anaesthetic patches on his trunk and arms for 3 months. Skin biopsy confirms borderline tuberculoid (BT) leprosy. He is started on paucibacillary MDT (rifampicin + dapsone). Three months into treatment, he returns in distress — the skin patches have become red, swollen, and tender, and he has developed weakness of the right wrist. His family insists he stop the MDT because 'the medicine is making him worse.' What is happening? Is this a drug reaction? Should MDT be stopped? The answers require understanding both the pharmacology of anti-leprosy drugs and the immunopathology of lepra reactions — a crucial distinction that, if missed, leads to withholding treatment from a patient who actually needs both MDT AND immunosuppression.
WHY THIS MATTERS
Leprosy is the world's leading infectious cause of peripheral neuropathy and physical disability, despite being curable. The WHO MDT regimen — introduced in 1982 — has cured over 16 million patients globally. India eliminated leprosy as a public health problem by WHO criteria in 2005, but sub-national pockets and new cases continue to appear. As a clinician, you will encounter leprosy patients throughout your career, particularly in rural postings and community medicine. The stigma associated with leprosy means patients often delay presentation and may stop treatment early — your pharmacological understanding helps you provide confident counselling and manage complications before they cause permanent disability.
RECALL
From prior SDLs: rifampicin — inhibits bacterial RNA polymerase (beta subunit); bactericidal; potent CYP450 inducer (same interactions as in TB); must never be used as monotherapy (rpoB resistance). Dapsone — structurally related to sulfonamides; inhibits dihydropteroate synthase (folate synthesis); bacteriostatic. Clofazimine — riminophenazine dye; used as second-line in MDR-TB Group B.
From Microbiology: Mycobacterium leprae is an obligate intracellular bacterium, exclusively infecting Schwann cells and macrophages; it has the longest doubling time of any pathogen (~13 days); it cannot be cultured in vitro (only in armadillos or mouse footpads). The Ridley-Jopling classification of leprosy ranges from tuberculoid (TT — high CMI, few bacilli) to lepromatous (LL — low CMI, abundant bacilli), with borderline forms (BT, BB, BL) in between.
Leprosy Pathobiology: Why M. leprae Requires MDT
Understanding why leprosy requires multi-drug therapy for 6–12 months (rather than a brief course) follows the same logic as TB: slow organism growth and the mathematical certainty of natural drug-resistant mutants in large bacterial populations.
M. leprae characteristics that determine pharmacotherapy:
- Slowest growth rate of any bacterium (doubling time ~13 days vs 20 minutes for E. coli, 15–20 hours for M. tuberculosis): even bactericidal drugs take months to sterilise tissue; clinical cure requires sustained suppression over the complete MDT course.
- Obligate intracellular habitat: M. leprae lives within Schwann cells (explaining the peripheral neuropathy — demyelination and axonal destruction from direct invasion and immune responses) and macrophages. Drugs must achieve intracellular concentrations: rifampicin and clofazimine penetrate cells well; dapsone achieves adequate intracellular levels for bacteriostatic effect.
- Spectrum of disease reflects host immune response: At the tuberculoid end (TT), the host mounts an effective cell-mediated immune (CMI) response — few bacilli, localised disease, minimal tissue destruction. At the lepromatous end (LL), CMI is suppressed — abundant bacilli, widespread skin infiltration, nodules (lepromata), progressive peripheral nerve destruction. The borderline forms (BT, BB, BL) are immunologically unstable and prone to reactional states (lepra reactions) when the immune balance shifts.
- Dapsone monotherapy history: Dapsone was the sole treatment for decades after its introduction in the 1940s; by the 1970s, widespread dapsone resistance had emerged. This history is the pharmacological rationale for MDT — combining dapsone with rifampicin (bactericidal) and clofazimine prevents resistance amplification by the same combinatorial probability argument as TB treatment.
Therapeutic Goal: Bactericidal Kill, Resistance Prevention, Reaction Management
The three pharmacotherapeutic goals of leprosy MDT are distinct and require specific drug contributions:
1. Bactericidal kill of M. leprae: Rifampicin is the only bactericidal drug in the MDT regimen — it kills the majority of viable M. leprae within the first few days of treatment, rapidly reducing infectivity. Within 3–5 days of starting rifampicin, a patient with MB leprosy is considered non-infectious. This rapid bactericidal action is the reason rifampicin is given as a monthly supervised dose (unlike TB where it is given daily) — monthly pulses still achieve adequate bactericidal effect because M. leprae has such a slow growth rate. Dapsone and clofazimine are bacteriostatic — they slow replication and prevent regrowth but do not rapidly kill.
2. Resistance prevention: Adding dapsone (and clofazimine in MB leprosy) to rifampicin ensures that any M. leprae with spontaneous rifampicin-resistance mutations are killed by the bacteriostatic drugs, and vice versa. This is the combinatorial resistance-prevention strategy applied to leprosy.
3. Immunological reaction management: Lepra reactions (Type 1 and Type 2 — see below) are immunopathological events that occur during — and sometimes after — MDT. They are NOT drug side effects and must NOT trigger withdrawal of MDT. Rather, they require specific immunosuppressive pharmacotherapy (corticosteroids for Type 1; thalidomide or clofazimine for Type 2) alongside continued MDT. Failure to recognise reactions and treat them appropriately leads to permanent nerve damage and disability.
