Page 18 of 46
PH8.6 | PH8.6 | Leprosy Pharmacotherapy — SDL Guide — SDL Guide (Part 2)
Dapsone, Rifampicin, and Clofazimine: PK, ADRs, Clinical Use
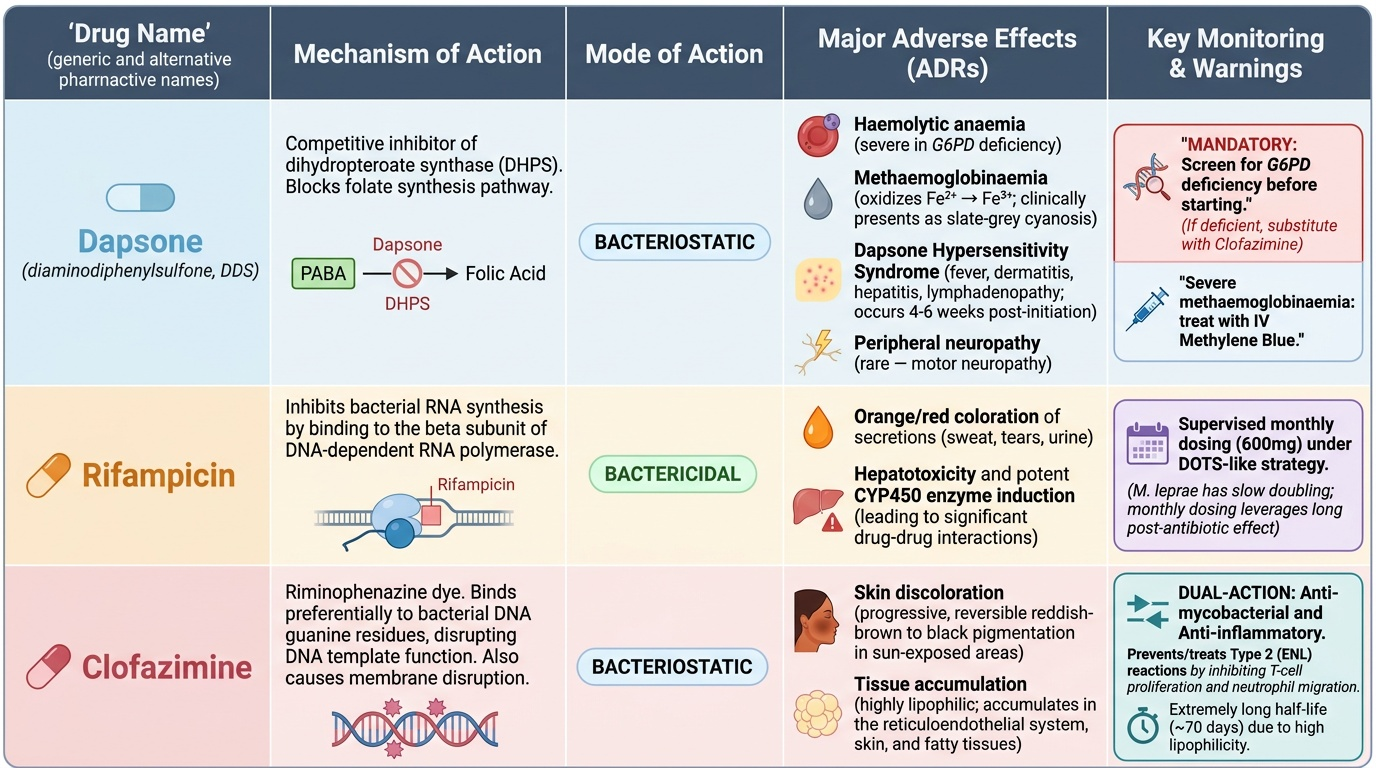
Dapsone (diaminodiphenylsulfone, DDS):
- Mechanism: competitive inhibitor of dihydropteroate synthase — the same enzyme inhibited by sulfonamides — blocking folate synthesis. Bacteriostatic against M. leprae.
- PK: well-absorbed orally; hepatic acetylation (slow/fast acetylators — similar NAT2 polymorphism to INH); enterohepatic recirculation; long half-life (~28 hours).
- ADRs: (a) Haemolytic anaemia — the most common serious adverse effect; mild haemolysis occurs in virtually all patients taking dapsone (Heinz body formation from oxidative stress on erythrocytes); severe haemolytic anaemia in G6PD-deficient patients (G6PD protects red cells from oxidative stress — its absence makes dapsone haemolysis catastrophic). Screen for G6PD deficiency before starting dapsone; if G6PD deficient, substitute with clofazimine. (b) Methaemoglobinaemia — dapsone oxidises haemoglobin iron (Fe²⁺ → Fe³⁺), producing methaemoglobin (does not bind O2); mild in most patients; severe in G6PD deficiency. Clinically: slate-grey cyanosis unresponsive to oxygen — treat with IV methylene blue 1–2mg/kg. (c) Dapsone hypersensitivity syndrome (rare but serious): fever, dermatitis, lymphadenopathy, hepatitis — occurs 4–6 weeks after initiation. Stop dapsone; treat with corticosteroids. (d) Peripheral neuropathy (rare — motor, unlike INH sensory neuropathy).
Rifampicin:
- Same mechanism and drug interactions as in TB (RNA polymerase beta subunit; CYP450 inducer; orange secretions). In leprosy MDT, it is given as a supervised monthly dose (600mg) rather than daily — adequate for M. leprae (slow doubling time; rifampicin post-antibiotic effect lasts weeks). Monthly dosing simplifies supervised delivery under DOTS-like strategy.
Clofazimine:
- Mechanism: a riminophenazine dye that binds preferentially to mycobacterial DNA (guanine residues), disrupting DNA template function. Also has direct membrane-disrupting activity. Bacteriostatic against M. leprae. Additionally, clofazimine has anti-inflammatory and anti-ENL properties (inhibits T-cell proliferation and neutrophil migration) — making it uniquely dual-purpose: treating the infection AND preventing/treating Type 2 (ENL) reactions.
- PK: highly lipophilic; accumulates in skin, reticuloendothelial system, fatty tissues (large Vd); very long half-life (~70 days); slowly released from tissue stores → leprosy bacilli are exposed to drug long after each dose.
- ADRs: (a) Orange-brown to reddish-brown discolouration of skin, eyes, urine, and body fluids — more pronounced in darker-skinned individuals; sometimes called 'drug-induced racial depigmentation'; this is predictable and harmless but cosmetically distressing. Must warn patients before starting — failure to do so causes treatment abandonment, particularly in lighter-skinned patients. Discolouration reverses slowly (over 6–12 months) after stopping clofazimine. (b) GI adverse effects — nausea, diarrhoea, abdominal pain; take with food; crystal deposition in intestinal wall with high doses. (c) Dryness and ichthyosis of skin (from fat-soluble storage).
Provided image
SELF-CHECK
A patient with multibacillary leprosy on WHO MDT (rifampicin + dapsone + clofazimine) has G6PD deficiency discovered on pre-treatment screening. Which modification to the MDT regimen is most appropriate?
A. Stop all MDT — G6PD deficiency is an absolute contraindication to leprosy treatment
B. Continue all three drugs with additional pyridoxine supplementation to protect red blood cells
C. Substitute dapsone with clofazimine — use clofazimine + rifampicin + ofloxacin or minocycline
D. Reduce dapsone dose to 50mg daily — halving the dose eliminates haemolytic risk in G6PD deficiency
Reveal Answer
Answer: C. Substitute dapsone with clofazimine — use clofazimine + rifampicin + ofloxacin or minocycline
Dapsone causes haemolytic anaemia via oxidative red cell damage; in G6PD-deficient patients, who lack the enzyme that regenerates reduced glutathione to protect red cells from oxidative stress, dapsone-induced haemolysis can be severe and life-threatening. Dapsone should be substituted with an alternative bacteriostatic agent. For MB leprosy, replacing dapsone with clofazimine (already in the regimen at the bacteriostatic level) plus adding a fluoroquinolone (ofloxacin) or minocycline provides adequate coverage. Pyridoxine does not protect against oxidative haemolysis (it prevents INH-induced neuropathy via a different mechanism). Halving the dapsone dose does not adequately protect a G6PD-deficient patient.