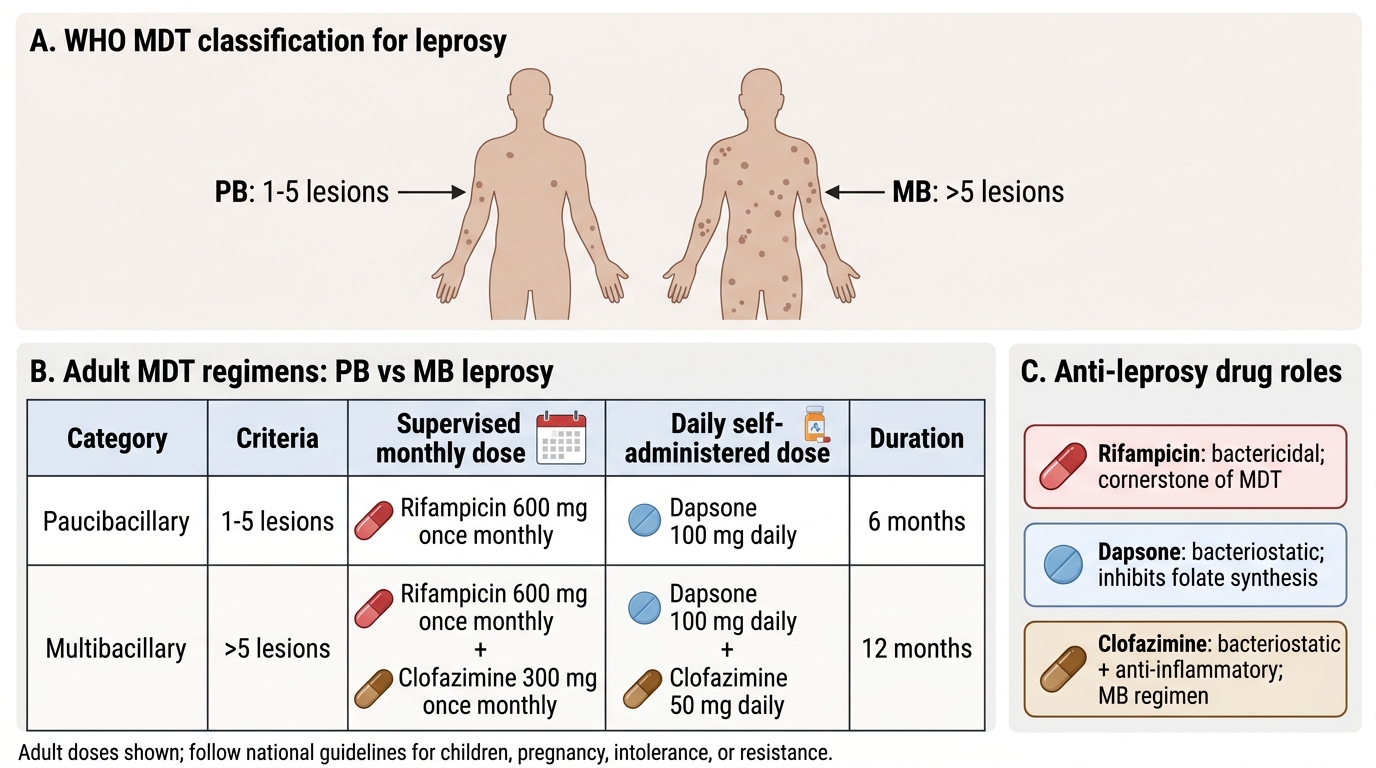
PB vs MB Leprosy MDT Regimens
Anti-Leprosy Drug Classification
Anti-leprosy drugs are classified by their role in MDT and their mechanism of action:
First-line MDT drugs (WHO-recommended):
- Rifampicin — bactericidal; supervised monthly dose (600mg); the cornerstone of MDT
- Dapsone — bacteriostatic; daily self-administered dose (100mg); inhibits folate synthesis
- Clofazimine — bacteriostatic and anti-inflammatory; supervised monthly dose (300mg) + daily self-administered dose (50mg); used in MB leprosy only
Second-line (alternative) drugs (for MDT drug intolerance or resistance):
- Ofloxacin (or other fluoroquinolones) — bactericidal; can substitute for rifampicin if rifampicin cannot be used
- Minocycline (tetracycline class) — bactericidal against M. leprae; substitutes for dapsone or clofazimine
- Clarithromycin (macrolide) — moderate anti-leprae activity; used in combination with ofloxacin + minocycline when full MDT is not tolerated
Single-dose ROM regimen (ROM = Rifampicin + Ofloxacin + Minocycline): Used for single-lesion paucibacillary leprosy (1 skin lesion). A single oral dose of rifampicin 600mg + ofloxacin 400mg + minocycline 100mg was shown in Indian trials to achieve equivalent 2-year relapse rates to the standard 6-month PB MDT regimen for this specific clinical presentation. Used by the NLEP (National Leprosy Elimination Programme) as a convenient single-visit treatment for confirmed single-lesion PB cases.