WHO MDT Regimens: PB and MB Leprosy
Provided image
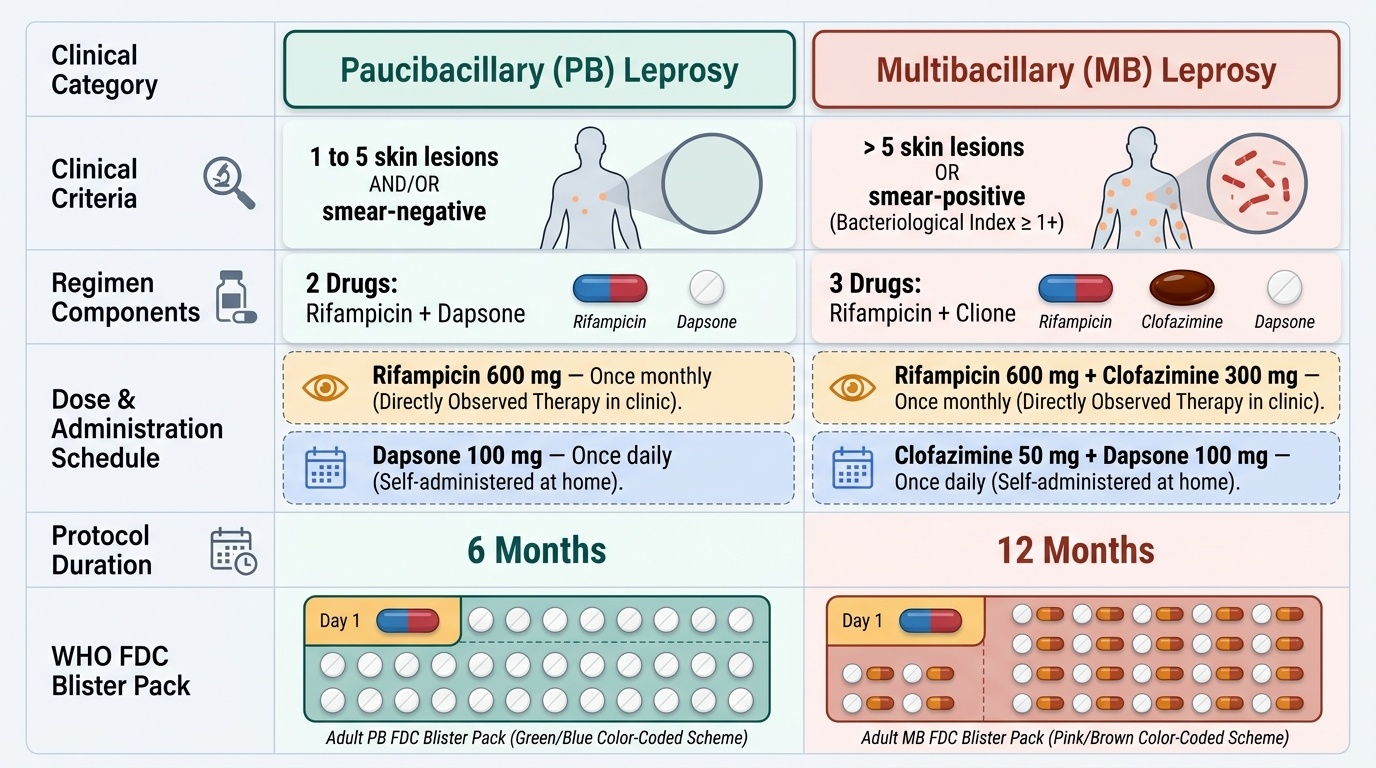
The WHO MDT regimens are designed around two clinical categories based on bacterial load:
Paucibacillary (PB) Leprosy: 1–5 skin lesions AND/OR smear-negative. Bacterial load is low; fewer drugs needed.
- Regimen: Rifampicin 600mg once monthly (supervised) + Dapsone 100mg daily (self-administered)
- Duration: 6 months
- Rationale: rifampicin bactericidal monthly dose; dapsone bacteriostatic daily dose suppresses regrowth between rifampicin doses; 6 months sufficient for paucibacillary disease to sterilise
Multibacillary (MB) Leprosy: >5 skin lesions OR smear-positive (Bacteriological Index ≥1+). Bacterial load is high; three drugs needed.
- Regimen: Rifampicin 600mg once monthly (supervised) + Clofazimine 300mg once monthly (supervised) + Clofazimine 50mg daily (self-administered) + Dapsone 100mg daily (self-administered)
- Duration: 12 months
- Rationale: addition of clofazimine addresses the higher bacterial load and its unique anti-inflammatory property covers ENL tendency in MB disease. Previously 24 months (pre-1997 WHO guidelines); shortened to 12 months based on evidence from multi-site trials showing equivalent relapse rates.
Fixed-dose combination (FDC) blister packs: The WHO supplies MDT as pre-packaged blister packs — one pack per month; adult PB pack (1 supervised capsule + 28 daily capsules); adult MB pack (1 supervised capsule + 28 pairs of daily capsules). This eliminates the need for individual drug dispensing and prevents selective non-compliance. Available free under the National Leprosy Elimination Programme (NLEP) in India.
Single-dose ROM (rifampicin 600mg + ofloxacin 400mg + minocycline 100mg): Reserved for single-lesion PB leprosy (exactly 1 skin lesion) — one visit, one dose, cure rates comparable to 6-month PB MDT at 2-year follow-up.
Outcome monitoring: Skin lesions should begin to improve after 3 months; complete clearing of skin changes may take 1–2 years after MDT (even after bacterial sterilisation). Nerve function monitoring is required — nerve function impairment (NFI) is the key preventable disability outcome.
SELF-CHECK
A patient with borderline tuberculoid (BT) leprosy on PB MDT develops sudden onset wrist drop (inability to extend the wrist) at month 4 of treatment. He has no new skin lesions and the existing patches are clearing. What is the most likely diagnosis and the appropriate immediate management?
A. Dapsone-induced peripheral motor neuropathy — stop dapsone and complete MDT with rifampicin alone
B. Type 1 lepra reaction with acute nerve damage — continue MDT and start prednisolone immediately
C. Rifampicin-induced peripheral neuropathy — this is a known complication of supervised monthly dosing
D. Treatment failure — the patient has developed drug-resistant leprosy and needs second-line drugs
Reveal Answer
Answer: B. Type 1 lepra reaction with acute nerve damage — continue MDT and start prednisolone immediately
Wrist drop (sudden-onset nerve function impairment) at month 4 of PB MDT in a borderline leprosy patient is a Type 1 (Reversal) reaction — an immunological upgrading reaction driven by enhanced T-cell-mediated immunity (CMI) against M. leprae antigens. This is NOT a drug side effect. Type 1 reactions occur characteristically in borderline leprosy (BT, BB, BL) as the immune system mounts a stronger response during MDT. Nerve involvement (acute neuritis, sudden neuropathy) is the most dangerous feature — if untreated, it causes permanent nerve damage and disability. Immediate treatment: prednisolone 40mg/day PLUS continue MDT without interruption. Stopping MDT is the wrong response — the reaction is immunological, not drug-toxic.
Lepra Reactions: Type 1, Type 2, and Their Management
Lepra reactions are acute inflammatory episodes that occur in the context of leprosy — before, during, and sometimes after MDT. They are NOT drug adverse effects; they are immunopathological events caused by the host's immune response to M. leprae antigens. Understanding their mechanisms determines the correct treatment.
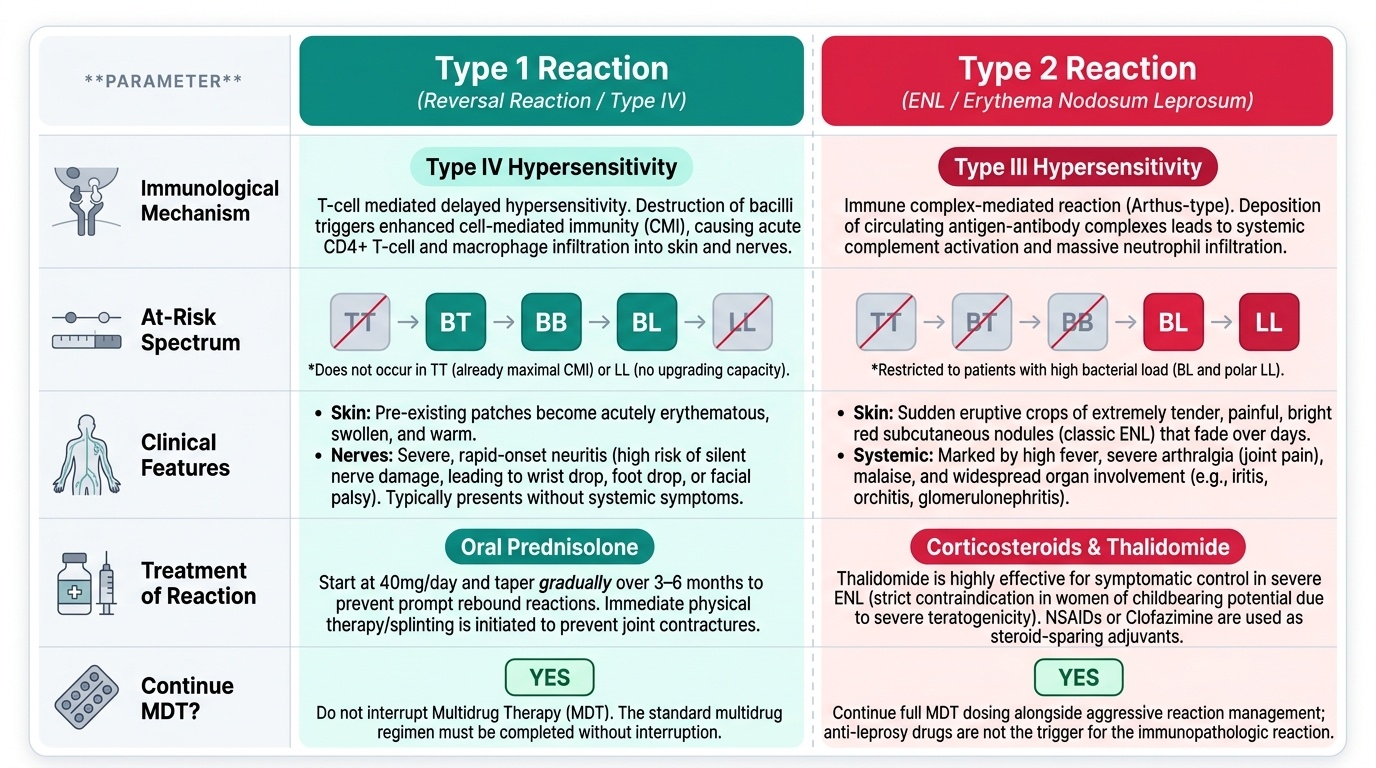
Type 1 Reaction (Reversal Reaction):
- Immunological mechanism: Type IV hypersensitivity (T-cell mediated). During MDT, dying mycobacteria release large quantities of antigen → enhanced cell-mediated immune (CMI) response → T-cell and macrophage infiltration into skin and nerves → inflammation.
- Which patients: Borderline leprosy — BT, BB, BL. Does NOT occur in tuberculoid (TT — already has maximal CMI, no upgrade possible) or lepromatous (LL — minimal CMI, no upgrading capacity).
- Clinical features: Pre-existing skin patches become erythematous, oedematous, and tender. New patches may appear. Acute peripheral neuropathy is the most dangerous feature — sudden wrist drop, foot drop, facial palsy from acute inflammation of involved nerves. May occur during MDT or after treatment completion (up to 5 years post-MDT — 'late reversal reaction').
- Management: Prednisolone 40mg/day orally, tapered gradually over 3–6 months (rapid tapering causes relapse of reaction). Continue MDT throughout — do not stop. Refer to NLEP district centre for nerve function monitoring. Physical therapy to prevent contractures.
Type 2 Reaction (Erythema Nodosum Leprosum — ENL):
- Immunological mechanism: Type III hypersensitivity (immune complex mediated — IgM immune complex deposition in skin and other organs → complement activation → neutrophil infiltration → inflammation).
- Which patients: LL (lepromatous) and BL (borderline lepromatous) leprosy — high antigen load + high antibody titres = immune complex formation. Does NOT occur in tuberculoid forms (insufficient antigen).
- Clinical features: Crops of tender erythematous nodules on the extensor surfaces and face (clinically different from Type 1 — the patches are new nodular lesions, not pre-existing patches becoming inflamed). Systemic features: fever, malaise, arthritis, iritis, orchitis, lymphadenopathy, nephritis. ENL can be severe and recurrent.
- Management: (a) Thalidomide 100–300mg/day — the most effective drug for ENL; works by inhibiting TNF-α production and neutrophil chemotaxis (immunomodulatory). Strictly contraindicated in females of childbearing potential (causes phocomelia — severe fetal limb reduction defects — the original thalidomide disaster). In India, thalidomide is available under the NLEP for male patients and post-menopausal/sterilised women with documented consent and contraception. (b) Clofazimine 200–300mg/day — anti-inflammatory property makes it safer than thalidomide for ENL, especially in fertile women; drug of choice for ENL in females of childbearing potential. (c) Prednisolone — for mild-moderate ENL and for acute neuritis associated with ENL; less effective than thalidomide for severe/recurrent ENL. Continue MDT throughout ENL reactions.
Provided image
SELF-CHECK
A 28-year-old woman with lepromatous (LL) leprosy on MB MDT develops crops of painful erythematous nodules on her arms and legs, with fever and joint pains. ENL is diagnosed. Thalidomide is suggested. What is the most important consideration before prescribing thalidomide?
A. Check renal function — thalidomide is predominantly renally cleared and causes nephrotoxicity at standard doses
B. She is a woman of childbearing potential — thalidomide is absolutely contraindicated and clofazimine should be used instead for ENL management
C. Confirm she is not taking corticosteroids — thalidomide and corticosteroids interact to cause severe immunosuppression
D. Check platelet count — thalidomide causes severe thrombocytopaenia as its primary adverse effect in women
Reveal Answer
Answer: B. She is a woman of childbearing potential — thalidomide is absolutely contraindicated and clofazimine should be used instead for ENL management
Thalidomide is absolutely contraindicated in women of childbearing potential (pregnancy category X). Thalidomide's mechanism of teratogenicity — inhibition of angiogenesis during fetal limb bud development — causes phocomelia (severe limb reduction defects). This is the drug's historical toxicity that led to the thalidomide tragedy in the 1950s-60s. For ENL in fertile women, clofazimine at higher doses (200–300mg/day, subsequently tapered) is the preferred alternative — it has anti-inflammatory properties and is safe in pregnancy (B category). Thalidomide can be used in post-menopausal women and men under strict REMS (Risk Evaluation and Mitigation Strategy) conditions. Renal toxicity and thrombocytopaenia are not the primary concern here.